Article Text

Abstract
Background: The Global Initiative for Obstructive Lung Disease (GOLD) has defined chronic obstructive pulmonary disease (COPD) as a post-bronchodilator ratio of forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC) of <0.7. In the first general population based study to apply post-bronchodilator values, the prevalence and predictors of GOLD defined COPD were assessed and the implications of β2 agonist reversibility testing examined.
Methods: Based on a random population sample, 2235 subjects (77%) aged 26–82 years performed spirometric tests before and 15 minutes after inhaling 0.3 mg salbutamol.
Results: The prevalence of GOLD defined COPD was 7.0% (95% confidence interval (CI) 5.9 to 8.0). This estimate was 27% lower than COPD defined without bronchodilatation. One percent of the population had severe or very severe COPD. Compared with women, men had 3.1 (95% CI 2.1 to 4.8) times higher odds for COPD. Subjects with a smoking history of more than 20 pack years had an odds ratio (OR) of 6.2 (95% CI 3.4 to 11.0) for COPD relative to never-smokers, while subjects older than 75 years had an OR of 18.0 (95% CI 9.2 to 35.0) relative to those below 45 years. Subjects with primary education only had an OR of 2.8 (95% CI 1.4 to 5.3) compared with those with university education. Subjects with body mass index (BMI) <20 kg/m2 were more likely than subjects with BMI 25–29.9 kg/m2 to have COPD (OR 2.4, 95% CI 1.1 to 5.3). The adjusted proportion of COPD attributable to smoking was 68%.
Conclusions: These results indicate that community programmes on prevention of COPD should focus on anti-smoking, nutritional aspects, and socioeconomic conditions. The effect of β2 reversibility testing on prevalence estimates of COPD was substantial.
- BMI, body mass index
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- chronic obstructive pulmonary disease
- prevalence
- Global Initiative for Obstructive Lung Disease (GOLD)
- bronchodilatation
- epidemiology
Statistics from Altmetric.com
- chronic obstructive pulmonary disease
- prevalence
- Global Initiative for Obstructive Lung Disease (GOLD)
- bronchodilatation
- epidemiology
The recent international guidelines from the Global Initiative for Chronic Obstructive Lung Disease (GOLD)1,2 have facilitated comparison of study results regarding chronic obstructive pulmonary disease (COPD). The new joint position paper from the European Respiratory Society (ERS) and the American Thoracic Society (ATS)3 has further enhanced this consensus through advocating the same disease definition.
GOLD defines COPD through post-bronchodilatation spirometric testing as a ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) of <0.7. The use of post-bronchodilator values is essential because of the mainly irreversible airflow limitation that characterises COPD.2,4 The prevalence of COPD using pre-bronchodilator values gives an overestimation, especially among young adults.4
This is the first study to present the prevalence and predictors of GOLD defined COPD in a general adult population. Although several population based studies claim to present prevalence estimates of COPD according to the GOLD criteria,5–9 none of these has defined COPD with post-bronchodilator spirometric values for adults with a broad age range. The need for, and importance of, correct use of GOLD guidelines with post-bronchodilator values has recently been stressed.4,10
The main objectives of the study were to estimate the prevalence and predictors of GOLD defined COPD in a general adult population. We also wanted to investigate how the bronchodilatation test affected the prevalence estimates, and whether the associations between disease and risk factors remained the same before and after bronchodilatation.
METHODS
Subjects
In 1985 there were 267 403 subjects aged 15–70 years living in Hordaland County, Norway. A random sample (N = 4992) was invited to answer a respiratory health questionnaire; 75% of the participants (N = 3370) lived in Bergen and 11 surrounding municipalities. Of 2912 subjects still living in the study area in 1996–7, 2401 (82%) participated in a follow up study. Acceptable spirometry with reversibility testing was achieved in 2235 (77%, fig 1). The most frequent reason for unsuccessful spirometric testing was unwillingness to inhale a β2 agonist (3.0%).
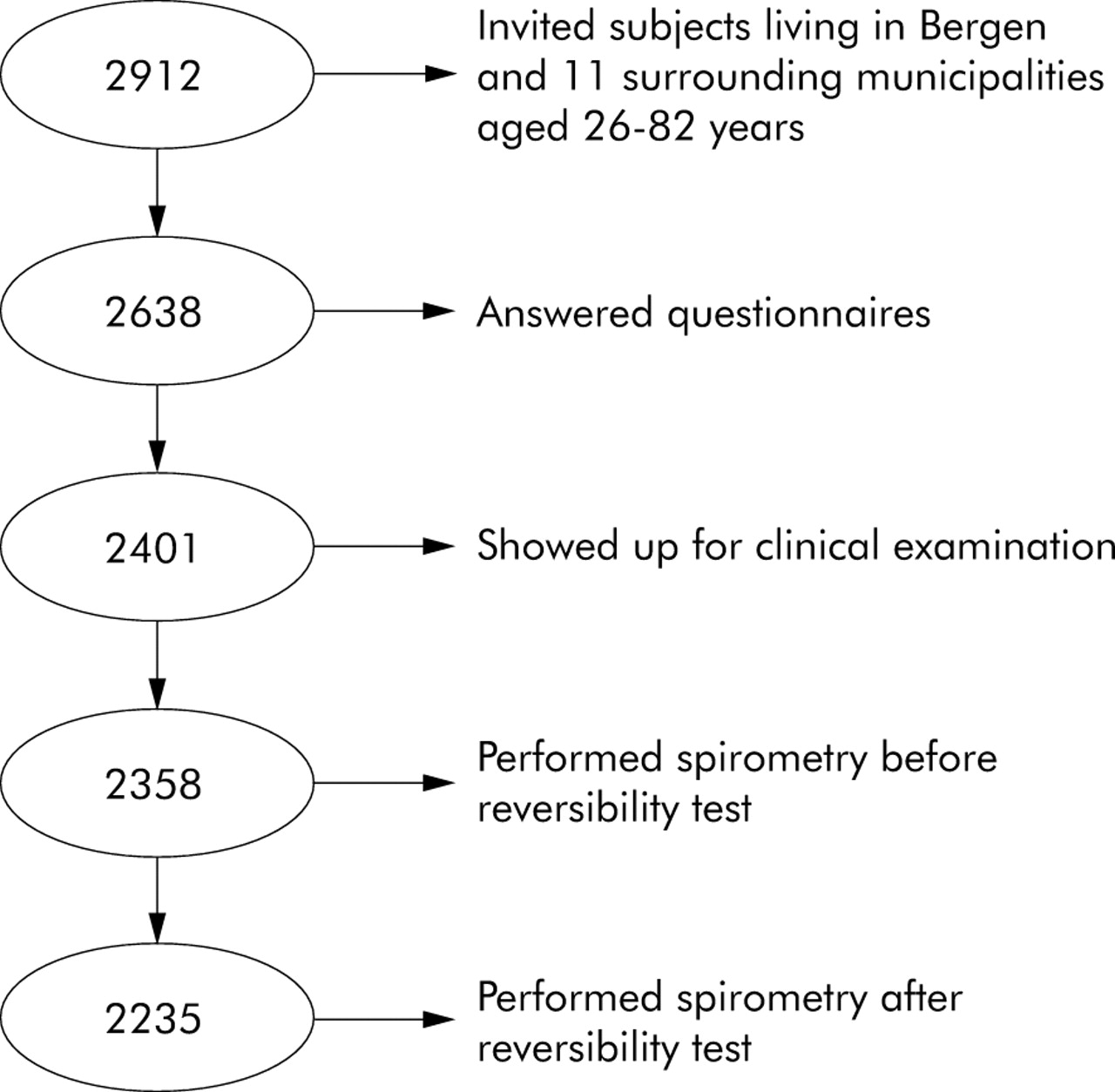
Flow chart of sample performing spirometry with reversibility test in the Hordaland County Cohort Study 1996–7.
Respiratory symptoms (cough, dyspnoea, wheeze) and diseases (asthma, chronic bronchitis, emphysema and COPD), occupational dust or gas exposure, educational level, and smoking habits were registered in self-administered questionnaires.11 Carboxyhaemoglobin (HbCO) was measured for each participant. Almost all current smokers (91%) and only 4% of non-smokers had HbCO >1.7%.
One pack year was defined as 20 cigarettes a day for 1 year. Occupational dust or gas exposure was defined as an affirmative answer to the question “Have you ever had a work place with much dust or gas in the air?” Information on the highest completed educational level was classified into three categories: (1) 9 year compulsory school; (2) continuation school, lower secondary school, upper secondary school, or technical school; (3) college or university.12 Height and weight were registered and body mass index (BMI) was categorised into four groups: <20 kg/m2, 20–24.9 kg/m2, 25–29.9 kg/m2, and ⩾30 kg/m2. Residential area was divided into urban (Bergen) and rural (11 surrounding municipalities). Information on BMI, pack years, educational level, and occupational exposure was lacking for 7, 48, 26 and 50 subjects, respectively.
The study was approved by the regional committee of medical research ethics.
Spirometry and reversibility testing
FVC and FEV1 were measured with Gould 2100 pulmonary function equipment13 according to the ATS criteria.14,15 Spirometric tests were performed before and 15 minutes after inhalation of salbutamol powder from a Turbuhaler. Each dose was 0.1 mg, and three inhalations were administered 1–2 minutes apart, giving a total dose of 0.3 mg salbutamol.
We estimated COPD according to the GOLD guidelines as post-bronchodilator FEV1/FVC of <0.7.2 In order to analyse the effect of reversibility testing on disease definition, we also estimated COPD defined without bronchodilatation. Subjects were grouped into four categories based on their pre- and post-bronchodilator FEV1/FVC ratio combinations.
Severity of disease was defined by level of FEV1 as percentage predicted.2 Predicted values of FEV1 were assessed using equations from a Norwegian reference population.16
Statistical analysis
Analyses were performed with Stata 8.0 and SPSS 12.0 for Windows.17,18 All p values were two sided and values below 0.05 were considered statistically significant if not stated otherwise. Sex, age, BMI, smoking habits, pack years, educational level, occupational exposure, and residential area were analysed as risk factors for COPD. All possible two way interaction effects from the risk factors in relation to post-bronchodilator FEV1/FVC were examined in logistic regression analyses. The significance level for the interaction effects was set to 0.01. Adjusted odds ratios (OR) and 95% confidence intervals (CI) for each risk factor were estimated in a backwards stepwise logistic regression analysis.
Adjusted attributable fractions with confidence intervals were estimated for smoking and occupational exposure to airborne agents. Attributable fraction was defined as the proportion of prevalence in the total population that could have been avoided if the exposure of interest had been removed.19 The definition presupposed that all other exposures remained stable.
One way ANOVA with Bonferroni tests was performed for multiple pairwise comparisons for the four combinations of pre- and post-bronchodilatation spirometry results. Mean pre- and post-bronchodilator FEV1, FVC, and FEV1/FVC were compared across the four groups.
RESULTS
Characteristics of study population
A similar number of men and women participated in the study (table 1). The mean (SD) age of the study population was 49.8 (14.7) years (range 26–82). Mean (SD) BMI was 25.6 (4.0) kg/m2. One third of the participants smoked on a daily basis, while almost 40% were never smokers. Female ever smokers had smoked a mean (SD) of 12 (10) pack years, while male ever smokers had smoked as much as 17 (14) pack years. Approximately one out of five ever smokers had smoked more than 20 pack years. Eighteen percent had completed primary school only, while 22% had university education. Almost half of the study population, twice as many men as women, had been occupationally exposed to dust or gas. Almost 70% of the participants lived in the urban municipality of Bergen.
Characteristics of study population by sex, age, body mass index, smoking habits, pack years, occupational exposure and residential area in an adult general Norwegian population, 1996–7
Prevalence estimates
The prevalence of GOLD defined COPD was 7.0% (table 2). The prevalence was higher in men than in women, and it increased with increasing age and decreasing BMI. COPD was more frequent in ever smokers than in never smokers, and increased in a dose-response manner with pack years. Furthermore, the prevalence was higher in subjects with lower education and in those who had been occupationally exposed to dust or gas. The prevalence of COPD was roughly equal in rural and urban residential areas.
Prevalence of COPD (FEV1/FVC <0.7) defined before and after bronchodilatation in a general adult population in 1996–7 by sex, age, body mass index, smoking habits, pack years, occupational exposure, and residential area
The prevalence of GOLD defined COPD was 27% lower than when COPD was defined before β2 agonist reversibility testing (table 2). The reduction in the prevalence of COPD after β2 inhalation was largest in younger age groups and in never smokers. After bronchodilatation, 69 subjects (32% of the pre-bronchodilatation defined prevalent COPD cases) converted from being a COPD case to being a non-case, and 11 subjects (0.5% of the pre-bronchodilatation defined non-cases) converted from being a non-case to being a case. The prevalence of COPD according to GOLD severity stages was 1.8% (95% CI 1.3 to 2.4) mild, 4.2% (95% CI 3.3 to 5.0) moderate, 0.9% (95% CI 0.5 to 1.2) severe, and 0.1% (95% CI 0.0 to 0.3) very severe. This implies that 86% of the COPD cases in our community were mild or moderate.
Changes in pulmonary function after inhalation of adrenergic bronchodilator
Most of the study population maintained a high FEV1/FVC ratio both before and after reversibility testing. This was true for 90% of the population, while 6.5% had FEV1/FVC <0.7 both before and after reversibility testing, 3% had a reversible airflow obstruction with a low ratio before bronchodilatation and a high ratio after, and 0.5% had an initial high ratio which decreased after bronchodilatation (table 3). For the 2010 subjects who maintained an FEV1/FVC ratio of ⩾0.7, FVC remained stable from pre- to post-bronchodilator spirometric testing, while FEV1 increased with a mean of 73 ml. Among subjects with low baseline FEV1/FVC, all pulmonary function variables increased with post-bronchodilator spirometric testing. In 11 subjects who converted from having an FEV1/FVC ratio >0.7 to having a ratio <0.7, FEV1 decreased slightly (−48 ml on average) while FVC increased considerably (269 ml) after reversibility testing. Reversibility of FEV1 was highest in the group that went from being a pre-bronchodilator case to a post-bronchodilator non-case (199 ml), with a mean of 122 ml in those who maintained a low FEV1/FVC ratio both before and after inhalation of adrenergic bronchodilator (table 3). The Bonferroni multiple pairwise comparison test showed that reversibility and FEV1/FVC both before and after reversibility testing differed significantly between all four groups (results not shown).
One way ANOVA and mean (SD) FEV1, FVC, and FEV1/FVC before and after reversibility test by all combinations of pre- and post-bronchodilator defined COPD in a general adult population in 1996–7
Comparison of subjects with a continuous low FEV1/FVC ratio and subjects who went from being pre-bronchodilator cases to post-bronchodilator non-cases showed that GOLD defined COPD cases were older than reversible airflow obstruction cases (mean age 63 v 55 years, p<0.001, results not shown), and that significantly more GOLD defined COPD cases reported chronic cough and smoking than those who converted after inhalation of adrenergic bronchodilator.
Risk factors for GOLD defined COPD
There were no significant two way interaction effects from any of the risk factors. The prevalence of COPD increased substantially with age, and more so after bronchodilatation than before (fig 2). Men had 3.3 times higher odds for COPD than women after adjusting for age, BMI, smoking, education, occupational exposure, and residential area (fig 3). An inverse association was observed between COPD and increasing BMI, as the odds ratio for COPD among subjects with BMI <20 kg/m2 was 2.4 relative to subjects with BMI 25–29.9 kg/m2 (fig 3).

Adjusted odds ratios (OR) and 95% confidence intervals (95% CI) for COPD (FEV1/FVC <0.7) defined before and after bronchodilatation (GOLD defined) in a general adult population in 1996–7 by age, smoking habits, and pack years. Reference categories: 26–44 years, never smokers, 0 pack years. Variables are adjusted for each other as well as for sex, BMI, education, occupational exposure and residential area.

{kind=link}
{kind=link}
{kind=link}
Adjusted odds ratios (OR) and 95% confidence intervals (95% CI) for COPD (FEV1/FVC <0.7) defined before and after bronchodilatation (GOLD defined) in a general adult population in 1996–7 by sex, body mass index, education, occupational exposure, and residential area. Reference categories: women, BMI 25—29 kg/m2, university, no occupational exposure, rural residential area. All variables are adjusted for each other as well as for age and smoking habits.
Current smokers had 4.2 times higher odds for COPD than never smokers, and ex-smokers had 3.6 times higher odds for disease than those who had never smoked (fig 2). There was a clear dose-response relationship between smoking and COPD. Although smoking was a significant predictor for COPD both before and after β2 agonist reversibility testing, the trend was stronger after bronchodilatation than before.
The odds ratio for the prevalence of COPD among subjects with a primary educational level was 2.9 compared with those who had completed university education. Neither occupational exposure to gas or dust nor residential area was significantly associated with GOLD defined COPD in this study population. The proportion of GOLD defined COPD attributable to smoking was 68% after adjustment for sex, age, BMI, education, occupational exposure to dust or gas, and residential area (results not shown). Less than 6% of COPD in this population could be ascribed to occupational exposure to dust or gas.
Although analyses of interaction effects revealed no significant two way interaction effects from any of the risk factors, separate explorative analyses for men and women were performed to examine whether the risk factor profiles differed (results not shown). The analyses indicated that women may be more susceptible to heavy smoking and that the relationships between low BMI and lower education, on the one hand, and COPD on the other, may be valid primarily for men.
DISCUSSION
The prevalence of GOLD defined COPD was 7% in this general adult population. The reduction in prevalence after bronchodilatation relative to before was 27%. The predictors for COPD remained the same whether disease was defined with or without β2 agonist reversibility testing, although the strength of the associations varied. Age and smoking were substantially stronger predictors for COPD when defined according to the GOLD criteria than when it was defined without bronchodilatation. The adjusted proportion of GOLD defined COPD attributable to smoking was 68%. Compared with COPD defined before bronchodilatation, fewer young never smokers with reversible airflow limitation would be included as prevalent COPD cases when applying the GOLD post-bronchodilator criteria.
Theoretically, non-response bias could influence prevalence estimates. However, we do not have any reason to suspect important systematic differences between responders and non-responders because of the results from previous studies of the present cohort.20,21 Based on characteristics among the 1985 participants, middle aged subjects in paid employment were over-represented among the responders in 1996–7.20 This indicated a tendency for responders to have higher socioeconomic status than non-responders. However, non-responders and responders in 1996–7 did not differ with regard to the prevalence of morning cough, chronic cough, breathlessness, and wheezing in 1985. A “survivor bias” where only the most healthy of the 1985 participants would be part of the 1996–7 study was therefore found to be unlikely.
The prevalence estimates in our study were based exclusively on spirometric results. Both GOLD and the ATS/ERS guidelines recommend that the presence of respiratory symptoms and a history of exposure to risk factors should be considered in addition to post-bronchodilator spirometric results when diagnosing COPD.3,22 We examined the presence of chronic cough, sputum, dyspnoea, and physician diagnosed COPD, emphysema, bronchitis and asthma in our study population. 73% of the GOLD defined COPD cases were symptomatic and/or had a physician diagnosed respiratory disease. Nearly all the COPD cases identified in our study were mild or moderate cases according to the GOLD severity stages. A recent patient study showed that COPD patients seek medical advice primarily in advanced stages of the disease.23 Performing routine spirometric tests according to GOLD recommendations could facilitate earlier detection of COPD and those at risk for COPD.
The Estudio Epidemiológico de la EPOC en España (IBERPOC) and the Obstructive Lung Disease in Northern Sweden (OLIN) studies both performed reversibility testing on subjects with initial airflow limitation.24,25 Initial airflow limitation was defined in the Spanish study as FEV1/FVC <88% of predicted in men and <89% of predicted in women, while in the Swedish study it was defined as FEV1/FVC <0.7 or FEV1 <90% of predicted. For subjects who were not defined as having airflow limitation, spirometric values without bronchodilatation were used in the analyses. In the IBERPOC population with an age range of 40–69 years, the prevalence of ERS defined COPD was 9.1% with smoking, male sex, and age as significant predictors. In the OLIN study three narrow age cohorts (46–47 years, 61–62 years, and 76–77 years) were examined in 1996–7.25 The prevalence of GOLD defined COPD was 14.3%, twice as high as in our study. However, to fulfil the GOLD criteria, reversibility testing should have been performed in all subjects and not just in those with a low initial FEV1/FVC ratio. Although in most cases the FEV1/FVC ratio is higher after than before reversibility testing, a considerable number of subjects will have a lower ratio after bronchodilatation than before, as observed in our study. Furthermore, age differences with a mean of 57.3 years in the OLIN study and 49.8 years in the present study could also partly explain the discrepancy between the prevalence estimates. When we included only subjects aged 46–77 years in our analyses, the GOLD defined COPD prevalence was 9.7% (95% CI 7.9 to 11.4) (results not shown).
International comparison of the prevalence of COPD is difficult until more studies provide estimates of COPD according to GOLD and ATS/ERS criteria with appropriate post-bronchodilator spirometric data. The ongoing Burden of Lung Disease (BOLD) initiative26 will facilitate direct comparison of the prevalence of GOLD defined COPD across nations. The BOLD initiative is currently being carried out in study centres in South America, North America, Australia, and Europe.
The GOLD initiative specifies the need for reversibility testing but does not specify in detail a standardised test procedure.2 In our study post-bronchodilator spirometric testing was performed 15 minutes after inhalation of 0.3 mg salbutamol from a Turbuhaler. In the OLIN study 0.8 mg salbutamol was inhaled from a Discus, while in the IBERPOC study two inhalations of salbutamol were administered using an inhalation chamber.24,25 Dose, medication, equipment, and time interval from drug inhalation to post-bronchodilator spirometric testing should be included in the guidelines. In addition, comparisons of the prevalence of COPD severity demand identical reference values.
Our study supports previous observations that male sex, old age, smoking, low BMI, and lower education are significant predictors for COPD.12,27,28 In our study subjects older than 75 years had a 19 times higher risk for COPD than subjects below the age of 45 years. The strength of this age trend may partly be due to the use of the fixed FEV1/FVC cut off point of 0.7. The age related decline in FEV1 accelerates in the elderly, and normal ageing of the lung resembles the development of COPD even in subjects without risk factors for COPD.7 However, all the 34 prevalent COPD cases older than 75 years in our study reported respiratory symptoms.
Occupational exposure to dust, gases, or fumes is a known risk factor for COPD.29 However, in our study self-reported exposure to airborne dust or gas was not a significant predictor of COPD. A study in 1987–8 from the same area found a positive, but not significant, association between having a job with a high degree of airborne exposure and spirometric airflow limitation.14 A longitudinal study from the same area also found a positive but not significant association between occupational exposure and COPD.30 A high awareness of the relationship between occupational exposures and chronic lung disease in our community, as well as advanced levels of national safety surveillance concerning occupational environment, may partly explain our finding.
Becklake and Kauffmann31 have stressed the importance of sex-specific analyses in studies of airway disease. Sex-specific analyses revealed mainly the same risk profiles for men and women (results not shown). The analyses nevertheless indicated that women who had smoked more than 20 pack years were more inclined to develop COPD than men who had smoked more than 20 pack years. In addition, the sex-specific results suggest that the relationships between low BMI and lower education, on the one hand, and COPD on the other, may be valid primarily for men. Low BMI was significantly associated with COPD primarily in men. The Tucson study found that being underweight was a predictor for emphysema, while obesity was a predictor for self-reported chronic bronchitis.32 Subjects were categorised as having emphysema or chronic bronchitis if they reported that they had a physician confirmed diagnosis of such disease in a self-administered questionnaire. In our study, self-reported physician diagnosed emphysema was associated with a low BMI in men, and self-reported physician diagnosed bronchitis was associated with a high BMI in women (p<0.05, results not shown). This sex difference regarding the association between BMI and the prevalence of COPD may therefore be due to unequal distribution of COPD phenotypes in men and women. However, whether BMI is a predictor for or a result of COPD is difficult to assess with a cross sectional study design. The predictive value of BMI should be investigated in a population based follow up study.
In conclusion, the GOLD defined prevalence of COPD in a general adult community was 7%. This estimate was reduced by as much as 27% when the GOLD post-bronchodilator criterion was not applied. Predictors of COPD remained the same regardless of β2 agonist reversibility testing, but smoking and age were stronger predictors after bronchodilatation than before. Two thirds of the prevalent cases could have been prevented if all subjects in this general adult population were non-smokers.
Acknowledgments
The authors thank respiratory laboratory technician Lene Svendsen, Centre for Clinical Research for statistical advice and office facilities, and Geir Egil Eide, Tomas Eagan, Sverre Lehmann and Roy Miodini Nilsen for valuable comments.
REFERENCES
Footnotes
-
Published Online First 5 August 2005
-
This survey was funded by the Royal Norwegian Council for Scientific and Industrial Research and the Norwegian Research Council.
-
Competing interests: None declared.
-
The authors thank Astra Zeneca, Norway for giving them the opportunity to use salbutamol powder by Turbuhaler.