Article Text

Statistics from Altmetric.com
There are around 1.1 thousand million smokers in the world which is approximately one third of the global population who are aged 15 years and over (47% of men and 12% of women).1 Most smokers live in developing countries (800 million) and most are male (700 million).1 While smoking rates have decreased in developed countries over the last 13 years, there has been a corresponding 50% increase in smoking rates in developing countries.2
The most important determinant of human health trends is the increase in tobacco related mortality and disability. Tobacco related deaths have been projected to increase from 3.0 million in 1990 to 8.4 million in 2020, which will make tobacco the largest single health problem at this time.3 There are 80–90% of deaths from chronic obstructive lung disease attributed to tobacco, and smokers have six times the risk of contracting this disease compared with smokers; similarly, 80–85% of lung cancer deaths are attributed to tobacco use, with smokers having 10 times the risk compared with non-smokers.4-6
National and international responses to the public health problem of tobacco therefore need to be intensified. Primary care physicians have a vital role to play in advising patients to stop smoking as most smokers visit their doctor.7-9 Studies have shown that very brief advice from the doctor yields one year quit rates of 5–10%,10-12 and interventions that are more comprehensive, including follow up sessions, produce abstinence rates of 20–36%.13-15
Another important way to control tobacco use is to encourage medical schools to teach about tobacco issues in the curriculum. It is vital that medical students, the future medical practitioners, have adequate knowledge of smoking related diseases and skills in smoking cessation. The purpose of this paper is to review the literature on medical students’ smoking rates, knowledge of tobacco related diseases and skills in smoking cessation, and to determine the extent of teaching about tobacco in medical schools. A teaching programme for implementation in the medical curriculum is then described.
Prevalence of smoking in medical students
There have been many studies conducted around the world to determine the smoking rates of medical students and their knowledge of smoking related diseases and intervention strategies. The Tobacco Prevention Section of the International Union Against Tuberculosis and Lung Disease (IUATLD), a committee of representatives from many countries concerned with tobacco control and prevention, has conducted a series of studies in medical schools globally. The studies were joint collaborations between the IUATLD, the World Health Organization (WHO), the American Cancer Society, and the International Union against Cancer. The surveys were conducted among more than 9000 students from 51 medical schools in 42 countries.16 ,17 The objectives were to determine the smoking rates of medical students; to ascertain medical students’ knowledge of smoking as a major cause of disease; and to determine whether students believed they can counsel patients about smoking. Additionally, many medical schools have conducted surveys among their student populations.
Table 1 shows that the smoking rates of medical students range widely from 0 to 56.9% for men and 0 to 44.7% for women. Overall, smoking was less prevalent in Asian medical schools than in European schools.25 ,40 Smoking was more prevalent among Turkish men than among those in other European countries and compared with male students in most other regions.55 In Asia and Africa the smoking rates of female students were lower than for males, as smoking is considered socially unacceptable for women.55 Smoking by women in Moslem societies is said to offend against social customs, and for women to smoke in public is considered shameful. This explains the low prevalence of smoking among women in Moslem countries such as Bahrain,22 Saudi Arabia,22 and Pakistan.36 With increasing education and urban residence, the frequency of smoking among women has risen but the smoking rate of men has not.55 ,78
Daily smoking among medical students
As medical students progress through their course their knowledge of smoking as a major cause of disease increases39 ,58 but, interestingly, superior knowledge did not lead to a lower rate of smoking, as students in the latter years generally smoked more than those in the earlier years. Table 1 shows that there is a disturbing worldwide trend for smoking rates to increase during time at medical school, particularly among male students. This is highlighted in the medical school in Bahrain in which there were no smokers in the first year, but prevalence rose to 45.5% by the final year.22 A comparison of rates across countries reveals that medical education fails to bring about a decrease in smoking rates. Students seem more likely to begin smoking in medical school than to give it up, and to increase their cigarette consumption rather than decrease it,58 supporting the suggestion that, in medical students, medical education and knowledge about the harmful effects of smoking have relatively little impact on smoking.22 Reviewing the students’ smoking rates in table 1, this comment appears to describe a worldwide phenomenon—that the effect of increased knowledge about smoking does not relate to students’ smoking behaviour.
While many medical schools teach about tobacco, providing the necessary information upon which to make an informed decision about continued tobacco use, for many students the timing of the information may be too late if given in the clinical years as initiation of smoking occurs earlier in the medical course, in the pre-clinical years,58 or even before medical school.74This evidence highlights the need for the topic of tobacco to be introduced early in the medical course and continued throughout the years of study.
Smoking rates of medical students compared with physicians and the general population
The smoking rates of medical students were lower than those of doctors in many countries.17 For example, a survey conducted in Czechoslovakia reported that 38% of male physicians, 25.6% of female physicians, and 49% of nurses were smokers, and these influential health professionals taught medical students, among whom 18% were smokers.41 Similar pictures emerge in other countries such as the Netherlands where 37% of male and 14% of female physicians smoked48 compared with 31% of male and 23% of female students; in Morocco where 44% of male physicians and 22% of female physicians smoked compared with 32% of male and no female medical students,18 and in Bahrain where 60.1% of male physicians smoked compared with 27.5% of male and 2.3% of female students.22
Between 45% and 69% of final year medical students in most world regions agreed that it was the doctor’s responsibility to set a good example by not smoking; however, only 16% of medical students thought this in Japan.17 In the UK 71% of students thought that it was entirely the doctor’s own business whether he or she smoked,63 and in a US study of 23 medical schools74 one third of students thought no action should be taken against physicians who smoke.
Leadership from the medical profession is essential if the world is to reduce preventable diseases caused by smoking. Teachers in medical schools should make every effort to present non-smoking role models17 and to encourage a sense of professional responsibility among students. The lower prevalence of smoking in students compared with physicians suggests that the next generation of physicians may be able to fulfil the exemplary role of non-smoking behaviour. The gradual disappearance of the smoking physician is mainly a generation effect which coincides with a dramatic change in social climate in relation to tobacco use.
Overall, the smoking rates of medical students were lower than the general population of their age and sex.17 For example, in a UK study of 13 medical schools 11% of medical students were smokers60 compared with 33% in the general population of the same age.79 In a US study of 23 medical schools senior medical students reported less use of tobacco compared with national age related groups.74 Compared with student data in table1, a similar pattern emerged in China where 61% of men and 7% of women in the general population smoked,28 ,80 Malaysia (men 41%, women 5%),34 Pakistan (men 66%, women very low),36 Thailand (men 67%, women 6%),37 ,81Denmark (40% of those aged 20–24 years),42 Australia (33.0% of men and 29.8% of women in the age group 18–39 years),39 ,82 and Bahrain (34.3% of men and 4.2% of women).22
Deficiencies in medical students’ knowledge of smoking related diseases
Although results from the studies conducted by the IUATLD are 5–9 years old, the findings revealed that medical students generally have poor knowledge of smoking as a major cause of diseases such as coronary artery disease, lung cancer, pulmonary emphysema and peripheral vascular disease, bladder cancer, and neonatal mortality.17 ,25 The deficiencies in knowledge among medical students shown in table 2 reflect a general failure of medical schools globally to teach about tobacco in the curriculum. These findings raise the issue that, if medical students are to become effective agents for reducing smoking when they graduate, then increased efforts need to be directed to increasing basic knowledge of tobacco related diseases in the medical curriculum.
Final year medical students’ knowledge of smoking as a major cause of diseases
Of course, it is expected that medical teachers will be aware of the important association between smoking and disease. In the Netherlands physicians and medical students knew of the relationship between smoking and development of lung cancer, coronary vascular disease, chronic bronchitis, peripheral vascular disease, emphysema, and carcinoma of the larynx.47 However, 12% of physicians were unaware of the association between smoking and leukoplakia, and only 43% of physicians knew of the association between cancer of the bladder and smoking.47
Medical students’ knowledge of smoking cessation techniques
Many final year students thought that they did not have adequate knowledge and skills to counsel patients about smoking.17 ,19 Most students claimed that they would advise a patient to quit only if the subject was raised by the smoker.17 ,55 More than half of Turkish students55 and around 45% of final year students in Africa16 ,18 and Tunisia19 thought that they had sufficient knowledge to counsel smokers, but students knew less about cessation techniques in Europe (27%),40 Asia (29%),25 and the former USSR (16%) (table3).33
Medical students who thought they had sufficient knowledge of smoking cessation techniques to counsel smokers
Extent of teaching about tobacco in medical schools
In a study to determine whether tobacco was taught in medical schools, the Tobacco Prevention Section, IUATLD collaborated with the WHO, Geneva. The aims were to determine the extent of teaching about tobacco, tobacco related diseases, and smoking cessation techniques to students in medical schools around the world, and to ascertain the problems of getting the topic of tobacco onto the medical curriculum.83 ,84
Using the WHO’s Directory of Medical Schools,85questionnaires were sent to 1353 medical schools in 159 countries. The questionnaires were translated into French, Russian, Japanese, and Mandarin. Table 4 shows that the most popular approach to teaching about tobacco was non-systematically as the topic arose, and only 11% of medical schools had a specific module on tobacco. There were 12% of schools who did not cover the topic of tobacco in the medical curriculum, and this was as high as one quarter in Africa and Asia. The content of the course commonly included knowledge about tobacco related diseases (98%), harmful components of tobacco (71%), effects of passive smoking (68%), and nicotine dependence (64%).83 ,84 Only one third taught about smoking cessation techniques. Whilst instilling the important role of the doctor as a non-smoking role model was important in North American medical schools, it was less important in the Middle East and Asia.83 More than a quarter of schools had experienced problems in introducing the topic of tobacco into the curriculum.
Teaching about tobacco issues by continent (n=485) (multiple responses)
There were many requests, especially from developing countries, for teaching resources and staff training in teaching programmes on tobacco and cessation techniques.83 One of the difficulties encountered by medical schools was in countering a lack of motivation among staff and students.
Another survey conducted by the Tobacco Prevention Section of the IUATLD jointly with the WHO involved circulating questionnaires to determine the extent of teaching about tobacco to deans of medical schools in European countries.86 The authors reported that only 8% had a specific module on tobacco, and in most medical schools tobacco was either systematically (35%) or unsystematically (55%) integrated with other teaching; 2% did not include tobacco issues. These findings generally concur with results from the survey distributed globally to medical schools.
A study conducted among 126 medical schools in the USA reported that only one third taught about smoking cessation methods and smoking prevention methods.87 Most students thought that smoking cessation was an important service for the physician to provide. However, they had low levels of confidence in the ability of physicians to provide smoking cessation advice or counselling because of the inadequacy of the present medical education for preparing physicians to provide such services.87-91 Students’ smoking assessment and cessation skills are underdeveloped and there is little opportunity to practise these skills in the inpatient setting.92 A US study found that only a quarter of physicians thought that their medical education had been effective in preparing them to assist smokers to stop smoking.93 This finding was confirmed in Turkey where less than half the doctors reported that they asked patients about smoking habits when they took a history, and only 40% believed that their level of education about smoking and health was adequate.57
Formats for teaching
Smoking related knowledge of medical students in Australia was found to increase significantly following training and was not dependent on mode of delivery, such as by traditional didactic lecture, use of role plays, audiotaped, peer, or video feedback.94A three hour seminar, including a lecture, video and small group discussion on tobacco, introduced to medical students in Hong Kong resulted in significant increases in knowledge.26 Training provided to US students resulted in increased confidence in their ability to provide effective assistance in smoking cessation.95 The lecture was the most common teaching method in the study of 126 US medical schools87 and the most common lecture topics were principles of cancer detection (73%) and cancer screening (72%), whereas the least likely lecture topics were related to prevention and cessation of smoking.87Formats such as role plays, computer-assisted instruction, group discussions,87 and simulated patients96 were found to be useful methods of teaching skills development and attitude change. The traditional didactic lecture mode was found to be an ineffective method in developing smoking cessation intervention skills.97
Teaching programmes on tobacco
The findings from the foregoing studies provide a major challenge to medical educators globally, and highlight the fact that medical schools should be encouraged to include teaching about tobacco issues in their curricula, and that teachers should present strong non-smoking models. Without adequate education in tobacco, doctors of the future will be unable to fulfil their important role in tobacco prevention and control. Yet medical practitioners are more likely to intervene and to achieve higher smoking cessation rates if they receive adequate training in intervention techniques and counselling.98-101
There are several programmes for teaching medical students about tobacco and smoking cessation intervention skills. The behavioural intervention developed by Ockene et al has been implemented in several US medical schools, and combines the use of guided questioning with the feedback of relevant information to assist the patient with smoking cessation.102
Another teaching programme is the Smokescreen Education Program which has been developed for medical students at the University of New South Wales (UNSW), Sydney and will be described here. The broad objectives are (1) to educate medical students in the health effects of tobacco use, (2) to raise awareness among students of the opportunities in medical practice to intervene with smoking patients, and (3) to educate students in the motivational aspects of assisting patients to stop smoking. There are two parts to the three hour teaching programme. Part I has nine sections from which the teacher can choose to develop a one hour lecture. Part I of the Smokescreen Education Program is based on Crofton’s Guidelines for teaching medical students about the health effects of tobacco: a checklist 103and Richmond’s Educating medical students about tobacco: teacher’s manual and students’ handouts.104 Part II deals with teaching medical students how to motivate patients to stop smoking and there are six components and is based on Richmond’s chapter.104 The education programme can be conducted in the lecture hall, in small groups in a tutorial room, and/or on the hospital ward. It can be extended if more time is available, which is the situation at UNSW. A handbook of parts I and II has been developed based on the chapters referred to above, and is provided to medical schools interested in implementing a teaching module on tobacco. The handbook includes copies of transparencies which can be used in the teaching of both parts.
In the one hour lecture there is a range of content areas from which the teacher can select including (1) smoking prevalence in their country and around the world, (2) harmful components of tobacco including nicotine, tar, and carbon monoxide, (3) health effects of tobacco use and benefits of quitting smoking, (4) health effects of passive smoking, (5) type of tobacco products, (6) nicotine dependence (characteristics, measurement of dependence, tolerance to nicotine, and withdrawal symptoms), (7) the role of the medical practitioner in tobacco control, including the effect of the doctor in advising patients to quit, (8) economic aspects of tobacco, and (9) the tobacco industry. When designing the one hour lecture some areas will be more relevant than others.
At the UNSW there are further opportunities to discuss tobacco issues in the medical curriculum. Correlation clinics are teaching opportunities in which several disciplines integrate teaching on various topics. During the correlation clinic on cardiovascular risk factors in year 4 several teachers present information on the major risk factors including smoking, and the cardiologist presents case studies for group discussions. Prior to this, during a lecture in community medicine, the students have completed a questionnaire on their lifestyle patterns. During the correlation clinic the results of the students’ cardiovascular risk factors are presented related to sex, age, and place of birth. The students are encouraged to find out if they are at risk of coronary heart disease during the two hour session on prevention which follows in a couple of days. At the prevention session many invited community groups set up display stands outside the lecture hall and the students are required to visit them and discuss the ways each community group is involved with prevention and promotion of health. At the same time students identify their cardiovascular risk factors by attending the stand where one community group measures students’ lung function using a spirometer, carbon monoxide using a carboximeter, cholesterol using a reflotron, and blood pressure, and presents them with a written record of their risk factors. Two community groups at the session are the National Heart Foundation and the Cancer Council who provide information on risk factors for heart disease and cancer.
Another opportunity to talk about smoking occurs during lectures on research designs in epidemiology in community medicine. Smoking studies over 30 years are used as examples of how knowledge is acquired in specific areas using various study designs.
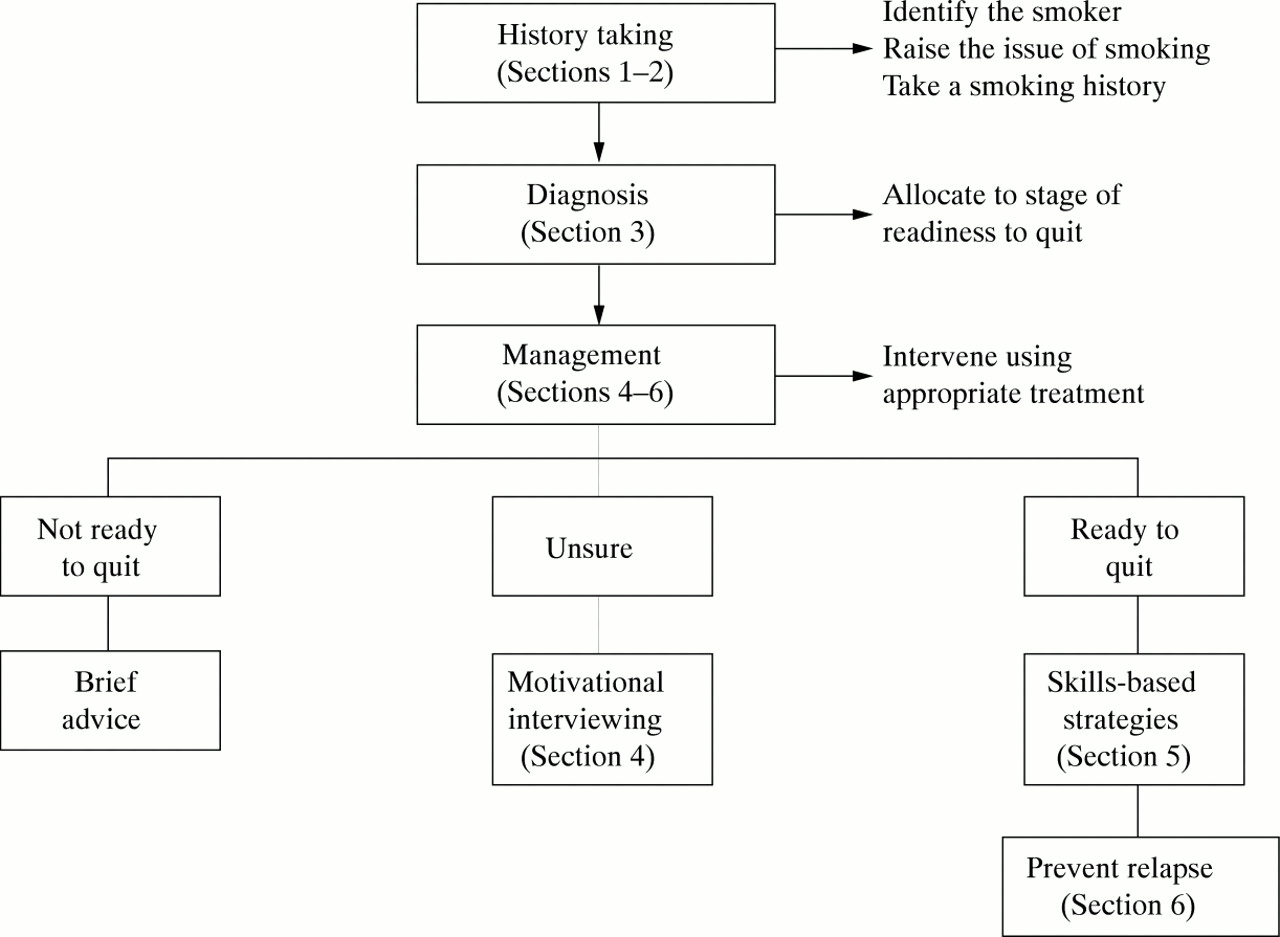
Part II of the Smokescreen Education Program focuses on increasing the student’s ability to intervene with people who are smokers.104 This programme takes two hours but can be extended. There are six sections: (1) identify the smoker; (2) take a smoking history; (3) allocate the smoker to the stage of readiness to change; (4) motivate smokers to change; (5) skills-based strategies; and (6) preventing relapse. For each of the sections there are notes for the teacher, handouts for students, and exercises. Figure 1 shows the six steps to motivate smokers to stop smoking.

Motivating patients to stop smoking. From Richmond.104
In section 1 the teacher discusses with students the difficulties doctors have in identifying smokers. At least half of smoking patients are not identified by the doctor. Identification is easier when the patient presents with a smoking related disease. There are two exercises that the teacher can use: identifying the organs affected by smoking, and problems in detecting use of tobacco based on case histories. In the hand out for students there are four case histories of smokers, and background notes on the health effects of smoking and passive smoking, harmful components of cigarette smoke, and nicotine dependence.
In section 2 students identify the elements of a smoking history and information is provided in the hand out given at the end of this exercise. An assessment of smoking history includes: number of cigarettes smoked on a work day and on a leisure day, duration of smoking, history of past health and risk factors for health problems, family history of tobacco use, pattern of use and triggers to smoke, level of dependence (using the Fagerstrom test for nicotine dependence105), and previous attempts at quitting. If the doctor’s time is limited, then only a few questions are asked to determine the smoking history.
A key element in smoking cessation is identifying the readiness of the smoker to stop smoking (section 3). A valuable model for assessing readiness to stop smoking is the “stages of change model” (the “transtheoretical model of change”) which was developed by Prochaska and DiClemente106 and Veliceret al.107 This model recognises that, at any one time, smokers are either not ready, unsure, or ready to stop smoking. Figure 2 presents the stages of readiness to change as a dynamic continuum in which smokers move from one stage of readiness to another as a result of various health, personal, work, and social circumstances. There are three exercises for this section: assessing stage of change; allocating to readiness to change groups; and a role play to practise allocating smokers to readiness to quit groups. Role plays give opportunities to rehearse newly acquired smoking cessation skills. Smokers in each stage of readiness to change have different needs and require different approaches by the doctor (fig 1).

{kind=link}
{kind=link}
Stages of readiness to change. From Richmond.104
About 40% of smokers at any one time are not ready to quit. This percentage may vary according to country. “Not ready” smokers are not thinking about quitting and may be resistant to any attempt to even discuss the subject. They generally see more positive aspects in smoking and do not like to acknowledge the disadvantages. The doctor’s approach with smokers who are not ready to change is to encourage them to think about the pros and cons of their smoking, and to return when ready to discuss smoking.
About 40% of smokers are uncertain or ambivalent about their smoking. They are thinking about the benefits of stopping smoking, but are also aware that there are disadvantages to quitting. The aim with unsure patients is to assist them to examine their habit, to help them weigh up the pros and cons of their smoking, and to decide whether to continue. A discussion of particular concerns about smoking and about quitting will often uncover a barrier such as worry about weight gain or concern about withdrawal symptoms, for which assistance such as nicotine replacement therapy may be offered. Smokers who are unsure about stopping smoking require motivational interviewing in which they decide which of the conflicting courses of action should be followed. An unsure smoker may require some time before he/she has weighed up the pros of quitting in favour of the cons.
Only 20% of smokers at any one time are actually ready to stop smoking. They have made a commitment seriously to attempt to stop smoking. For them the disadvantages of smoking outweigh the benefits. Ready patients need specific brief advice to help them overcome withdrawal symptoms, triggers for smoking and support. The ready smoker may require several attempts at quitting before stopping successfully. There are three exercises provided in the programme from which the teacher can choose.
There are many benefits to categorising smokers according to their readiness to change. It maximises the use of the doctor’s resources, little time is wasted on smokers who are not yet ready to change their smoking habit, and more time can be spent with those most likely to benefit.
The purpose of section 4 is to make students aware that there are two sides to making most decisions, and that reaching a decision involves a process of weighing up the pros and cons. Motivational interviewing is a style of counselling for patients who are ambivalent or unsure about stopping smoking, and it assists smokers to explore their habit and concerns.108 A key principle in the four brief steps of motivational interviewing is that it is a patient-centred approach in which the smoker takes responsibility for the behaviour change.104 There are three exercises provided from which the teacher can select.
When the smoker has decided to stop smoking (20% of smokers) there are a range of skills and strategies that should form the plan of action (section 5). The exercise consists of identifying the components of the plan of action to stop smoking based on a case history. Table 5presents components of the plan which can be used as a basis for an examination question.
Components of a plan of action to stop smoking
Section 6 deals with preventing relapse, a common result among those who attempt to stop smoking. Recognition of situations that are high risk for relapse and the strategies that enable craving to be resisted are important elements of the learning process that will enable a plan to cope with future lapses to be developed. There are two exercises in which students identify high risk smoking situations and develop a relapse prevention plan based on a case history.
Implementing the teaching programme in other countries
The Smokescreen Education Program has been introduced to respiratory physicians in a three hour workshop at the 27th Global Conference on Lung Health in Mainz, Germany in 1994, over two days in a meeting of doctors from different parts of China in Beijing in 1995, implemented among teachers in most of the 37 medical schools in Turkey in 1996, presented during a workshop at the 10th World Conference on Tobacco or Health in Beijing in 1997, and in a one day workshop to be conducted at the IUATLD conference in Thailand in 1998.
CHINA
The study of smoking rates among Chinese medical students in Shanghai Medical University revealed high levels of smoking among male students and rates increased as the students progressed through the course (see table 1).28 There were widespread deficiencies in knowledge of smoking as an important causal factor in many diseases. The researchers concluded that the results from their study indicated that the current system of medical education in China has little effect on the attitudes and behaviours of medical students regarding smoking. The IUATLD survey84 found that, among the 39 who responded, three Chinese medical schools included a specific module in their curricula, 27 integrated tobacco teaching with other subjects, and 10 did not teach about tobacco.
The Smokescreen Education Program has been translated into Mandarin. Two series of workshops have been conducted in China in which teachers in medical schools have been trained in the program. In December 1997, with a WHO (Manila) consultancy, two two-day workshops were conducted in Shanghai and in Beijing. Four months later more than half of the medical universities had implemented the teaching programme in their curriculum. In July 1998 two further workshops were conducted in the north of China in Chang Chun and in southern China in Wuhan with the support from the Community Health and Anti-Tuberculosis Association (CHATA), Sydney. At one Chinese medical university, students have to sign a pledge on entry to medicine that they will not smoke during their time at university. If found smoking they are given one warning, then expelled. If staff are found smoking they are fined one quarter of their monthly wage.
ITALY
A study conducted in Italy found that 35% of the Italian population aged over 14 years of age are smokers, and that 43% of doctors smoke.109 When Italian medical schools were surveyed with regard to their teaching about tobacco it was found that no medical school in Italy had a syllabus which specifically taught about tobacco related issues.109 Where teaching about tobacco did exist it consisted of tobacco as a risk factor for respiratory and cardiovascular diseases and was conducted in a didactic mode on the hospital wards during teaching of respiratory physiopathology and bronchology. The researchers found little evidence of teaching about smoking cessation.109 The Smokescreen Education Program has been translated into Italian and is ready for implementation into Italian medical schools. An official statement about the poor situation in Italian medical schools with respect to the lack of teaching about tobacco will be published by a professor from an Italian medical school, and he will make recommendations about implementing the Smokescreen program in the medical curricula.
The Smokescreen Education Program is currently being translated into French and Japanese for implementation in medical schools in countries with these languages.
Conclusions
It is important in public health terms that future doctors are educated adequately in medical school so that they become knowledgable in tobacco control and prevention measures and develop skills in smoking cessation. However, the literature reveals serious deficiencies in knowledge and counselling skills among medical students, and large gaps in the medical curriculum with respect to tobacco issues. Students generally have a poor knowledge of smoking as a major cause of diseases such as coronary artery disease, lung cancer, pulmonary emphysema, peripheral vascular diseases, bladder cancer, and neonatal mortality. This is not surprising as few medical schools have a tobacco module in the curriculum. Although students accept that not smoking is part of the doctor’s exemplar role, the modelling of non-smoking has not been presented consistently to them as some members of the teaching staff were smokers and may have justified their habit to students.58 The ambivalent picture presented by staff to students may encourage continued smoking among students. A more determined and concerted effort is required in which quit programmes are offered to students, and teaching staff present as non-smoking models. The disincentives to smoke in a Chinese medical school are further innovative ways to curb smoking in medical school. What emerges from the many studies conducted in medical schools worldwide is the great deal of work that is required to rectify the situation, particularly in developing countries where the full impact of the smoking epidemic has yet to be experienced.110 If future medical practitioners are to engage actively in advising smokers to quit, it is vital that they acquire the skills and knowledge base which will allow them to accomplish this task. Medical students should receive sufficient knowledge of the determinants of smoking and specific training on how to help patients to stop smoking, and a tobacco module should be included in the curriculum of every medical school. Medical schools in developed countries should be prepared to offer assistance and work jointly with medical schools in developing countries. The information and resources that we have produced in developed countries must become available to physicians and teachers in medical schools around the world so that medical students can be adequately prepared to fulfil their future medical function by assisting patients to stop smoking.