Article Text

Abstract
Background Factors involved in the regulation of muscle mass in chronic obstructive pulmonary disease (COPD) are still poorly understood. Comparing the signalisation involved in muscle mass regulation between two muscles with different levels of activation within the same subjects is an interesting strategy to tease out the impact of local (muscle activity) versus systemic factors in the regulation of muscle mass. A study was undertaken to measure and compare the protein levels of p-AKT, AKT, Atrogin-1, p-p70S6K, p-4E-BP1, p-GSK3β as well as the mRNA expression of Atrogin-1, MuRF1 and FoxO-1 in the quadriceps and the diaphragm of 12 patients with COPD and 7 controls with normal lung function.
Methods Diaphragm biopsies were obtained during thoracic surgery and quadriceps samples were obtained from needle biopsies. Protein content and mRNA expression were measured by western blot and quantitative PCR, respectively.
Results Increased mRNA expressions of Atrogin-1, MuRF1 and FoxO-1 were found in the quadriceps compared with the diaphragm only in patients with COPD. The quadriceps/diaphragm ratio for MuRF1 was higher in COPD. The protein level of p-p70S6K was decreased in the quadriceps compared with the diaphragm in patients with COPD. The quadriceps/diaphragm ratios of p-p70S6K and p-GSK3β were lower in patients with COPD than in controls.
Conclusions These results indicate a greater susceptibility to a catabolic/anabolic imbalance favouring muscle atrophy in the quadriceps compared with the diaphragm in patients with COPD. The balance between the atrophy and hypertrophy signalling is inhomogeneous between respiratory and lower limb muscles, suggesting that local factors are likely to be involved in the regulation of muscle mass in COPD.
- Chronic obstructive pulmonary disease
- muscle
- atrophy
- wasting
- cachexia
- inactivity
- p70S6K
- E3-ligases
- FoxO-1
- COPD mechanisms
- respiratory muscles
- systemic disease and lungs
Statistics from Altmetric.com
- Chronic obstructive pulmonary disease
- muscle
- atrophy
- wasting
- cachexia
- inactivity
- p70S6K
- E3-ligases
- FoxO-1
- COPD mechanisms
- respiratory muscles
- systemic disease and lungs
Introduction
Limb muscle dysfunction affects functional status,1 quality of life2 and survival in chronic obstructive pulmonary disease (COPD).3 Inspiratory muscle dysfunction is associated with negative clinical consequences such as dyspnoea, hypercapnic respiratory failure4 and even premature mortality.5 Among the different facets of skeletal muscle dysfunction, the regulation of muscle mass has attracted the attention of several research teams because of the clinical relevance of muscle wasting in COPD and other chronic diseases.
The maintenance of muscle mass may be compromised in a variety of clinical situations. Ageing, hypoxaemia, systemic inflammation (chronic or occurring during acute bursts in relation to COPD exacerbations),6 nutritional imbalance and oxidative stress may all threaten the preservation of muscle mass.7–9 Decreased muscle activation may also create an imbalance in the regulation of muscle mass that promotes catabolism10 11 at the expense of anabolism.12
These observations on the potential role of muscle activation as a cause of muscle dysfunction and wasting are relevant to COPD as chronic inactivity reduces the degree of quadriceps activation, even early in the disease process,13 while increased work of breathing results in a chronically activated diaphragm. Based on this divergent level of muscle activation between limb and respiratory muscles, one would predict that the pathways involved in the regulation of the quadriceps and diaphragmatic muscle mass should be regulated differentially in patients with COPD, with the former muscle expected to be more susceptible to catabolism and the latter exhibiting a tendency towards increased anabolism.
We recently explored atrophy/hypertrophy signalling pathways involved in the regulation of quadriceps muscle mass in wasted patients with COPD.14 As we predicted, this study showed an activation of the ubiquitin–proteasome pathway consistent with a catabolic state in the quadriceps of patients with COPD compared with controls with normal lung function.14 Similar findings have been reported by other investigators.15 Our investigation also revealed, in the same individuals, an overexpression of the muscle insulin-like growth factor-1 (IGF-1) hypertrophy signalling pathways that is not consistent with muscle atrophy and could represent a failed attempt to restore muscle mass.14
The regulation of diaphragmatic muscle mass is another active field of investigation. In apparent discrepancy with our hypothesis, an imbalance in the catabolic/anabolic status favouring catabolism has also been reported in patients with COPD.16–18 These findings were somewhat unexpected because the continuous training stimulus to which the COPD diaphragm is exposed should trigger anabolism.19–22
Activation of the ubiquitin–proteasome pathway in the quadriceps and the diaphragm does not mean that these two muscles are equally susceptible to catabolism. One difficulty in interpreting the current literature is that the comparative assessment of the quadriceps and diaphragm signalling pathways in COPD is based on comparisons of muscle samples that do not originate from the same subjects. This makes it impossible to rule out the potential role of confounders such as nutritional status, smoking status, exposure to corticosteroids and hypoxaemia that may influence the regulation of muscle mass. This concern can only be addressed by comparing the two muscle groups within the same individuals. Thus, using this approach, our aim was to measure and compare the mRNA and protein levels of the ubiquitin–proteasome and the IGF-1/Akt pathways in both muscle groups within the same individuals.
The present study was first designed to test the hypothesis that the ubiquitin–proteasome and the IGF-1/AKT pathways would be differentially regulated in the quadriceps muscle compared with the diaphragm in patients with COPD. Quadriceps and diaphragm biopsies obtained from the same patients showed a clear differential regulation of the biochemical pathways of interest in the vastus lateralis and the diaphragm in COPD.
These results naturally led to the question of whether this differential muscle mass regulation between the quadriceps and the diaphragm was specific to COPD or a normal phenomenon seen in healthy individuals. To address this, we recruited subjects with normal lung function from whom we obtained quadriceps and diaphragm biopsies. Our second hypothesis was that a differential regulation of the ubiquitin–proteasome and IGF-1/AKT pathways between the quadriceps and the diaphragm, if present, would be of a smaller magnitude in individuals with normal lung function than in those with COPD.
Methods
Subjects
Twelve patients with COPD undergoing lung resection were recruited. Nutritional status was evaluated with anthropometric parameters and serum albumin levels at the time of the investigation. Patients had not been exposed to systemic corticosteroids during the 2 months preceding their participation in the study and none were receiving long-term oxygen therapy. Seven subjects with normal lung function were also recruited in whom the same inclusion/exclusion used in COPD were applied except for lung function. None of the participating subjects was involved in our previous comparative study between the diaphragm and the quadriceps.22 Patients with body weight loss that could be ascribed to cancer were excluded. Further information on study subjects can be found in the online data supplement.
Pulmonary function tests and anthropometric measurements
Standard pulmonary function tests including spirometry, lung volumes with body plethysmography and transfer factor (diffusion capacity) were obtained according to previously described guidelines23 and related to the normal values of Quanjer et al.24 Height and weight were measured according to standardised methods.25
Muscle biopsies
Diaphragm
Diaphragm biopsies were obtained during a thoracic surgical procedure (thoracoscopy or thoracotomy).22 Either the right or the left diaphragm was biopsied, depending on the side of the surgery. Muscle samples were taken from the costal median region of the diaphragm (COPD: right side in 9/12; controls: right side in 4/7). Diaphragm specimens were frozen in liquid nitrogen and stored at −70°C for subsequent analysis.
Quadriceps
Needle biopsies of the quadriceps performed as routinely done in our laboratory26 were obtained within 24 h of the diaphragm biopsy. Muscle specimens were immediately frozen in liquid nitrogen and stored at −70°C for future analysis.
Skeletal muscle analysis
Muscle fibre cross-sectional area determination
The mean muscle fibre cross-sectional area (CSA) was determined for each muscle. Briefly, serial consecutive 5 μm cryosections were prepared from frozen muscle samples. The sections were immunohistochemically stained22 and all muscle sections were visualised by light microscopy and images digitally captured using Image Pro Plus 4.1 for Windows (MediaCybernetics, Silver Spring, Maryland, USA). The fibre CSA was calculated based on 80 randomly selected fibres for each muscle.27
RNA extraction and quantitative PCR
Total RNA extraction was performed from approximately 15 mg of muscle (TRIzol Reagent, Invitrogen, Carlsbad, California, USA); 1 μg of RNA was reverse transcripted to cDNA using Quantitect Reverse Transcription Kit (Qiagen Inc, Valencia, California, USA). Real-time PCR was performed in an Opticon 2 (MJ Research, Waltham, Massachusetts, USA) using Quantitect SYBR Green PCR Kit (Qiagen Inc). Further details on the PCR are provided in the online data supplement.
Protein extraction and western blotting
Cytoplasmic protein extraction was performed with approximately 30 mg of muscle using a commercial kit according to the manufacturer's protocol (NE-PER; Pierce Biotechnology, Rockford, Maryland, USA) for subsequent western blot analysis. The methodologies are described in further detail in the online data supplement.
Statistical analysis
The results are expressed as mean±SD unless otherwise specified. Between muscle group comparisons were performed using paired Student t tests or χ2 tests for gender distribution. Possible relationships between muscle mRNA and protein levels and pulmonary function were evaluated using Pearson correlations. To highlight the impact of COPD in the differential regulation of the ubiquitin–proteasome and IGF-1/AKT pathways in the two muscle groups, we compared the quadriceps to diaphragm ratio for the expression of the different mRNA and proteins of interest between subjects with COPD and those with normal lung function using unpaired t tests. The results were considered statistically significant if p values were <0.05.
Results
Subject characteristics
On average, patients with COPD had moderate to severe airflow obstruction (table 1). Six patients had stage II disease according to the GOLD classification28; the remaining had stage III disease. Body mass index and serum albumin levels were normal in all patients. Thirteen of the 19 study subjects were suspected of having a resectable lung cancer while one subject was diagnosed with carcinoma of the oesophagus. On final analysis, 11 had lung cancer and two patients had a benign tumour, and one patient had oesophageal lymphoma. This last patient was kept in the study since there was no extension of the lymphoma outside the thorax. One patient with normal lung function underwent surgery for recurrent pneumothoraces related to subapical blebs and four patients with COPD had a bullectomy. Patients with cancer did not differ in terms of their body mass index and clinical status from those with a benign condition. Mean quadriceps and diaphragm muscle fibre CSA were similar in both groups (5388±2043 μm2 and 4968±1504 μm2 for the quadriceps and diaphragm in patients with COPD; 4287±573 μm2 and 4319±1383 μm2 for the quadriceps and diaphragm in controls). There were no statistically significant between-group differences in quadriceps or diaphragm muscle fibre CSA.
Patient characteristics
Muscle atrophy and hypertrophy signalling in subjects with COPD
The mRNA expression of Atrogin-1, MuRF1 and FoxO-1 was significantly increased in the quadriceps compared with the diaphragm in patients with COPD (figure 1A–C). A significant positive correlation was observed between Atrogin-1 and MuRF1 mRNA expression in the quadriceps (r2=0.78, p<0.001) and in the diaphragm (r2=0.60, p=0.003). In the quadriceps, positive correlations were found between Atrogin-1 and FoxO-1 (r2=0.56, p=0.005) and between MuRF1 and FoxO-1 (r2=0.45, p=0.016) mRNA levels. Atrogin-1 protein expression was similar between the quadriceps and the diaphragm (data not shown).
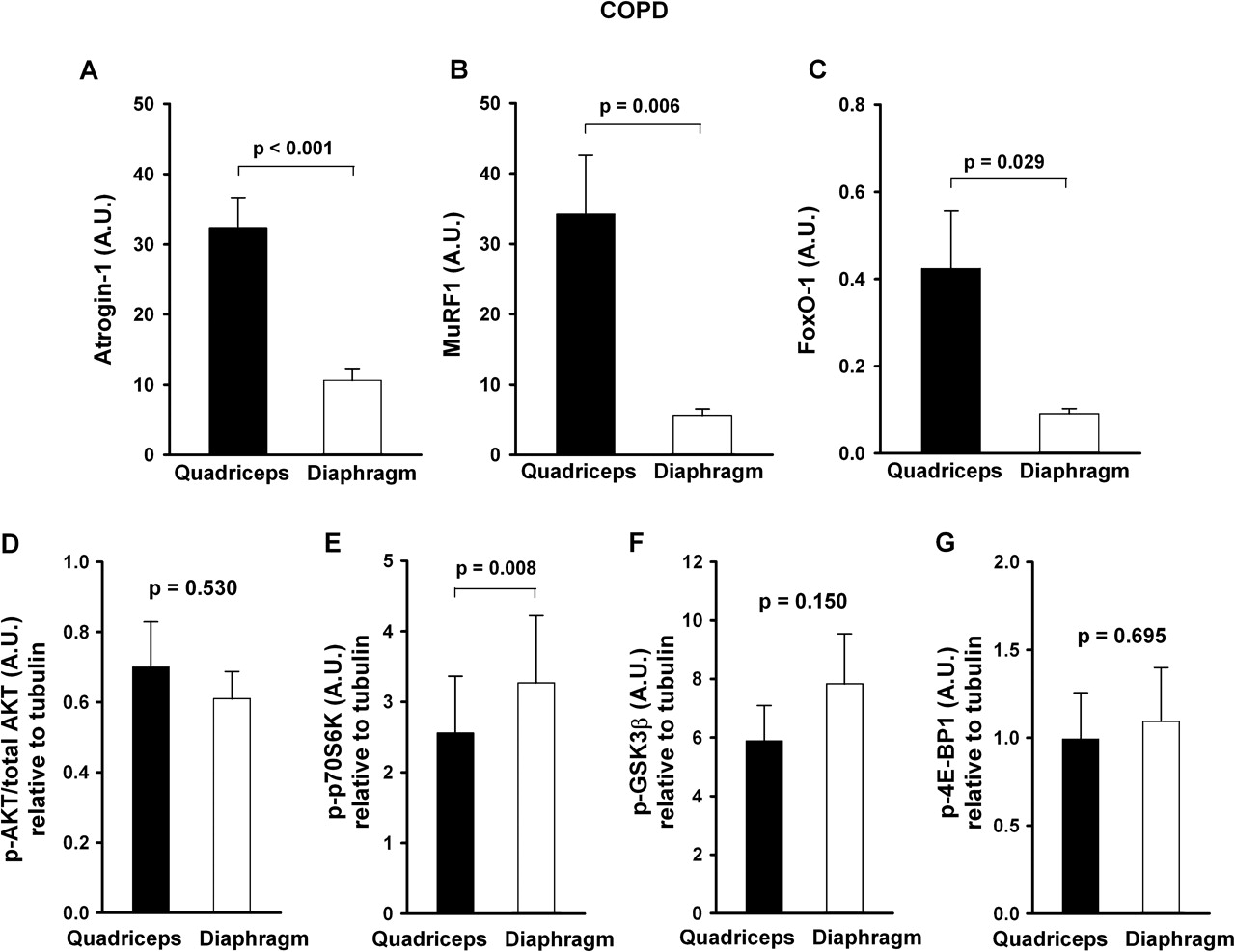
mRNA expression of (A) Atrogin-1, (B) MuRF1 and (C) FoxO-1 and protein content of (D) phosphorylated AKT/total AKT and the phosphorylated form of (E) p70S6K, (F) GSK3β and (G) 4E-BP1 in the quadriceps and diaphragm of patients with chronic obstructive pulmonary disease (COPD). Data are presented in arbitrary units (AU). Values are mean±SEM.
There were no significant differences in the protein levels of phosphorylated-AKT and the phosphorylated-AKT/total AKT ratio (figure 1D). p70S6K was significantly downregulated in its phosphorylated state in the quadriceps compared with the diaphragm in patients with COPD (figure 1E). There were no significant differences in phosphorylated-GSK3β and phosphorylated-4E-BP1 between the two muscles (figure 1F,G).
Muscle atrophy and hypertrophy signalling in subjects with normal lung function
In contrast to patients with COPD, the mRNA expression of Atrogin-1, MuRF1 and FoxO-1 was similar in the quadriceps and the diaphragm of controls (figure 2A–C). There were also no significant differences in the levels of phosphorylated-AKT and the phosphorylated-AKT/total AKT ratio or in phosphorylated-p70S6K, -GSK3β and -4E-BP1 between the two muscles in control subjects (figure 2D–G).
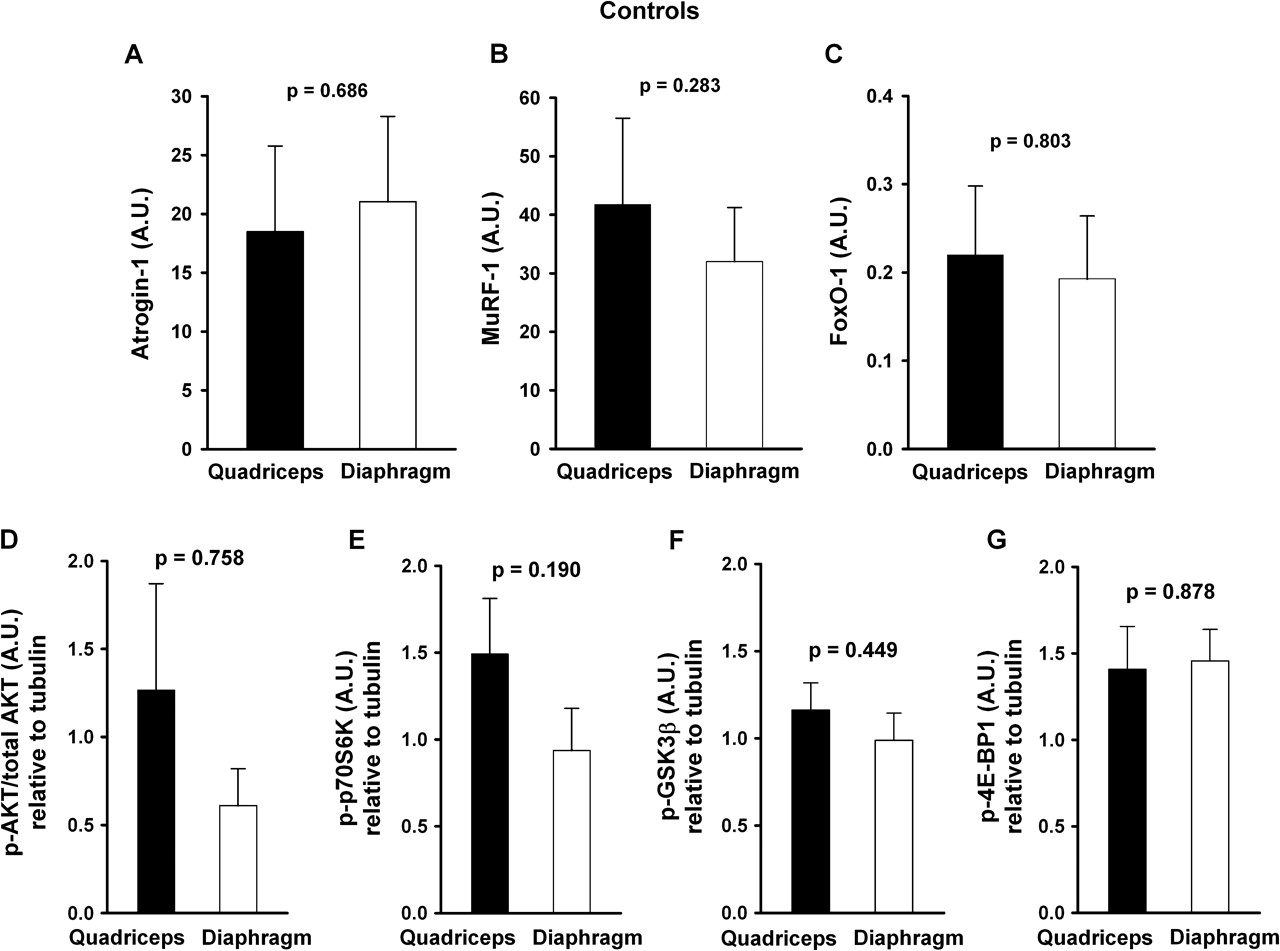
mRNA expression of (A) Atrogin-1, (B) MuRF1 and (C) FoxO-1 and protein content of (D) phosphorylated AKT/total AKT and the phosphorylated form of (E) p70S6K, (F) GSK3β and (G) 4E-BP1 in the quadriceps and diaphragm of subjects with normal lung function. Data are presented in arbitrary units (AU). Values are mean±SEM.
Quadriceps to diaphragm ratio of the ubiquitin–proteasome and IGF-1/AKT pathways
Muscle samples of the two study groups were analysed sequentially. For this reason and because material from patients with COPD was insufficient to repeat the experiments, it was not possible to make direct between-group comparisons of the regulation pathways of the quadriceps and the diaphragm. To further assess whether the differential expression of the ubiquitin–proteasome and IGF-1/AKT pathways was specific to COPD, we compared the quadriceps to diaphragm ratio of the different mRNA and proteins of interest between subjects with COPD and controls. The quadriceps to diaphragm ratio for Atrogin-1 and MuRF-1 mRNA was higher in subjects with COPD than in those with normal lung function, indicating a greater susceptibility to protein degradation in the quadriceps than in the diaphragm in subjects with COPD (figure 3A,B). Conversely, the quadriceps to diaphragm ratio for two proteins involved in hypertrophic signalling (p70S6K and GSK3β) was lower in subjects with COPD, indicating less hypertrophic stimulation in the quadriceps than in the diaphragm in COPD than in individuals with normal lung function (figure 3E,F).

Quadriceps to diaphragm ratio for (A) Atrogin-1, (B) MuRF1 and (C) FoxO-1 mRNA expression and protein content of (D) phosphorylated AKT/total AKT and the phosphorylated form of (E) p70S6K, (F) GSK3β and (G) 4E-BP1 in subjects with normal lung function and those with chronic obstructive pulmonary disease (COPD). Values are mean±SEM.
Relationships between diaphragm signalisation and pulmonary function
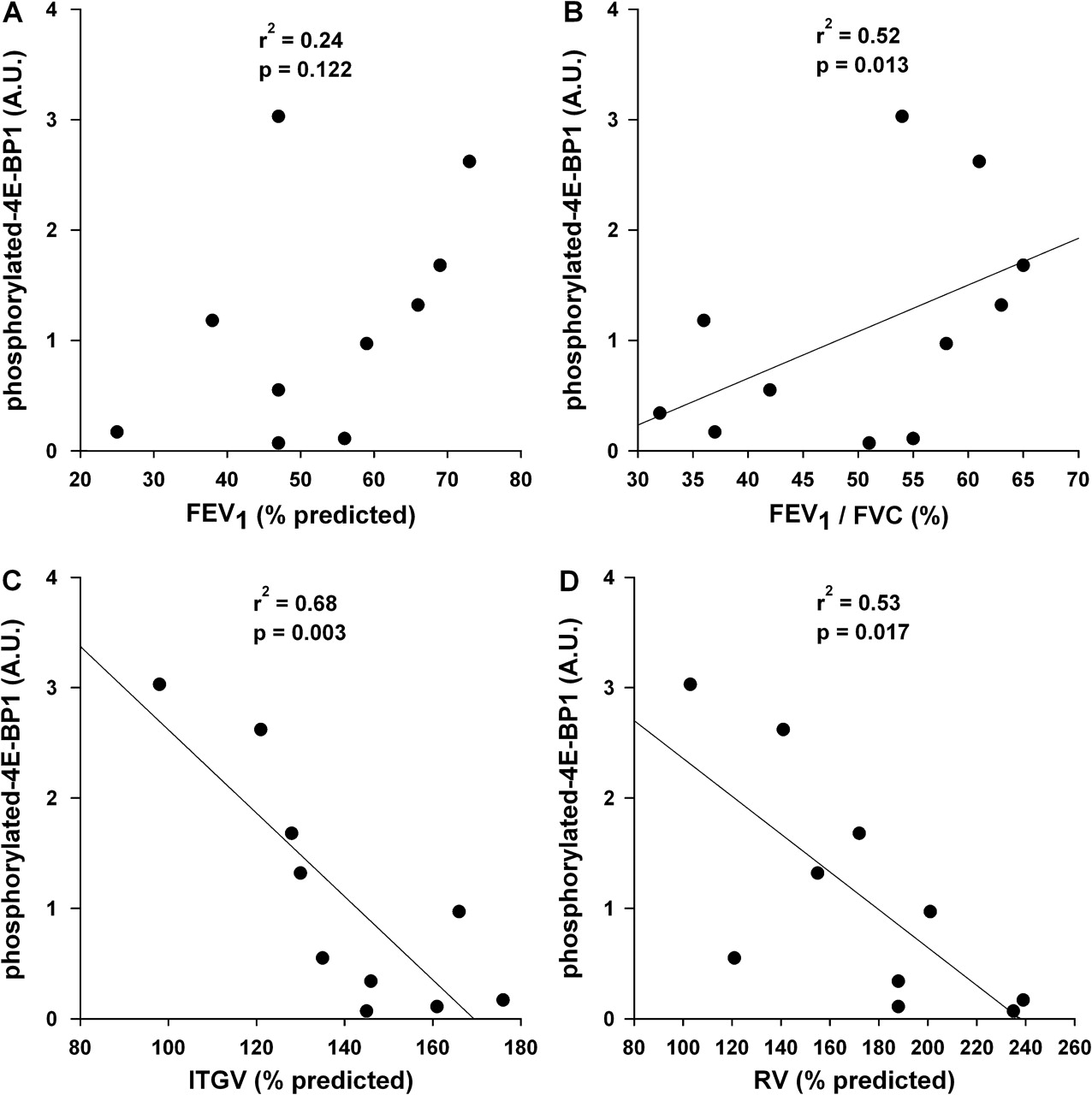
The phosphorylated-4E-BP1 diaphragm protein content did not correlate with forced expiratory volume in 1 s (FEV1) percentage predicted (figure 4A). As shown in figure 4B, there was a positive relationship between diaphragm phosphorylated-4E-BP1 protein content and FEV1/FVC ratio (FEV1/FVC%: r2=0.52, p=0.013). Phosphorylated-4E–BP1 protein content was inversely correlated with intrathoracic gas volume (ITGV), a surrogate of functional residual capacity, and residual volume (RV) (ITGV% predicted: r2=0.68, p=0.003; RV% predicted: r2=0.53, p=0.017; figure 4C,D). No other correlation with phosphorylated forms of AKT, p70S6K or GSK3β protein content was found with pulmonary function. There were no statistically significant correlations between the E3-ligases and indices of lung function.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation analyses between the phosphorylated form of 4E-BP1 protein content in the diaphragm and indices of pulmonary function. The phosphorylated 4E-BP1 protein content did not correlate with (A) forced expiratory volume in 1 s (FEV1) percentage predicted but was positively correlated with (B) the ratio of FEV1 to forced vital capacity (FEV1/FVC). Statistically significant inverse correlations were found between phosphorylated 4E-BP1 protein content and (C) intrathoracic gas volume (ITGV) percentage predicted and (D) residual volume (RV) percentage predicted. Protein contents are presented in arbitrary units (AU).
Discussion
This study provides a thorough investigation of key signalling pathways involved in the regulation of muscle mass in patients with COPD. A major feature of this study was the opportunity to investigate these pathways in two different muscles taken from the same individuals. Comparison with the diaphragm demonstrated greater catabolism and concomitant lower anabolism signalling in the quadriceps in patients with COPD. Although the study design did not allow a direct comparison of the regulating pathways of the two muscle groups between the two study groups, the data obtained in control subjects were useful in showing that this differential regulation of muscle mass between the quadriceps and the diaphragm was a specific feature of COPD, which suggests that this does not simply reflect a physiological situation but is part of the skeletal muscle adaptation seen in COPD.
The present results support an increased activation of the ubiquitin–proteasome pathway in the COPD quadriceps compared with the diaphragm, as indicated by the increased expression of Atrogin-1 and MuRF1 mRNA. Our data also suggest a role for FoxO-1 in the transcriptional upregulation of these two muscle-specific E3-ligases. In spite of similar AKT protein content, a decrease in the levels of the active form of p70S6K was also found in the COPD quadriceps and could be interpreted as a suboptimal anabolic signal in this muscle. Together these results suggest that the balance between atrophy and hypertrophy signalling is not homogeneous between respiratory and lower limb muscles, the latter muscles being more susceptible to catabolism. An important finding was that this imbalance towards greater susceptibility to catabolism in the quadriceps was not seen in individuals with normal lung function, suggesting that the observations made in subjects with COPD were driven by the underlying pathological process. Although the mechanistic explanation underlying the differential regulation in muscle mass between the COPD quadriceps and diaphragm could not be explored, one likely candidate is a larger difference in activity levels between these two muscles in subjects with COPD than in individuals with normal lung function.
Although the level of muscle activation was not measured in this study, physical inactivity is a common feature of COPD which is already present early in the disease process.13 29 Conversely, the diaphragm in COPD faces a chronic increase in work load that acts as a continuous source of muscle stimulation.30 Mechanical unloading in human models initiates muscle protein breakdown that is mediated via activation of the proteasome components.10 11 31 Also, the extent of muscle atrophy and upregulation of the ubiquitin–proteasome system within a given muscle is tightly related to the magnitude of the reduction in muscle activation.32 These results are consistent with the notion that the low level of activity of the quadriceps could favour the signalling of muscle protein breakdown in patients with COPD.
Other interesting findings that support the involvement of local factors in the regulation of muscle mass in COPD are the negative correlations between phosphorylated-4E-BP1 protein content and lung hyperinflation indices. These results suggest that decreased protein synthesis might be triggered by chronic diaphragm shortening.33 These muscle adaptations in COPD may promote the loss of contractile proteins, perhaps related to the loss and/or shortening of diaphragm sarcomeres which occurs as part of the adaptation to chronic hyperinflation.30 Increased activation of the ubiquitin–proteasome pathway has been reported in the diaphragm of patients with COPD,17 18 while increased apoptosis and altered regeneration capacity of the diaphragm has been found in emphysematous hamsters.34 These data are thus consistent with the notion that COPD may predispose to the loss of diaphragmatic muscle mass although, as suggested by our results, to a lesser extent than the quadriceps.
A possible contribution of systemic factors in the expression of the anabolic/catabolic regulation pathways in the quadriceps and the diaphragm cannot be excluded because these two muscles may react differently to the presence of systemic factors such as inflammatory mediators, corticosteroids and hypoxaemia in their external milieu. Although less likely, the possibility also exists that intrinsic alterations of the quadriceps muscle tissue itself may render it more susceptible to catabolism than the diaphragm.
We found a parallel upregulation in Atrogin-1 and MuRF1 in the quadriceps and the diaphragm in patients with COPD. Although a coordinate expression of these two E3-ligases is often seen in models of atrophy,35 this is not always the case. Atrogin-1 but not MurF1 has been reported to be upregulated in the COPD diaphragm.17 18 In one study,18 60% of the COPD study population was exposed to systemic corticosteroids. This is relevant when considering that Atrogin-1 might be more responsive to corticosteroids than MuRF1.36 Thus, discrepancies in the expression pattern of the E3-ligases between studies could be explained by differences in study population and in the specific models of atrophy under study.
In the present study, an upregulation of FoxO-1 mRNA was found in the quadriceps compared with the diaphragm of patients with COPD. Moreover, the positive associations of FoxO-1 with both E3-ligases support a transcriptional role for FoxO-1 in the regulation of the ubiquitin–proteasome pathway in the quadriceps. In addition to being a negative regulator of muscle mass, FoxO-1 also appears to downregulate several type I fibre-related genes as demonstrated in transgenic mice with muscle-specific overexpression of FoxO-1.37 We therefore speculate that FoxO-1 may be involved in the regulation of limb muscle mass and fibre-type expression in patients with COPD.33
Potential implications of the findings
Although there was clear differential expression of the atrophy and hypertrophy signalling pathways of the quadriceps and diaphragm in subjects with COPD favouring atrophy in the quadriceps, we could not demonstrate quadriceps muscle fibre atrophy in comparison to the diaphragm in these individuals. The cross-sectional nature of the current study should be appreciated so that it is not possible to make inference about a possible ongoing atrophy process in the quadriceps. Interestingly, perturbations in the biochemical pathways regulating muscle mass precede overt muscle fibre atrophy and weight loss in experimental38 and human models of cachexia.39 Our results suggest a similar phenomenon in patients with COPD. Only longitudinal studies with serial muscle biopsies and muscle mass measurements could confirm that biochemical events within the muscles antedate muscle atrophy. One potential implication of this discussion is that consideration should be given to early targeting of the biochemical changes responsible for the atrophying process.
Limitations of the study
A number of methodological considerations and potential limitations need to be taken into account when interpreting our study. First, the study was not designed to compare directly the ubiqutin–proteasome and AkT/IGF-1 pathways of the quadriceps and the diaphragm in subjects with COPD versus healthy controls. Second, there was a tendency towards an imbalance in sex distribution between the two study groups, although this did not reach statistical significance. However, any influence of hormonal status on the results has been minimised because all studied women were postmenopausal. Third, human diaphragm samples can only be obtained in patients scheduled to undergo a surgical procedure. The presence of a lung neoplasm in half of the patients could have, through cancer-related cachexia, influenced muscle molecular signalling. Any potential confounding effects of any systemic effects related to cancer should have been minimised by the fact that the diaphragm and quadriceps were exposed to the same external milieu. Also, patients with body weight loss that could be ascribed to cancer were excluded. Fourth, information on body composition and whether patients with COPD were involved in a progressive body weight loss process are not available owing to the limited access to these patients prior to surgery. This limitation is partially compensated by the measurements in muscle fibre CSA, a parameter that is related to muscle mass.40 Last, the ubiquitin–proteasome activity was evaluated only indirectly and mRNA levels alone were measured for FoxO-1 and MuRF1.
Conclusion
This study highlights potentially key molecular mechanisms involved in muscle atrophy in patients with COPD by the comparison of two muscles with different levels of activity. Evidence of an increase in atrophic signals in the quadriceps compared with the diaphragm in patients with COPD was demonstrated by the upregulation of mRNA expression of Atrogin-1 and MuRF1. This gene upregulation was likely to be mediated by the expression of FoxO-1. On the other hand, decreased expression of p-p70S6K in the quadriceps would indicate a low anabolic signal in this muscle. Low anabolic signals combined with increased activation of the catabolic pathway would represent an unfavourable situation for the quadriceps, potentially leading to atrophy. Together, these results suggest that the balance between atrophy and hypertrophy signalling is not homogeneous between respiratory and lower limb muscles and that local factors are involved in the regulation of muscle mass in patients with COPD.
Acknowledgments
The authors acknowledge the contribution of Audrey Lapierre for his technical assistance, Serge Simard for his statistical assistance and Marthe Bélanger, Christine Racine, Sabrina Biardel and France Simard for their help in accomplishing this study.
References
Supplementary materials
Web Only Data THORAX.2009.133827
Files in this Data Supplement:
Footnotes
Funding Canadien Institutes of Health Research grant MOP-84091. FM holds a GSK/CIHR Research Chair on COPD at Université Laval.
Competing interests None.
Ethics approval This study was conducted with the approval of the Comité d'Éthique de la Recherche, Institut Universitaire de Cardiologie et de Pneumologie de Québec and each patient signed a written informed consent form.
Provenance and peer review Not commissioned; externally peer reviewed.