Article Text

Abstract
Background: Leukotriene (LT) B4 concentrations are increased and prostaglandin (PG) E2 concentrations are decreased in exhaled breath condensate (EBC) in patients with chronic obstructive pulmonary disease (COPD). A study was undertaken to investigate the short term effects of cyclo-oxygenase (COX) inhibition on exhaled LTB4 and PGE2 concentrations in patients with COPD and to identify the COX isoform responsible for exhaled PGE2 production.
Methods: Two studies were performed. A double blind, crossover, randomised, placebo controlled study with ibuprofen (400 mg qid for 2 days), a non-selective COX inhibitor, was undertaken in 14 patients with stable COPD, and an open label study with oral rofecoxib (25 mg once a day for 5 days), a selective COX-2 inhibitor, was undertaken in a different group of 16 COPD patients. EBC was collected before and after drug treatment. Exhaled LTB4 and PGE2 concentrations were measured with specific immunoassays.
Results: All patients complied with treatment as indicated by a reduction in ex vivo serum thromboxane B2 concentrations (ibuprofen) and a reduction in lipopolysaccharide induced increase in ex vivo plasma PGE2 values (rofecoxib) of more than 80%. Exhaled LTB4 was increased after ibuprofen (median 175.5 (interquartile range 128.8–231.5) pg/ml v 84.0 (70.0–98.5) pg/ml, p<0.001) and exhaled PGE2 was reduced (93.5 (84.0–105–5) pg/ml v 22.0 (15.0–25.5) pg/ml, p<0.0001). Rofecoxib had no effect on exhaled LTB4 (p = 0.53) or PGE2 (p = 0.23).
Conclusions: Non-selective COX inhibition decreases PGE2 and increases LTB4 in EBC, whereas selective COX-2 inhibition has no effect on these eicosanoids. PGE2 in EBC is primarily derived from COX-1 activity, and COX inhibition may redirect arachidonic acid metabolism towards the 5-lipoxygenase pathway.
- COPD, chronic obstructive pulmonary disease
- COX, cyclo-oxygenase
- EBC, exhaled breath condensate
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- LTB4, leukotriene B4
- NSAID, non-steroidal anti-inflammatory drug
- PGE2, prostaglandin E2
- TxB2, thromboxane B2
- cyclo-oxygenase
- exhaled breath condensate
- chronic obstructive pulmonary disease
- leukotriene B4
- prostaglandin E2
Statistics from Altmetric.com
- COPD, chronic obstructive pulmonary disease
- COX, cyclo-oxygenase
- EBC, exhaled breath condensate
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- LTB4, leukotriene B4
- NSAID, non-steroidal anti-inflammatory drug
- PGE2, prostaglandin E2
- TxB2, thromboxane B2
- cyclo-oxygenase
- exhaled breath condensate
- chronic obstructive pulmonary disease
- leukotriene B4
- prostaglandin E2
Concentrations of leukotriene (LT) B4, a potent neutrophil chemoattractant, are detectable in sputum in patients with stable chronic bronchitis1 and are raised in patients with chronic obstructive pulmonary disease (COPD) during acute exacerbations.2 Prostaglandin (PG) E2, an endogenous bronchodilating compound, may have anti-inflammatory effects in the airways.3–5 The isoprostanes are prostaglandin-like compounds which are formed by the free radical catalysed peroxidation of arachidonic acid in the plasma membrane phospholipids.6,7
LTB4, PGE2, and 8-isoprostane (15-F2t-isoprostane or 8-iso-PGF2α) concentrations are increased in exhaled breath condensate (EBC) in patients with COPD.8,9 EBC is a completely non-invasive method of sampling secretions from the airways.10–12 Preliminary data show that ibuprofen, a non-selective cyclo-oxygenase (COX) inhibitor, decreases exhaled PGE2 concentrations in patients with stable COPD.13 As PGE2 may have anti-inflammatory effects in the airways, raised PGE2 levels in COPD might represent a mechanism for counteracting lung inflammation in this disease.8 This is further supported by the selective increase in exhaled PGE2 in patients with COPD but not in asthmatics,14 and the correlation between exhaled LTB4 and PGE2 concentrations in patients with COPD.8 Taken together, these data indicate that non-selective COX inhibition might have important implications for lung inflammation in COPD patients.
A study was undertaken to investigate the short term effect of non-selective and selective COX-2 inhibition on exhaled LTB4, PGE2, and 8-isoprostane concentrations in patients with stable COPD and to identify the COX isoform responsible for exhaled PGE2 production.
METHODS
Study design
Two studies were performed. The first study was a double blind, crossover, randomised, placebo controlled study with ibuprofen. The study duration was 11 days. Patients attended the outpatient clinic at the Royal Brompton Hospital, London on days 1, 3, 9, and 11. Visit 1 was a screening visit for clinical examination, spirometric tests, skin prick testing, EBC collection, and venous blood sampling. On the same day they were randomised to receive either oral ibuprofen (400 mg every 6 hours) or matched placebo for 2 days. After 2 days of treatment and a morning dose of 400 mg of either ibuprofen or placebo, all the above tests except skin prick tests were repeated (visit 2). After a 5 day washout the patients underwent the other arm of the study.
The second study was an open labelled, uncontrolled study of rofecoxib, a selective COX-2 inhibitor. Patients attended the COPD outpatient clinic of the Department of Internal Medicine, Catholic University of the Sacred Heart, Rome, Italy on three occasions for clinical examination, EBC collection, spirometric tests, sputum induction, measurement of arterial blood gas tensions, and venous blood sampling. After a screening visit (visit 1) and a 2 week run-in period (visit 2), patients were given oral rofecoxib (25 mg once daily for 5 days). After treatment all the above tests were repeated (visit 3). Skin prick testing was performed at visit 1.
Day to day repeatability of eicosanoid measurements in both the ibuprofen and rofecoxib study group patients was assessed in a randomised design before patients entered the study by collecting three EBC samples within 7 days of the first.
The ibuprofen study was approved by the ethics committee of the Royal Brompton Hospital and Harefield Trust, London, and the rofecoxib study was approved by the ethics committee of the University Hospital “A Gemelli”, Catholic University of the Sacred Heart, Rome. Informed consent was obtained from each patient.
Subjects
In the ibuprofen study 15 patients with stable severe COPD were studied (table 1), of whom 14 completed the study. One patient was excluded because of lack of compliance.
Characteristics of ibuprofen study subjects (n = 14)*
In the rofecoxib study 17 patients with stable moderate COPD were enrolled (table 2), 16 of whom completed the study. One patient was excluded because of COPD exacerbation and recent smoking exposure.
Characteristics of rofecoxib study subjects (n = 16)*
In both studies the diagnosis and classification of COPD severity were based on the Global Initiative for Obstructive Lung Disease (GOLD) guidelines.15 All patients who completed the studies were clinically stable with baseline post-bronchodilator forced expiratory volume in 1 second (FEV1) <80% predicted and FEV1/forced vital capacity (FEV1/FVC) ratio <70% which did not change markedly over 8 weeks. Patients with other respiratory or systemic diseases were excluded from the studies. All patients had negative bronchodilator reversibility testing defined as an increase in FEV1 that was both lower than 200 ml and 12% above the pre-bronchodilator FEV1 after inhalation of 400 μg salbutamol. All study subjects were ex-smokers and had stopped smoking for at least 6 months. They all had a negative history for atopic disease and negative skin prick testing. In the ibuprofen study, smoking status was checked by measuring urinary cotinine levels which were <10 ng/ml in all study subjects (data not shown). Six of the 14 patients were treated with inhaled corticosteroids (table 1). Patients had never received LT receptor antagonists or 5-lipoxygenase inhibitors. None of the patients had received non-selective non-steroidal anti-inflammatory drugs (NSAIDs) in the previous 10 days and none had ever received COX-2 inhibitors.
In the rofecoxib study, smoking status was checked by measuring arterial carbomonoxyhaemoglobin (HbCO, table 2). None of the patients had received corticosteroids in the previous 4 weeks. Patients had never received LT receptor antagonists, 5-lipoxygenase inhibitors, or COX-2 inhibitors. As two patients were on treatment with NSAIDs at baseline (visit 1), a 10 day washout period preceded the run-in. Inhaled β2 adrenergic agonists and anticholinergic drugs were used in some patients in both groups (tables 1 and 2).
Pulmonary function
Spirometric parameters were measured using a dry spirometer (Vitalograph Ltd, Buckingham, UK) in the ibuprofen study and a 10 l bell spirometer (Biomedin, Padova, Italy) in the rofecoxib study. Three to a maximum of six acceptable manoeuvres were performed until the two largest FEV1 and FVC values were within 0.2 l of each other. The best value was chosen.
Exhaled breath condensate collection and measurement of exhaled eicosanoids
In both studies EBC was collected using a condensing chamber (Ecoscreen, Jaeger, Hoechberg, Germany) as described previously.9 Subjects were instructed to breath tidally through a mouthpiece connected to the condenser for 15 minutes while wearing a noseclip. An average of 1.0 ml EBC per patient was collected in the ibuprofen study and 1.1 ml EBC in the rofecoxib study. Samples were stored at −80°C before eicosanoid measurements. α-Amylase concentrations in all EBC samples were measured by an in vitro colorimetric method (detection limit 22 U/ml) to check for possible salivary contamination (Roche Diagnostics, Basel, Switzerland).
LTB4 was measured by a commercially available enzyme immunoassay (Cayman Chemical, Ann Arbor, Michigan, USA);8,16 PGE2 and 8-isoprostane were measured by radioimmunoassays using specific antisera.17 Specificity for LTB4, 8-isoprostane, and PGE2 was previously confirmed by reverse phase-high performance liquid chromatography (RP-HPLC).16,17 The immunoassay detection limit was 4 pg/ml for LTB4 and 10 pg/ml for 8-isoprostane and PGE2. The intra-assay and interassay coefficients of variation for eicosanoid were as follows: LTB4, <10% and <15%, respectively; 8-isoprostane, <4% and <11%, respectively; PGE2, <4% and <5%, respectively.
Sputum induction
Sputum induction was performed as previously described.18 Subjects inhaled 3.5% saline for 15 minutes via an ultrasonic nebuliser (DeVilbiss 2000, DeVilbiss Co, Heston, Middlesex, UK) with a calibrated mass median aerodynamic diameter of 4.5 μm and output of 4.5 ml/min. Secretions collected during the first 5 minutes were discarded to minimise squamous epithelial cell contamination. Samples were considered adequate for analysis if there was <50% squamous cell contamination. Sputum samples were processed immediately. Dithiothreitol solution (0.1%) (Sigma-Aldrich Co, St Louis, MO, USA) was added to the sputum and the mixture was allowed to stand for 30 minutes. Cell viability was determined by exclusion of Trypan Blue. After centrifugation at 1500g for 8 minutes, the cell pellet was resuspended in 10 ml Presercyt solution and fixed overnight. Thin layer slides were prepared using the Thin Prep 2000 automated slide processor (Cytyc Co, Boxborough, MA, USA).19 100 μl of suspension were added to 50 ml of Preservcyt solution and placed in the automated slide processor. After dispersion, cells were automatically collected on a polycarbonate filter membrane. The thin, evenly dispersed monolayer of cells was then deposited onto the slide in a 20 mm circle. Residual mucus and erythrocytes were removed in the process. For each determination two slides were prepared and stained with either the Papanicolaou or May-Grünwald-Giemsa method. Differential cell counts were expressed as a percentage of lower airway cells (that is, excluding squamous epithelial cells). Differential cell counts for epithelial cells, macrophages, lymphocytes, and neutrophils were performed using Papanicolaou stained slides; differential cell counts for eosinophils were performed using May-Grünwald-Giemsa stained slides.
Serum thromboxane B2 (TxB2) measurement
Compliance with ibuprofen treatment was assessed by measuring ex vivo serum TxB2 concentrations at each visit as treatment with ibuprofen suppresses production of serum TxB2 in response to endogenously formed thrombin.20 Blood drawn by a plastic syringe was immediately transferred into glass tubes and allowed to clot at 37°C for 30 minutes. Serum was separated by centrifugation and stored at −20°C until assayed. Serum TxB2 concentrations were measured by a radioimmunoassay as described previously.20
Plasma PGE2 measurement
Compliance with rofecoxib treatment was assessed by measuring plasma PGE2 concentrations after ex vivo platelet COX-2 activation with lipopolysaccharide (LPS) and COX-1 inhibition with aspirin.21 A venous blood sample (5 ml) was drawn and collected in a heparinised tube before (visit 2) and after treatment with rofecoxib (visit 3). One ml aliquots of whole blood samples were incubated at 37°C for 24 hours in tubes containing LPS (10 μg/ml) to activate COX-2 and a low dose of aspirin (10 μg/ml) to selectively suppress platelet COX-1 or tubes containing no LPS to assess basal PGE2 production derived from COX-2 (control samples). Plasma was separated by centrifugation and kept at −30°C until assayed for PGE2 as described previously.21 COX-2 inhibition after rofecoxib was expressed as percentage of decrease in plasma PGE2 concentrations compared with pretreatment values in LPS containing samples after subtracting basal plasma PGE2 concentrations (control samples).
Arterial blood gas tensions
Arterial oxygen and carbon dioxide tensions (Pao2, Paco2) and pH were measured using an ABL 510 blood/gas analyser (Radiometer, Copenhagen, Denmark).
Sample size
The sample size for both studies was calculated22 considering LTB4 concentrations in EBC as the primary outcome. Sample size was estimated to be 15 subjects based on exhaled LTB4 concentrations, after having considered a standard deviation of 20 pg/ml, a drop out rate of 20%, and identified the minimal difference of biological significance (33.8 pg/ml) with a power of 90% (α value of 5% and β value of 10%). Size effect corresponds to a 33% increase in LTB4 concentrations after drug treatment.
Statistical analysis
LTB4, PGE2, and 8-isoprostane concentrations in EBC and cell counts in sputum were expressed as medians with interquartile range (IQR) in parentheses. Exhaled LTB4, PGE2 and 8-isoprostane concentrations, cell counts in sputum within the treatment group, and comparisons before and after treatment were analysed using Friedman’s repeated measures of analysis of variance. Spirometry, arterial blood gases, serum TxB2, and plasma PGE2 values followed a normal distribution and were expressed as mean (SE). Spirometric values and arterial blood gases within the treatment group and comparisons before and after treatment were analysed using repeated measures of analysis of variance with Newman-Keuls test. For comparing plasma PGE2 and serum TxB2 values, a paired t test was used. A p value of <0.05 was considered significant. Correlation was expressed as Spearman’s correlation coefficient.
RESULTS
No amylase activity (<22 U/ml) was detected in any study sample, excluding significant salivary contamination.
Mean serum TxB2 concentrations ex vivo were reduced by 93.9% after treatment with ibuprofen (p<0.0001, fig 1A) but not after placebo (p = 0.29, fig 1B). The reduction in TxB2 concentration was more than 85% in all patients, indicating compliance with treatment. Following rofecoxib treatment there was a reduction in the LPS induced increase in plasma PGE2 concentrations compared with pretreatment values (p<0.0001, fig 2). This reduction was more than 80% in all patients, indicating compliance with treatment. Treatment with ibuprofen and rofecoxib was well tolerated.
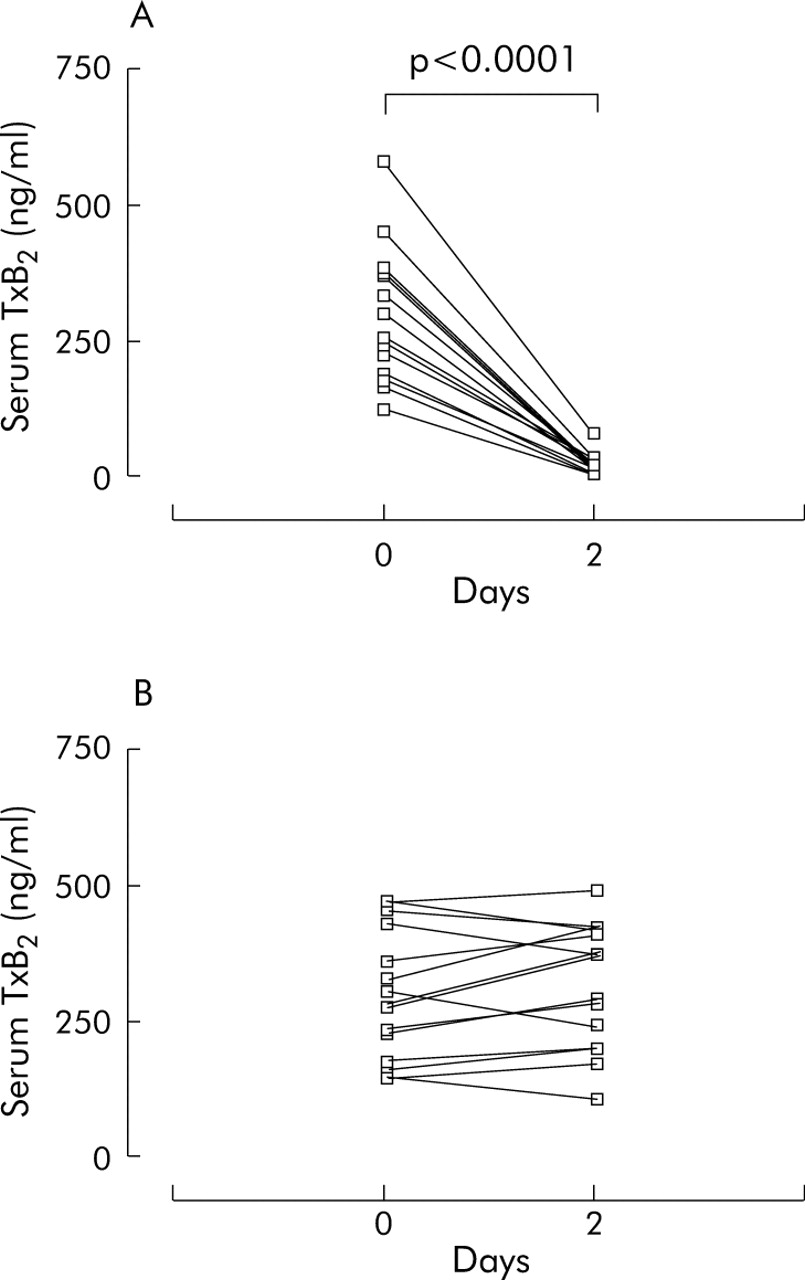
Serum thromboxane B2 (TxB2) concentrations ex vivo before (day 0) and after treatment (day 2) with (A) oral ibuprofen (400 mg four times a day) or (B) matched placebo for 2 days in patients with COPD (n = 14). Values are expressed as means.
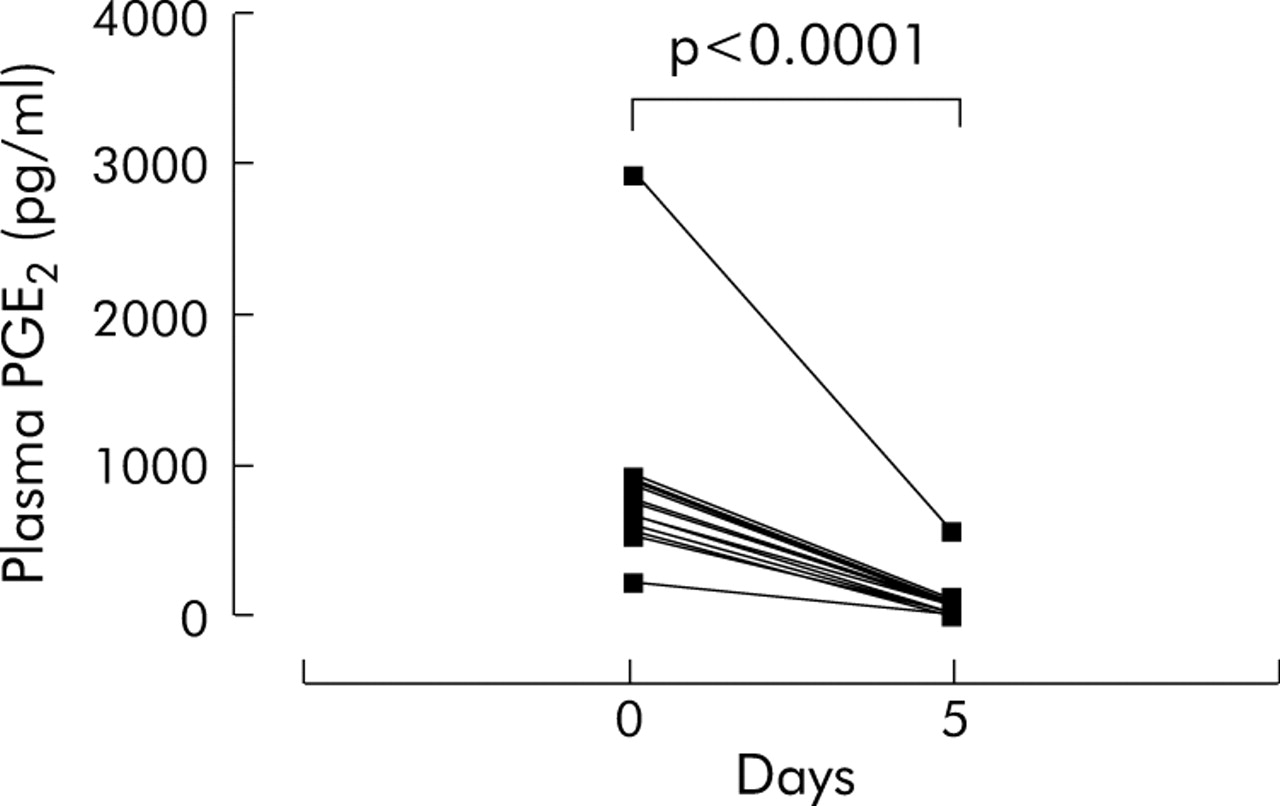
Plasma prostaglandin E2 (PGE2) concentrations after ex vivo platelet COX-2 activation with lipopolysaccharide (10 μg/ml) and COX-1 inhibition with aspirin (10 μg/ml) before (day 0) and after treatment (day 5) with oral rofecoxib (25 mg once a day for 5 days) in patients with COPD (n = 16) Values are expressed as means.
Exhaled breath condensate
Ibuprofen study
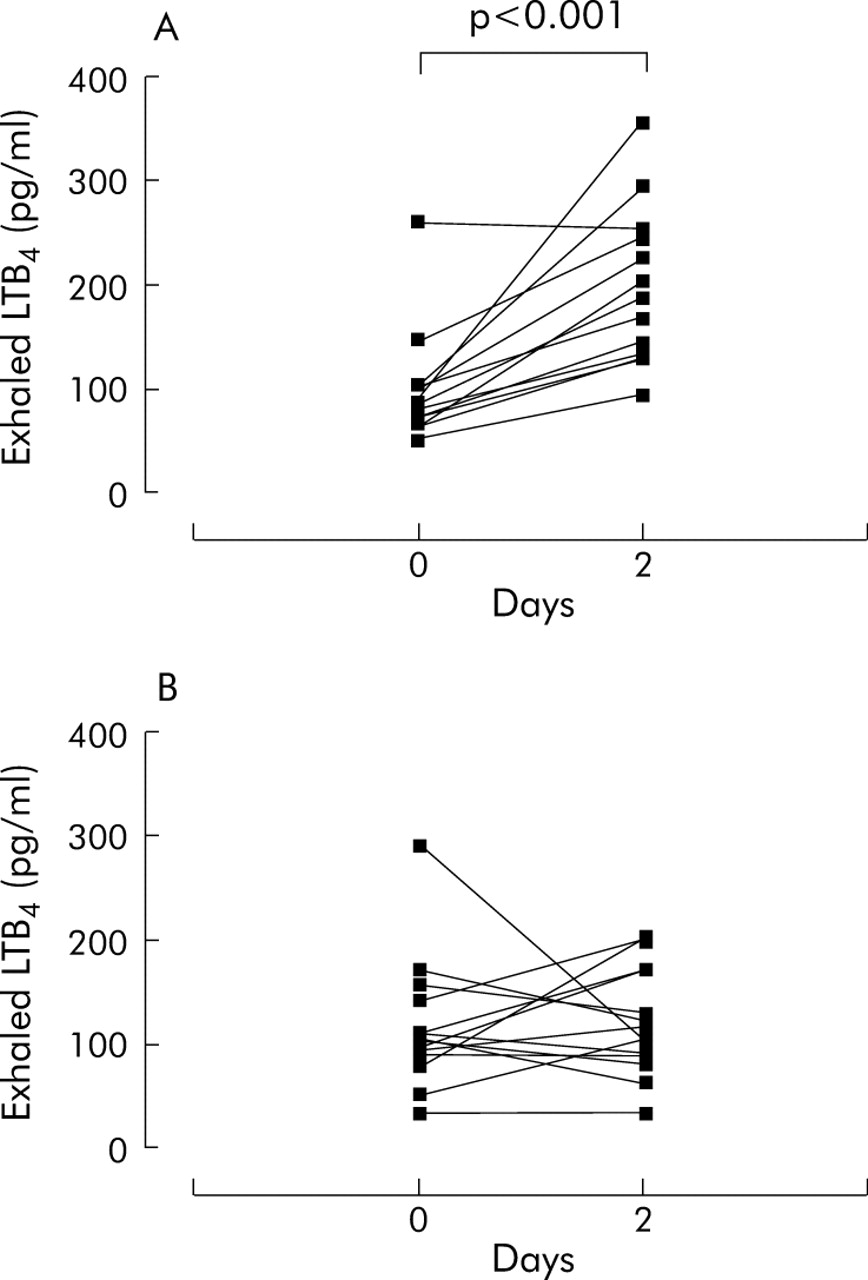
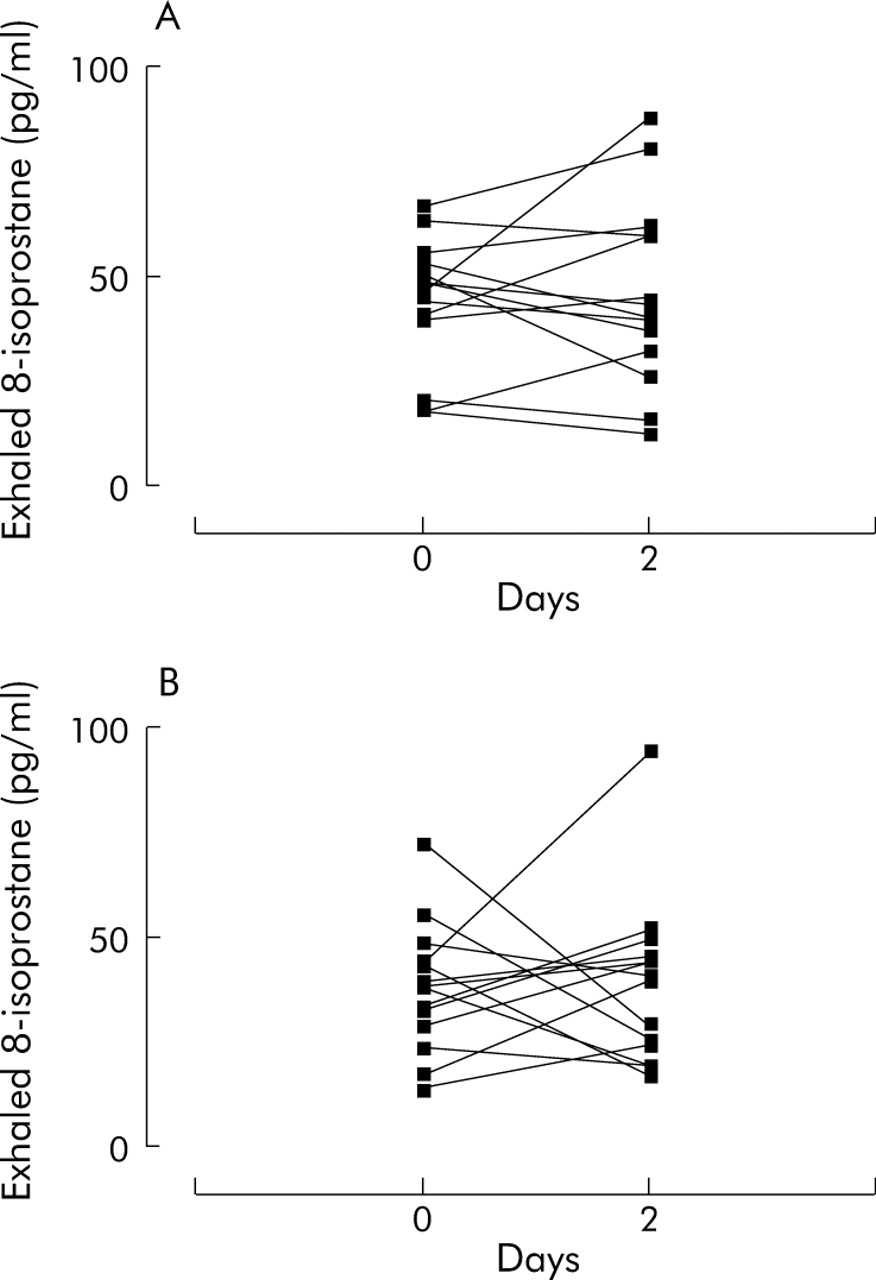
Exhaled LTB4 concentrations were increased after drug treatment (175.5 (128.8–231.5) pg/ml v 84.0 (70.0–98.5) pg/ml), p<0.001; fig 3A) but not after placebo (104.5 (92.8–126.5) pg/ml v 111.0 (91.0–150.5) pg/ml, p = 0.87; fig 3B). Exhaled PGE2 concentrations were reduced after treatment with ibuprofen (93.5 (84.0–105.5) pg/ml v 22.0 (15.0–25.5) pg/ml, p<0.0001; fig 4A) but not after placebo (88.0 (72.5–103.0) pg/ml v 95.5 (72.5–104.0) pg/ml, p = 0.49; fig 4B). Ibuprofen did not affect exhaled 8-isoprostane concentrations (ibuprofen: 47.9 (40.5–51.9) pg/ml pre-treatment v 42.2 (34.9–60.0) pg/ml post-treatment, p = 0.64, fig 5A; placebo: 38.3 (31.0–43.8) pg/ml pre-treatment v 40.6 (25.1–45.2) pg/ml post-treatment, p = 0.87, fig 5B).

Leukotriene B4 (LTB4) concentrations in exhaled breath condensate before (day 0) and after treatment (day 2) with (A) oral ibuprofen (400 mg four times a day) or (B) matched placebo for 2 days in patients with COPD (n = 14). Values are expressed as medians.

Prostaglandin E2 (PGE2) concentrations in exhaled breath condensate before (day 0) and after treatment (day 2) with (A) oral ibuprofen (400 mg four times a day) or (B) matched placebo for 2 days in patients with COPD (n = 14). Values are expressed as medians.
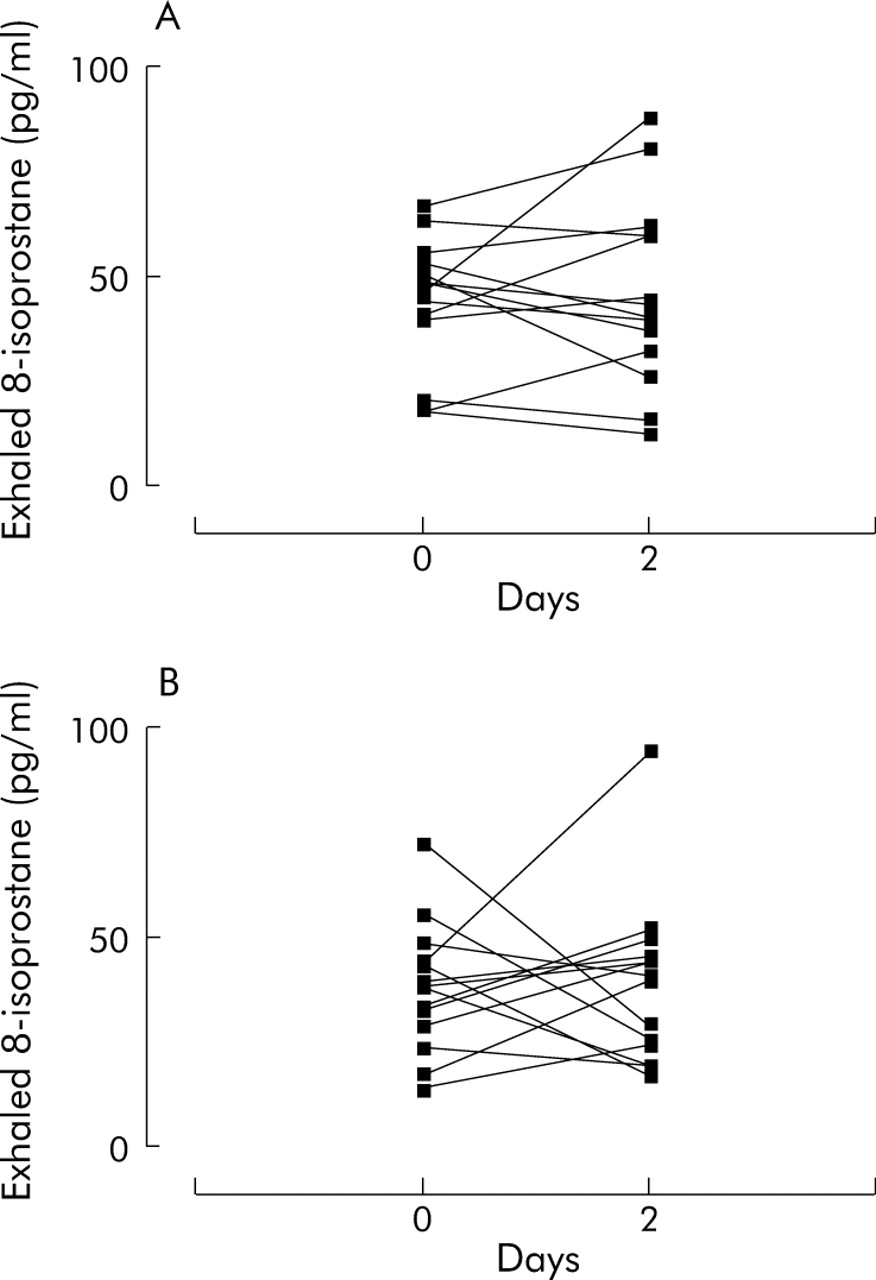
8-Isoprostane concentrations in exhaled breath condensate before (day 0) and after treatment (day 2) with (A) oral ibuprofen (400 mg four times a day) or (B) matched placebo for 2 days in patients with COPD (n = 14). Values are expressed as medians.
There was no correlation between exhaled eicosanoids and spirometric values. The intraclass correlation coefficient was 0.75 for LTB4 (p<0.001), 0.87 for PGE2 (p<0.0001) and 0.79 for 8-isoprostane (p<0.001).
Rofecoxib study
Rofecoxib had no effect on median exhaled LTB4 (pre-treatment 89.4 (81.8–116.4) pg/ml v post-treatment 83.8 (64.4–105.6) pg/ml, p = 0.53; fig 6A), PGE2 (pre-treatment 89.3 (75.5–100.5) pg/ml v post-treatment 91.5 (85.5–102.8) pg/ml, p = 0.23; fig 6B), or 8-isoprostane concentrations (pre-treatment 39.5 (33.0–46.5) pg/ml v post-treatment 39.5 (34.8–43.5) pg/ml, p = 0.93; fig 6C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) LTB4, (B) PGE2, and (C) 8-isoprostane concentrations in exhaled breath condensate in patients with COPD at baseline (day –14), before (day 0), and after treatment with oral rofecoxib 25 mg once a day for 5 days (day 5) in patients with COPD (n = 16). Values are expressed as medians.
There was a negative correlation between 8-isoprostane concentrations in EBC and Pao2 values at baseline (r = −0.67, p = 0.045, n = 16) (fig S3 available online at http://www.thoraxjnl.com/supplemental). There was no correlation between exhaled eicosanoids and spirometric values. There was no correlation between exhaled markers and either absolute or relative cell counts in sputum. The intraclass correlation coefficient was 0.67 (p<0.001) for LTB4, 0.82 (p<0.0001) for PGE2, and 0.75 (p<0.0001) for 8-isoprostane.
Pulmonary function tests
Ibuprofen study
Treatment with ibuprofen or placebo had no effect on FEV1 (p = 0.61), FVC (p = 0.26), and FEV1/FVC ratio (p = 0.99) (see tables S1 and S2 available online at http://www.thoraxjnl.com/supplemental).
Rofecoxib study
Rofecoxib had no effect on FEV1 (p = 0.45), FVC (p = 0.52), and FEV1/FVC ratio (p = 0.82) (see table S3 available online at http://www.thoraxjnl.com/supplemental).
Sputum induction
Rofecoxib study
Three samples from one patient had more than 50% squamous cell contamination and were excluded from analysis. Differential or absolute counts of any cell type at baseline and after the run-in period were similar (see table S4 available online at http://www.thoraxjnl.com/supplemental).
Rofecoxib had no effect on absolute (total cells, p = 0.55; macrophages, p = 0.77; neutrophils, p = 0.77; lymphocytes, p = 0.42; eosinophils, p = 0.77) or differential sputum cell counts (squamous cells, p = 0.77; macrophages, p = 0.31; neutrophils, p = 0.59; lymphocytes, p = 0.53; eosinophils, p = 0.69) (see table S4 available online at http://www.thoraxjnl.com/supplemental).
Arterial blood gases
Rofecoxib study
In 10 out of 16 patients arterial blood gas measurements were performed on visits 1, 2, and 3. Six patients who participated in the study refused to have a second arterial blood gas measurement. In the 10 patients who had three arterial blood gas measurements the mean Pao2 was increased by 4.2 mm Hg after rofecoxib, although statistical significance was not reached (pre-treatment 73.3 (1.8) mm Hg; post-treatment 77.5 (3.3) mm Hg, p = 0.42) (see fig S4A available online at http://www.thoraxjnl.com/supplemental). Rofecoxib had no effect on Paco2 or pH values (see fig S4B and C in online supplement).
DISCUSSION
We have investigated the effects of COX inhibition on exhaled LTB4, PGE2, and 8-isoprostane concentrations in patients with COPD. All patients complied with treatment as reflected by a reduction in ex vivo serum TxB2 concentrations after ibuprofen of more than 85% and inhibition of LPS induced increase in plasma PGE2 values after rofecoxib of more than 80% in each patient. The specificity of the enzyme immunoassay for LTB4 and the radioimmunoassays for 8-isoprostane and PGE2 has been shown previously by RP-HPLC.16,17 Day to day repeatability for exhaled eicosanoid measurements is acceptable, as indicated by their intraclass correlation coefficients consistent with previous findings.23 In a randomised, double blind, placebo controlled, crossover study, ibuprofen, a non-selective COX inhibitor, given orally at a dose of 1600 mg/day for 2 days, increased LTB4 concentrations and decreased PGE2 concentrations in EBC in patients with stable COPD. By contrast, in a different study of open label design, oral administration of rofecoxib (25 mg/day for 5 days), a selective COX-2 inhibitor, had no effect on these eicosanoids. Other authors have reported increased LTB4 concentrations in bronchoalveolar lavage (BAL) fluid from allergic COX-1 deficient mice compared with allergic wild type and COX-2 deficient mice.24 Taken together, these data indicate that COX-1 inhibition can divert arachidonic acid to other metabolic products (such as leukotrienes) under conditions of increased lung inflammation. LTB4 is a potent chemoattractant for neutrophils which have an important pathophysiological role in COPD.25 Increased exhaled LTB4 concentrations in patients with COPD treated with ibuprofen might indicate that airway inflammation in these patients is increased after non-selective COX inhibition. These effects are not observed after rofecoxib, which indicates that selective COX-2 inhibitors might be more tolerated than other NSAIDs in patients with COPD. However, the lack of administration of a non-selective and a selective COX-2 inhibitor to the same group of patients and the open label uncontrolled design of the rofecoxib study limit the strength of these findings and preclude definitive conclusions.
In the ibuprofen study six of the 14 patients were on inhaled corticosteroids, whereas all the rofecoxib study group patients were steroid naïve. A previous observational study showed that inhaled steroids had a limited, if any, effect on exhaled eicosanoids in patients with COPD.8 However, studies are needed to address formally the influence of steroid treatment on exhaled eicosanoids in patients treated with COX inhibitors. As ibuprofen decreases exhaled PGE2 concentrations in patients with COPD while rofecoxib does not, the present study indicates that COX-1 is primarily responsible for exhaled PGE2 production. Similar PGE2 levels in BAL fluid were reported in allergic wild type and COX-2 deficient mice.24 By contrast, prostaglandin synthesis in allergic guinea pig lungs in vitro has been reported to be significantly dependent on COX-2.26 This discrepancy may partially be explained by in vitro/in vivo differences in expression and regulation of COX isoforms24 and/or differences in the inflammatory process (allergen challenge v COPD). Data on the effect of COX inhibitors in the present studies should be interpreted cautiously as COPD severity was different in the rofecoxib and ibuprofen study group patients (moderate and severe, respectively). Further studies are required to clarify whether the effect of COX inhibitors on exhaled eicosanoids in COPD is affected by disease severity, whether the difference between the action of the two drugs is related to COX independent mechanisms, and the long term effect of COX inhibitors on exhaled eicosanoids in patients with COPD. Findings on the functional consequences of COX inhibition on airway inflammation are controversial,26,27 possibly due to the fact that COX inhibitors abrogate the synthesis of both pro- and anti-inflammatory prostaglandins (PGD2v PGE2).28 The lack of effect of ibuprofen and rofecoxib on exhaled 8-isoprostane concentrations indicates that this compound is primarily formed independently of the COX pathway.7
The values of exhaled eicosanoids in our study are given per ml EBC, as in most of the published studies on exhaled biomarkers. This approach may have limitations since many factors are likely to affect differentially the volume of EBC and the concentrations of various compounds in it, including differences in EBC collection, sample storage, analytical techniques, and disease severity.11 As pointed out by Effros and co-workers, part of the variation in the concentrations of non-volatile compounds in EBC can be related to differences in the dilution of respiratory droplets by water vapour.29 The lack of correlation between structurally related compounds such as 8-isoprostane and PGE2 observed in this study and the selective increase of leukotrienes (LTB4v LTE4) in the single subject previously reported8 do not seem to support this evidence. However, reference indicators, such as the measurement of conductivity as proposed by Effros and co-workers,30 should be used in future studies aimed at quantifying exhaled eicosanoids. At present, because of the lack of a standardised procedure for EBC collection and validated analytical methods, comparisons of data obtained in different laboratories are difficult.11 The fact that eicosanoid concentrations in EBC are not more diluted than those observed in BAL fluid might indicate that these compounds are somewhat volatile and reach the EBC in the gas phase. However, recent data indicate that LTB4 is not volatile (P Montuschi, unpublished data). The physical and chemical properties of eicosanoids in EBC are largely unknown and require further research. EBC analysis is currently more reliable for measuring relative values than for determining absolute levels of inflammatory mediators.
No changes were seen in lung function tests or sputum cell counts after short term treatment with oral ibuprofen or rofecoxib at therapeutic doses. Similarly, 1 week of treatment with oral celecoxib (200 mg twice daily), another selective COX-2 inhibitor, did not affect bronchial responsiveness in asthmatic patients.31 However, possible effects on lung function and/or sputum cell counts after longer treatment with COX inhibitors cannot be ruled out. The mean Pao2 was increased by 4.2 mm Hg after rofecoxib, although statistical significance was not reached (p = 0.42). The biological significance of these findings is currently unknown, as is the effect on Pao2 of long term treatment with selective COX-2 inhibitors.
In conclusion, short term non-selective COX inhibition increases LTB4 and reduces PGE2 concentrations in EBC in patients with COPD, whereas selective COX-2 inhibition does not seem to have these effects. These findings indicate that exhaled PGE2 is primarily derived from COX-1 activity and that COX-1 inhibition may redirect arachidonic acid metabolism towards the 5-lipoxygenase pathway. However, controlled studies with non-selective and selective COX inhibitors in the same group of patients with COPD are required to draw definitive conclusions.
REFERENCES
Supplementary materials
The figures are available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Figures 1-4.
The appendix is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Online supplement.
Footnotes
-
The ibuprofen study was funded by Imperial College, School of Medicine at the National Heart and Lung Institute, London, UK. The rofecoxib study was funded by Merck, Sharp & Dohme.
-
PM, FM, PP, SV, LL, GC, PJB, and GC have no competing interests. They have no financial and/or personal relationships with other people or organisations that could inappropriately influence this work.
-
This work was performed at Imperial College, School of Medicine, National Heart and Lung Institute, London, UK and at the Catholic University of the Sacred Heart, Rome, Italy.