Article Text

Statistics from Altmetric.com
Pulmonary thromboendarterectomy (PTE) can provide a surgical cure for the pulmonary hypertension of chronic pulmonary embolism. This form of pulmonary hypertension often goes unrecognised, yet it is progressive and carries a high mortality. Many physicians are unaware that a corrective operation exists, and rely instead on referral for transplantation or merely palliative medical treatment. PTE is technically demanding for the surgeon, and requires careful dissection of the pulmonary artery planes and the use of circulatory arrest. Excellent short and long term results can be achieved, however, and increased awareness of both the prevalence of this condition and the possibility of a surgical cure should avail more patients of the opportunity for relief from this debilitating and often fatal disease.
Acute pulmonary embolism has been said to result in more than 600 000 symptomatic episodes in the United States each year, and to be the principal cause of death in 200 000 patients.1 However, this may be an underestimation as necropsy studies have shown that the diagnosis of acute pulmonary embolism was unsuspected in 70–80% of patients in whom it was the principal cause of death.2 ,3The majority of surviving patients appear gradually to resolve their pulmonary emboli over time. However, complete resolution of embolic material does not always occur; the pulmonary clots then organise, and narrow or occlude the pulmonary arterial branches—pulmonary hypertension results.
How many patients affected by acute pulmonary embolism develop chronic sequelae? The natural history of acute pulmonary embolism is not entirely clear as most patients are not followed serially with lung scans or echocardiography, and acute pulmonary embolism is an underdiagnosed condition. However, significant pulmonary hypertension due to chronic pulmonary embolism is not a rare disease. Presti4 found chronic massive thrombosis of major pulmonary arteries in nearly 1% of 7753 necropsies. Many patients who have had relief of their pulmonary hypertension following PTE have had disease confined to their minor pulmonary arteries, and chronic thrombus in these smaller pulmonary vessels is probably often overlooked in necropsy series. In addition, it is well known that pulmonary hypertension persists and may indeed be progressive long after evidence of the original thrombus has disappeared. For these reasons, the actual prevalence of the chronic form of this disease is almost certainly underestimated.
Although the surgical operation for acute pulmonary embolism remains controversial, operation for chronic pulmonary embolism is now well established. As Trendelenburg first described in 1908,5the bronchial circulation protects the lung parenchyma from ischaemia when a thrombus occludes a pulmonary vessel. The lungs can thus sustain an embolic event without parenchymal necrosis, in contrast to the heart or brain that lack this supplemental blood supply. Resolution or removal of embolic occlusion even years afterwards will therefore result in resumption of functional oxygenation in the affected portion of the lung.
The prognosis for patients with untreated pulmonary hypertension is poor. There is a 30% five year survival rate for patients with mean pulmonary artery pressures > 30 mm Hg, and only 10% of those with pressures > 50 mm Hg are still alive after five years.6 Medical treatment for embolic pulmonary hypertension (anticoagulants, vasodilators, or thrombolytic agents) is seldom even transiently effective.7 ,8
Preoperative assessment
Patients with chronic pulmonary thromboembolic disease typically present with progressive dyspnoea on exertion, followed by signs of worsening right heart failure. Some may show evidence of severe cor pulmonale but many describe only vague symptoms, easily attributable to other causes. Fewer than half can describe either a past deep venous thrombosis or episode of pulmonary embolus. Many cases therefore remain undiagnosed, especially when the pulmonary artery pressures are normal at rest.
Once pulmonary hypertension is suspected, a lung scan will determine whether major perfusion defects are present. The major differential diagnosis is primary pulmonary hypertension. This is an important distinction as performing PTE on a patient with primary pulmonary hypertension is not only ineffective but carries a high mortality. Significant pulmonary hypertension due to emboli is unlikely if the perfusion scan is completely normal, but unfortunately perfusion scans tend to underestimate thrombotic occlusion. Complete evaluation must include right heart catheterisation to measure the right heart pressures and pulmonary angiography to identify the pulmonary artery anatomy. Reservations are often expressed regarding the performance of pulmonary arteriograms in pulmonary hypertensive patients, but in our experience of more than 1000 such procedures, high quality pulmonary angiography can be performed safely.9 Selective power injections of the right and left pulmonary trunks using non-ionic contrast agents to prevent the cough response are well tolerated, and there has been no mortality or morbidity. When the cause of the pulmonary hypertension remains unclear, even after angiography, pulmonary angioscopy may be performed.10 The pulmonary angioscope is placed into the pulmonary artery through central venous access, and a balloon at its tip inflated. This produces a bloodless field for inspecting the pulmonary vasculature. Clot, or fibrous webs and bands involving the vessels are diagnostic of thrombotic sequelae. Lung biopsy has not proved helpful in the differential diagnosis.
Most patients referred for PTE have a pulmonary vascular resistance > 1000 dynes/s/cm−5, and many have suprasystemic pulmonary artery pressures. The patients operated on for this condition have ranged in age from 14 to 83 years. The documented history of pulmonary vascular occlusion has been as brief as a few months to as long as 24 years. Before PTE, an inferior vena cava filter is always placed. Patients are thereafter treated with anticoagulants indefinitely.
The operation
The PTE operation as performed at our centre, the University of California San Diego, has been described in detail elsewhere.11 In our experience of 700 cases completed since 1990, three guiding principles have determined success. First, the operation must be performed on both lungs as patients with significant chronic embolic pulmonary hypertension invariably have bilateral disease. Second, cardiopulmonary bypass with periods of circulatory arrest is essential to achieve adequate exposure in the face of the copious bronchial blood flow. Third, a true endarterectomy in the plane of the media must be accomplished.
Under general anaesthesia and on cardiopulmonary bypass, the patient is cooled to 20°C. Circulatory arrest is initiated. The operation begins on the right pulmonary artery, which has been fully exposed by dissection out to the hilum. Any loose thrombus is removed. It is essential to appreciate that the removal of visible thrombus is largely incidental to this operation. Indeed, in the majority of patients, no free thrombus is present, and initial direct examination of the pulmonary vascular bed may appear normal. It cannot be overemphasised that the key to the success of the operation is complete endarterectomy of the entire pulmonary arterial tree.
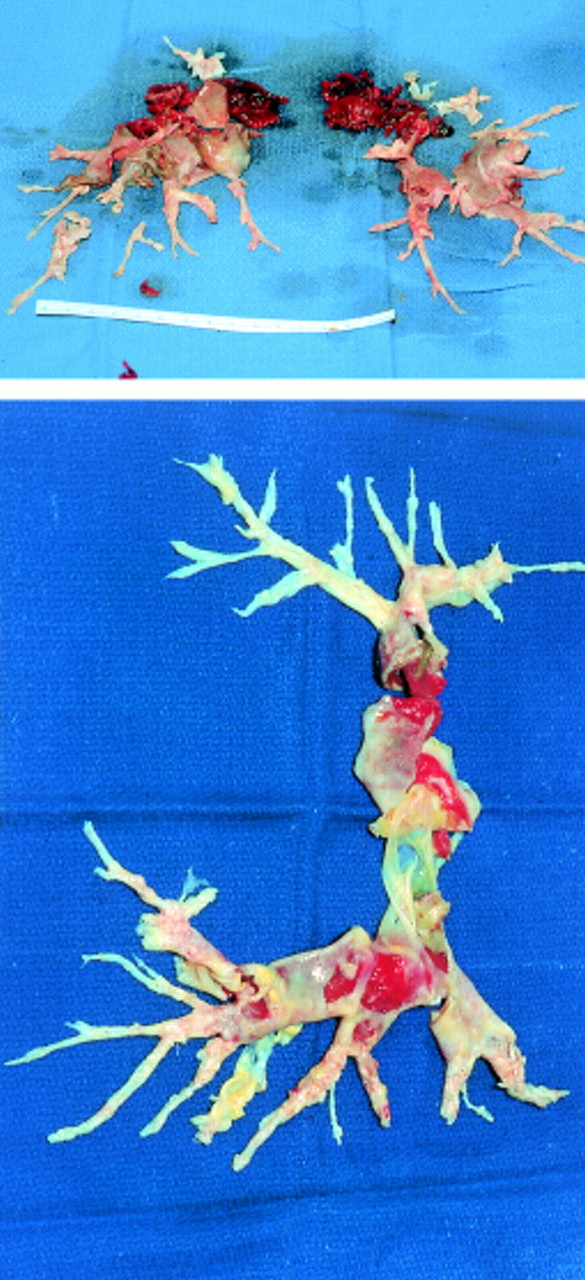
The endarterectomy plane is developed. Each lobe is endarterectomised, and then each segmental and subsegmental artery pursued distally. Although many of these vessels cannot be visualised initially, progressive dissection and traction allow a complete endarterectomy of the entire pulmonary vascular bed (fig 1). This is a painstaking and technically demanding process, and periods of reperfusion with resumption of cardiopulmonary bypass may be necessary to avoid prolonged circulatory arrest. When the endarterectomy on the right side has been completed, the procedure is repeated on the left. Bypass is then reinstituted and the patient rewarmed. Intraoperative transoesophageal echocardiography invariably demonstrates some degree of tricuspid valve regurgitation, but tricuspid valve repair is not performed. Right ventricular remodelling occurs within a few days, with return of tricuspid competence.

{kind=link}
Endarterectomy of the entire pulmonary vascular bed.
Postoperative management
Meticulous postoperative management is essential to the success of this operation. All patients are mechanically ventilated for at least 24 hours, and all are subjected to vigorous diuresis. Most patients can be extubated on the first postoperative day, and leave the hospital after 7–10 days.
Reperfusion pulmonary oedema (the so called reperfusion response) is a rare complication, which occurs within the first 72 hours following PTE.10 Blood overperfuses the endarterectomised areas of the lung, causing a pulmonary capillary leak. Diversion of blood away from the normal areas of the lung results in severe hypoxia, and this is compounded by hypoxic pulmonary vasoconstriction of the normal vessels. Careful management of ventilation and fluid balance will minimise the alveolar capillary leak. Treatment is supportive, as reperfusion pulmonary oedema will eventually resolve if oxygenation can be maintained. Cerebral complications from circulatory arrest are no longer encountered, with the shorter circulatory arrest periods that have come with significant experience with this technique.
Results following PTE
Of the 850 PTE operations performed at our centre over the past 25 years, 700 have been completed since 1990, when the surgical procedure was modified.11 The mortality rate is 6.4% in the most recent 500 patients.12 The haemodynamic and functional improvement achieved in survivors has been excellent. Right heart catheterisation routinely shows a marked and sustained reduction in pulmonary artery pressure and pulmonary vascular resistance as well as a substantial improvement in cardiac output. Significant recovery of right ventricular function and resolution of tricuspid regurgitation is apparent by cardiac echocardiography. Long term results document haemodynamic and respiratory improvement, which appears to persist indefinitely, with New York Heart Association functional classification generally improving from class III or IV to class I.13
Summary
Although PTE is potentially curative for thromboembolic pulmonary hypertension, probably fewer than 1500 of these operations have been performed worldwide. Unquestionably, the disease is under-recognised, and even among cardiac surgeons PTE is considered very hazardous and perhaps of questionable long term benefit. Our experience does not support this view. There is neither disagreement regarding the poor prognosis of patients with pulmonary hypertension nor the unsatisfactory results of medical treatment for this disease. The only surgical alternative to PTE is lung transplantation. Compared to lung transplantation, PTE offers a lower surgical mortality rate, better long term survival, and fewer chronic complications. The mortality rate for PTE at our centre is now in the range of 5–7%, with documented sustained functional improvement in survivors. These results clearly favour PTE as the primary treatment for thromboembolic pulmonary hypertension, and physicians should be encouraged to identify patients with this now curable disease.