Article Text

Statistics from Altmetric.com
Pneumococcal disease is endemic all over the world. Epidemics may occur, most often in closed institutional settings such as schools and military camps,1-3 but account for only a minority of all the cases. The total incidence of pneumococcal pneumonia in Western populations is 1–5 per 1000 person-years, and several times higher in the very young and the elderly. In developing countries it is estimated that at least one million children below the age of five die each year from pneumococcal pneumonia.4 Streptococcus pneumoniae is also the most important pathogen in bacterial meningitis, otitis media, and sinusitis. The annual incidence of pneumococcal bacteraemia in North America and Europe is at least 10–20 per 100 000 individuals, the majority of cases being due to pneumonia. However, the most common host-parasite interrelationship is the asymptomatic carriage of one (or occasionally two or more) pneumococcal strains in the nasopharynx.5 6
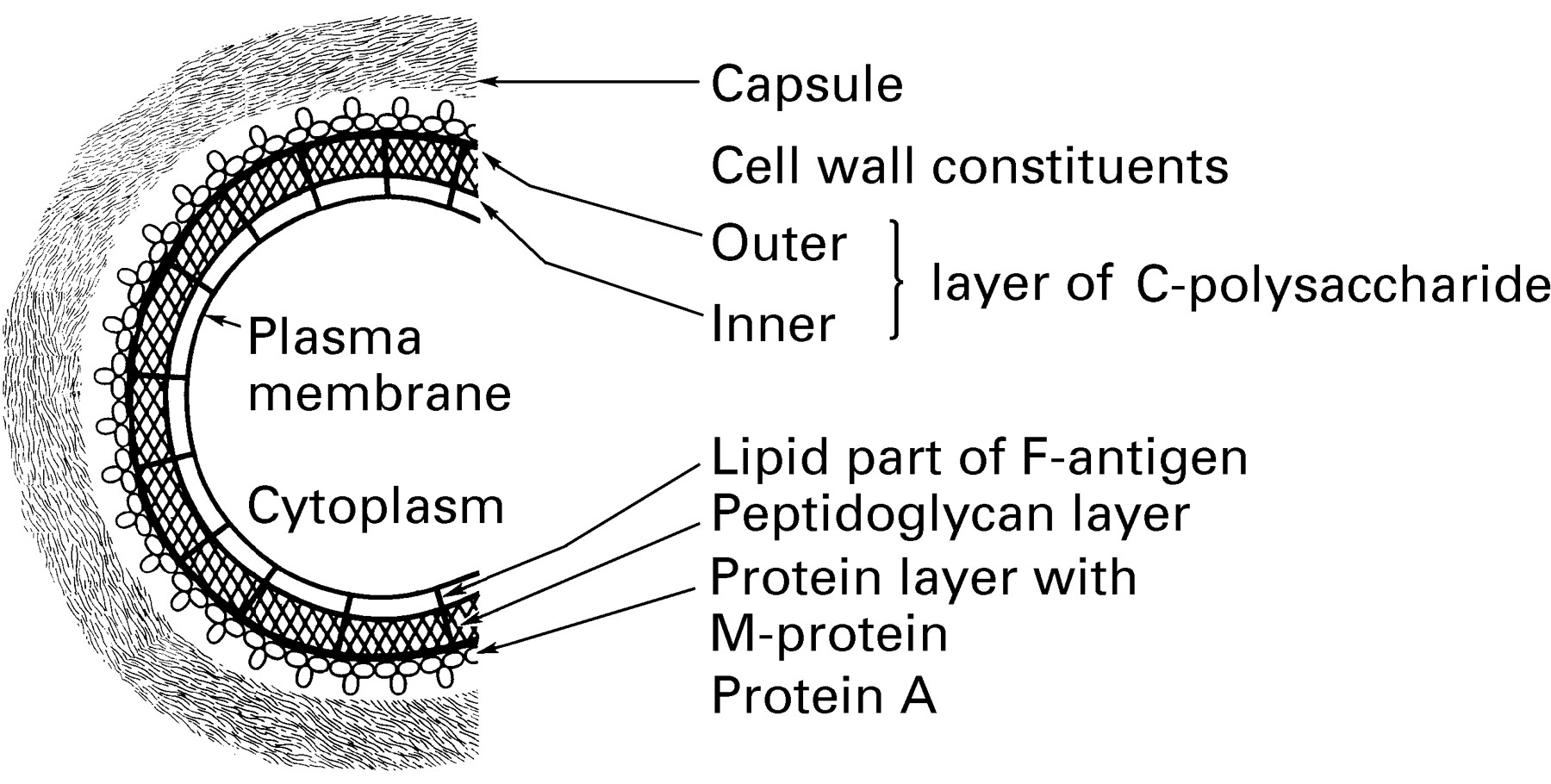
As in other Gram positive bacteria, the pneumococcal cell wall is composed of peptidoglycan and teichoic acid (fig 1). A predominant component of teichoic acid is the C-polysaccharide which is covalently bound to the peptidoglycan layer and distributed both on its inner and outer side.7 The exact chemical structure of the C-polysaccharide has been established as a ribitol teichoic acid containing glucose, 2-acetamido-2,4,6-trideoxygalactose, galactosamine, ribitol phosphate, and phosphorylcholine.8 Interestingly, each of these components has been identified as constituents of different capsular polysaccharides, possibly pointing to an evolutionary origin of the capsular substances from the C-polysaccharide.

Schematic illustration of the arrangement of the pneumococcal cell wall.
The capsule
All wild strains of Streptococcus pneumoniae are provided with a polysaccharide capsule. To date, 90 distinct capsular types have been described, six of them very recently.9Some of the types are antigenically related to each other and such related types are included together in groups—for example, 9A, 9L, 9N and 9V—while types without a close antigenic relationship to other types are given numbers only—for example, types 1, 2, 3, 4, 5. All of the six recently described types are antigenically related to previously known types. The capsular polysaccharides are composed of repeating units of oligosaccharides and for most of them the exact chemical structure is known.10 The extent of cross-reactivity between types within the respective groups may differ—for example, types 6A and 6B have identical chemical composition except for one of the bonds between two sugars and are extensively cross-reactive9 11 while types 19F and 19A are clearly less cross-reactive. This has been illustrated in a chinchilla model of otitis media in which a polysaccharide vaccine including types 6B and 19F conferred protection against otitis with types 6B as well as 6A, and against 19F but not 19A.12
Molecular analysis of the genes responsible for the synthesis of some of the capsular substances has recently shown that they are arranged in cassettes comprising all the genetic material necessary for capsule synthesis.13 14 The pneumococcus, as well as several other streptococci, is naturally transformable which means that genetic material may be exchanged between different strains. By such a process the capsule specificity, in a cassette type recombination event, can be exchanged in vitro as well as in vivo.13 14 Capsule transformation was known as early as 192815 and has recently been noted on several occasions in antibiotic resistant clones.16 17 Occasionally pneumococcal strains may contain both of two different polysaccharide coding gene cassettes at the same time.13 14 It has been suggested that further recombination events in such strains may form novel capsule types.15
It has been known since the beginning of the century that the polysaccharide capsule is crucial for virulence.15 18 19Although pneumococcal capsular polysaccharides have been found to be non-toxic when injected into laboratory animals as pure substances, it was recently shown that different capsular types caused substantially different inflammatory responses in a rabbit model of meningitis: types 5 and 7F exhibited mild inflammatory responses, type 1 an intermediate response, and types 6B, 14 and 23F a severe response.20The mechanisms are not entirely clear, however. The often dramatic toxic symptoms of a pneumococcal infection are otherwise thought to be primarily caused by soluble or cell wall products such as peptidoglycan, C-polysaccharide, pneumolysin, neuramidases, autolysin, hyaluronidase, and surface adhesin.15 18 19Interruptions of genes encoding for these proteins have also been shown to attenuate virulence to some degree. The physical removal of the pneumococcal capsule or the interruption of encapsulation genes, however, completely abolishes virulence.19
The most important mechanism by which the capsule promotes virulence is probably by protecting the bacteria against immediate ingestion by animal phagocytes. A substantially thicker capsule may therefore confer more protection against phagocytosis.18 The chemical composition of the capsule is, however, far more important. The binding of type-specific anticapsular antibodies to the capsule changes the structure of the cellular surface so that phagocytosis is facilitated and a functioning antibody response is crucial in the defence against pneumococcal infections. The capsule is normally the only exposed antigen with the cell wall antigens concealed by the capsular material.7 All the same, an antibody response is elicited against several other structures of the pneumococcus such as the C-polysaccharide and the pneumolysin. However, only antibodies directed against the capsular polysaccharide have been shown to have a protecting role.18 21 Thus, a highly significant relationship can be demonstrated between opsonisation and pneumococcal antibody levels which is almost abolished by adsorption of capsular polysaccharide antibodies but is not affected by removal of cell wall antibodies.22 In fact, it has been shown that the risk of developing pneumonia with a certain serotype is very small in the presence of type-specific antibody.21 Moreover, in a recent study of outbreaks of pneumococcal pneumonia in military camps, serotype-specific antibody was present in about one third of the soldiers who did not contract pneumonia and developed as a result of nasopharyngeal colonisation in another third.3Nasopharyngeal carriage seems to be of crucial importance for developing immunity to S pneumoniae.5 21 23
As the capsular substances are pure polysaccharides they are T cell independent antigens which implies that there may be an antibody response after contact with a particular polysaccharide, but no immunogenic memory and no booster response upon new contact with the same polysaccharide.18 T cell independent antigens also elicit a poor antibody response in small children with their immature immune system, particularly the weak or absent IgG2response. An adult type of antibody response is acquired gradually and differently for different types. Against some of the capsular polysaccharides—notably 6A, 14, 19F, and 23F—a mature antibody response is recorded only at the age of five years or even later.11 24 As a consequence, these types most often predominate in nasopharyngeal childhood carriers.5 11 25-26 27
Serotype prevalence
Most, if not all, serotypes are capable of causing serious disease in humans. Three recent studies illustrate this fact. Of 5619 strains isolated from patients with serious pneumococcal infections in Belgium, 64 different types were identified.28 In a combined study of 13 different data records from different countries comprising 7010 episodes of invasive pneumococcal disease, all but four of 46 serogroups were identified.25 Finally, in a study of 10 298 strains from mostly European patients with invasive pneumococcal disease, 77 of the then known 84 types were identified.29Moreover, all of the six recently described types were found in patients with bacteraemia or meningitis.9 Although all capsular types may thus be involved in pneumococcal disease at some time, the frequency with which different types are isolated is different. Most of the capsular types have been isolated in very low frequencies since the beginning of this century, when different types were first identified, indicating that these polysaccharides confer a low grade of virulence on the pneumococcal cell.11 15 18
In the most comprehensive analysis so far, a total of 13 616 different pneumococcal strains isolated from patients with invasive infections in several countries around the world were typed with both group and factor (type) sera.11 The data from types 6A and 6B, as well as those from 15B and 15C, were combined due to their extensive cross-reactivity. Figure 2 clearly illustrates the uneven prevalence of pneumococcal serotypes. Type 14, which was the most prevalent type, accounted for 9% and types 4, 1, and 3 for 7–8% each. Types 6A and 6B together accounted for 8%. If they are considered as two distinct types the 10 most prevalent ones together made up 61.7% and the 30 most prevalent types accounted for 91.5%. Since the recently detected six types have a very low prevalence, it can be deduced that in this material 69 of the 90 known types had a relative prevalence of <1% and the least common 60 types accounted for only 8.5%—that is, less than type 14 alone. This study provided the basis for formulating the current 23-valent polysaccharide vaccine which has subsequently been shown to confer about 70% protection against invasive pneumococcal disease with vaccine types in immunocompetent adults.30 31 There is no protection against non-vaccine types.

{kind=link}
{kind=link}
Type distribution among 13 616 pneumococcal strains isolated from patients with invasive infections in several different countries worldwide. Modified from reference 11.
In table 1 two large samples of pneumococcal strains from preschool children and from older individuals are compared. These strains were collected by the Center for Disease Control and Prevention in the USA, approximately during the same time period and only from blood or cerebrospinal fluid specimens.27 31 As can be seen, there is a marked difference between the two age groups with types 14, 6B, 19F, and 18C being much more prevalent in small children. In adults the type distribution pattern is more even. This is also illustrated by the fact that the seven most frequent types were responsible for 80% of the invasive infections in small children, but for only 55% in older individuals. The findings were similar in a large, mostly European, study comprising more than 10 000 strains.29 In another recent study by Scott et al 25 involving 7010 strains from invasive infections in all ages from several Western as well as several developing countries, these findings were further extended. The risk of infection was, as in other studies, found to be much higher in children below five years of age and in the elderly. However, in addition to this general age dependent difference in incidence, it was found that types/groups 6, 14, and 19 were, in comparison with other types, unusually common in childhood, but also associated with an exceptionally abrupt reduction in prevalence beyond the first decade of life; the same effect, but more gradual, was seen with groups 23 and 18, while the relative importance of types 3 and 8 was, in contrast, found to increase after middle age.25
Percentage of different types of S pneumoniae causing invasive disease in persons aged <6 years and those aged ⩾6 years
In the study by Scott et al it was also found that serogroups associated with higher nasopharyngeal prevalence—for example, 19 and 23—were relatively more common in Europe and North America, while the invasive serotypes 1 and 5 were much more common in South America.25 In another study the serogroup or serotype distributions among strains isolated from invasive or lower respiratory tract infections in children in 16 different countries were compared (table 2).32 Type 14 was the most frequent type in total, with high prevalences in both developed and developing countries. However, very substantial differences were seen with 27% and 29% of the isolates in USA and Belgium, respectively, being type 14 but only 3% in Spain. Similarly, this type was responsible for 40% and 32% of the infections in Uruguay and the Gambia, respectively, but for only 1% of the infections in Pakistan. Also, groups 6 and 19 were common in both developed and developing countries, again with remarkable differences between the different countries. Serotypes 2, 3, and 4 were relatively uncommon in all countries. Types 1 and 5 are the most interesting types being common only in several of the developing countries. Together they accounted for 40%, 37%, and 36%, respectively, in Israel, Rwanda and Egypt. In accordance with this, types 1 and 5 together were responsible for 50% of the pneumococcal infections in West Africa in the 1970s.33 Type 2 in this study accounted for 6%.
Serotype/group prevalence in children in different countries
Thus, type 14 has been the most (or one of the most) frequent types encountered in several recent surveys and has generally been found more frequently in children. In the CDC study referred to above27 it was found that, over a period of 16 years, a doubling of the isolation frequency of type 14 was seen, while types 3 and 18C decreased. Similar changes have been noted in Belgium. In an analysis of 5619 mostly invasive pneumococcal infections it was found that type 3 steadily decreased from >16% in 1980 to <5% in 1993, while there was an increase of the same magnitude in types 14 and 23.28 Also in Sweden,34Finland,35 and Denmark26 a decrease in type 3 has been noted. However, in Sweden an accompanying increase in type 14 was especially pronounced in the elderly, in whom it now accounts for almost one quarter of the invasive infections.33
Interestingly, in the USA and Europe in the beginning of the 20th century types 1 and 2 accounted for up to 65% of the cases of lobar pneumonia and types 1, 2, and 3 together for up to 75% of the bacteraemic cases (table 3).15 18 36 37 Type 5 was also common. Today types 2 and 5 are almost never isolated in Western countries and type 1 occurs usually with a frequency well below 10%.11 26-29 These changes in the relative importance of different pneumococcal types have taken place in a remarkably similar way in most Western countries. At the same time, the type distribution pattern in developing countries is often similar to that seen in the USA and Europe at the beginning of the century with a few types predominating, particularly types 1 and 5. However, type 2 has been uncommon in all geographical regions for several decades. Type 3, on the other hand, has been one of the most important types during most of the 20th century, but is now decreasing in frequency in most studied areas. The changes seen during this century and the type distribution pattern seen in different countries today may indicate a different susceptibility to different capsular polysaccharides in hosts living under different socioeconomic circumstances. Types 1, 2, 3, and 5, in comparison with other types, are more immunogenic and have been isolated less often from carriers and seem to have a more pronounced tendency to spread epidemically.18 It may be speculated that, in overcrowded living conditions with poverty, exposure to active cases of pneumococcal disease may be more prevalent, while in Western countries small children who are asymptomatic carriers are the predominant source from which spread of pneumococci occurs.
Percentage of types 1, 2, and 3 in lobar pneumonia in the beginning of the 20th century
Nasopharyngeal carriage of pneumococci is especially frequent in small children, particularly those staying in day care centres and other crowded settings. It most often implies colonisation with a single or a few serotypes at a time for a few weeks or months.5 38 39 Small children are often treated with antibiotics and this is probably why antimicrobial resistance toS pneumoniae has developed primarily in types/groups 6, 14, 19, and 23 which are prevalent in young children.40Moreover, the selective pressure of antibiotics seems to have an impact on the spectrum of serotypes. In Israel the prevalence of penicillin resistance in invasive pneumococcal isolates increased from 16% to 36% from 1987 to 1992, and during this observation period the seroprevalence of types/groups 6, 14, 19, and 23 increased from 37% to 62%.41
The existing pure polysaccharide vaccine does not confer protection in small children who have a high incidence of severe pneumococcal disease, not the least in developing countries. Moreover, there is no protection against childhood carriage and thus this vaccine cannot be used to reduce the prevalence of antibiotic resistant strains. In order to improve the vaccine, pneumococcal polysaccharides have been coupled to suitable carrier proteins to convert them into protein antigens in the same way as has been done with the Haemophilus influenzae type b polysaccharide. With such conjugates an antibody response can also be elicited in children of a few months of age.42-44 Moreover, an immunogenic memory and a booster effect upon revaccination is obtained. Interestingly, as has been the case with the H influenzae conjugate vaccines, the pneumococcal conjugate vaccines seem also to reduce the carrier frequency in vaccinated children. In one study colonisation with vaccine types one month to one year after vaccination with a heptavalent vaccine was reduced from 25% to 4–9%.43 No effect was seen on non-vaccine types nor with a pure polysaccharide vaccine. The main problem with the pneumococcal conjugate vaccines is that only a limited number of types may be included. In a very recent report44 a substantial reduction in colonisation frequency with vaccine types was accompanied by an increase in non-vaccine types of the same magnitude. The importance of this finding from a disease protection point of view is at present unknown. Moreover, there may be a risk that resistant genes are transferred to such new colonising types. The total effect on disease incidence and the frequency of antibiotic resistance is therefore impossible to estimate at the present time.
Conclusions
The pneumococcal polysaccharide capsule is crucial for virulence, primarily by protecting the bacteria against phagocytosis. Ninety different types have been described but their capability to cause serious disease is different and most of them are uncommon. Major shifts in prevalence have been noted over time among more frequent types, although the patterns may differ between Western and developing countries. Types 1, 2, 3, and 5 are more immunogenic and are less often isolated from carriers, but seem to have a greater tendency to spread epidemically. Types/groups 14, 6, 19, and 23 are more prevalent in young children who are often asymptomatic nasopharyngeal carriers. In this age group antimicrobial resistance has developed frequently, probably as a result of frequent antibiotic usage in type 14, 6, 19, and 23 clones, some of which have achieved extensive geographical spread. Capsular gene cassette transformation, leading to a change in the capsule specificity, is a common event in such antibiotic resistant clones, and possibly also in more natural clones. This phenomenon may influence the protective efficacy of conjugate vaccines as well as their ability to reduce the prevalence of resistant pneumococcal clones. Moreover, the use of these vaccines seems to imply a risk for significant shifts in type prevalences among carriers. It will therefore be important to follow the type distribution in regions with and without vaccine usage, and to study the epidemic characteristics and the tendency to emergence and spread of antibiotic resistant clones among common and uncommon types.