Article Text

Statistics from Altmetric.com
We read with interest the paper by Kemp and colleagues1 which utilises cumulative sum (CUSUM) to analyse the learning curves associated with endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA). The retrospective study from five centres demonstrated that variable learning periods are required to attain proficiency in the procedure, and a pooled sensitivity of 67.4% was observed.
The authors are to be commended on using CUSUM to calculate the learning curves for EBUS-TBNA; however, several points deserve comment. First the study only includes patients undergoing EBUS-TBNA for the diagnosis or staging of lung cancer. In clinical practice, the procedure is also commonly employed for the diagnosis of isolated mediastinal lymphadenopathy, and these procedures should be incorporated in the learning process. Secondly, the authors included non-malignant nodes in the CUSUM analysis. Therefore, it may be possible to inadequately sample a benign node and for the result to be assigned as a true negative. This highlights the importance of reporting the disease prevalence for each cohort. Thirdly, utilising the criteria employed in this paper, there is potential to miss a diagnosis of sarcoidosis or tuberculosis and for the procedure to still be classified as a true negative. Fourthly, it should be emphasised that CUSUM analysis is suited to ongoing audit of the EBUS service beyond the learning curve and that issues with training and competence may be identified before 100 cases are reached. A final point is an inaccuracy in the definition of Q in the description of the CUSUM methodology. The paper states Q=ln((1–p1)/(1–p0)), where it should be Q=ln((1–p0)/(1–p1)). The value of s obtained is however correct, so does not represent an error in calculation by the authors.
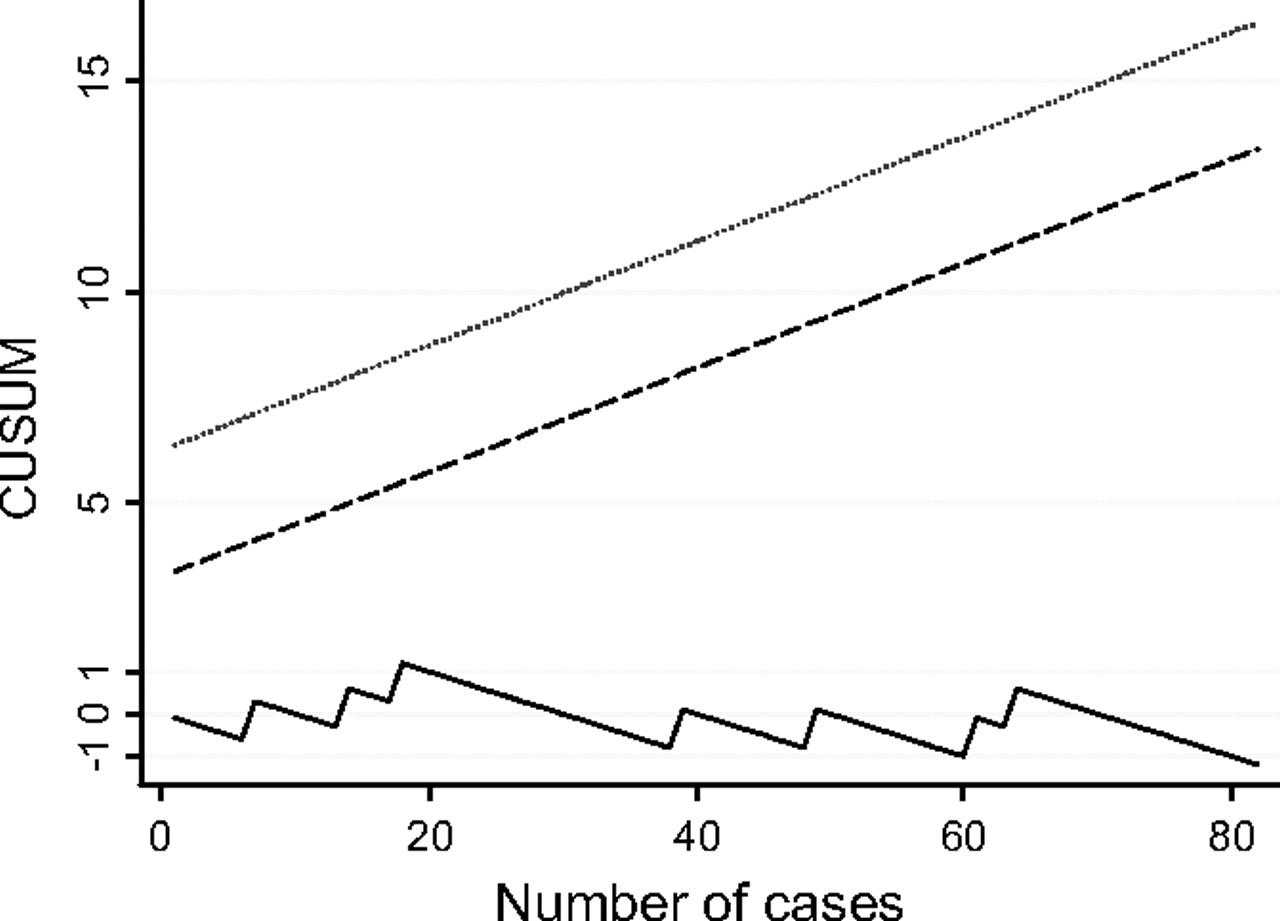
In our institution, a tertiary teaching centre, EBUS-TBNA has been performed by two physicians (NN and SJ) since February 2008. In order to maximise our learning process, a gastroenterologist (SP) with expertise in endoscopic ultrasound (EUS) attended the first 25 of our procedures. The CUSUM chart for our initial 120 cases (reached in November 2008) is shown in figure 1. Only patients with abnormal nodes were included in the analysis and nodes <1 cm in the short axis were excluded. Real-time evaluation of aspirates was available by an on-site cytologist in 23 (19%) cases. The chart demonstrates a short learning curve with a rise in the curve and a learning period over the first 20 patients. After this, the curve reaches a steady state below the alert line, indicating that the target sensitivity was being met and performance remained acceptable for the duration of the series. In contrast to the data from Kemp et al, isolated mediastinal lymphadenopathy was the indication for EBUS-TBNA in 53 (44%) of the patients in our initial cohort. The sensitivity of EBUS-TBNA for our first 120 patients undergoing EBUS-TBNA was 90% with a diagnostic accuracy of 93% and negative predictive value of 83% when the disease prevalence was 68%. No false positives were observed and therefore the specificity and positive predictive values were 100%.

{kind=link}
CUSUM chart of the learning curve of endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) at our centre using an acceptable false-negative rate of 10% and an unacceptable rate of 15%.
EBUS-TBNA is an important procedure for the diagnosis of mediastinal lymphadenopathy and its use will continue to spread. Where available, inviting gastroenterologists and pathologists into the bronchoscopy suite may help to shorten the learning curve.
Reference
Footnotes
Funding NN is Medical Research Council Research Training Fellow; PN is funded by a ERS Long Term Research Fellowship; SMJ is Welcome Trust Senior Research Fellow.
Competing interests None.
Provenance and peer review Not commissioned; not externally peer reviewed.