Article Text

Abstract
Background Comorbidities associated with systemic inflammation including cardiovascular disease (CVD), stroke and diabetes mellitus (DM) are common among individuals with chronic obstructive pulmonary disease (COPD). A study was undertaken to quantify the burden of comorbidity and to determine the risk of first acute arteriovascular events among individuals with COPD.
Methods The computerised primary care records of 1 204 100 members of the general population aged ≥35 years on 25 February 2005 were searched for recordings of each disease. Data were analysed using multivariate logistic regression. Cox regression was used to determine whether individuals with COPD were at increased risk of acute myocardial infarction (MI) and stroke.
Results Cross-sectional analyses showed that physician-diagnosed COPD was associated with increased risks of CVD (OR 4.98, 95% CI 4.85 to 5.81; p<0.001), stroke (OR 3.34, 95% CI 3.21 to 3.48; p<0.001) and DM (OR 2.04, 95% CI 1.97 to 2.12; p<0.001). In the follow-up analyses, after adjusting for confounding by sex and smoking status and stratifying for age, the greatest increase in the rate of acute arteriovascular events was found in the youngest age groups; the HR for acute MI was 10.34 (95% CI 3.28 to 32.60; p<0.001) and for stroke the HR was 3.44 (95% CI 0.85 to 13.84; p<0.001) compared with the oldest age group.
Conclusion Individuals with COPD are substantially more likely to have pre-existing CVD, DM or a previous stroke and are at high risk of acute arteriovascular events. National COPD guidelines and models of care need to adapt to provide an integrated approach to addressing these comorbidities.
- Chronic obstructive pulmonary disease
- comorbidity
- cardiovascular disease
- diabetes mellitus
- stroke
- COPD epidemiology
Statistics from Altmetric.com
- Chronic obstructive pulmonary disease
- comorbidity
- cardiovascular disease
- diabetes mellitus
- stroke
- COPD epidemiology
Introduction
Chronic obstructive pulmonary disease (COPD) causes 5% of deaths in the UK1 and may contribute to more. Cardiovascular disease (CVD) and cerebrovascular disease are the leading causes of morbidity and mortality in high-income countries, together accounting for 27% of all deaths; diabetes mellitus (DM), an important risk factor for both these diseases, independently accounts for at least 2.6% of deaths in these countries.2 People with COPD are at high risk of hospitalisation and death from CVD3 4 and cerebrovascular disease5 6 and at increased risk of DM.7 Despite this, there is a paucity of data to quantify the degree to which these diseases coexist in COPD.
We therefore used UK-wide primary care data to quantify the association between COPD and diagnoses of cardiovascular disease, stroke and DM, and to determine whether individuals with COPD are at increased risk of a subsequent first cardio-cerebrovascular event compared with those without COPD. These associations were examined further for evidence of variation according to age, sex, smoking history, socioeconomic status and region of residence.
Methods
Dataset
The Health Improvement Network (THIN) is a large database of anonymised computerised primary care medical records collected at 311 general practices throughout the UK and has been shown to have high standards of validity.8
Study population
All patients alive and contributing to THIN on 25 February 2005 were included in the study. These patients were originally identified as part of a larger study of current care for patients with COPD 1 year after the introduction of the General Medical Services contract in February 2004; the results are published elsewhere.9 For this analysis, patients were defined as having COPD if they were aged >35 years and had a relevant diagnosis recorded prior to the baseline date.10 Where possible, in those with COPD the percentage predicted forced expiratory volume in 1 s (FEV1) was calculated using standard reference tables11 and patients were grouped according to disease severity using British Thoracic Society (BTS) guidelines.10 Details of sex, age, smoking status, region of residence and postcode level sociodemographic indicators were also extracted.
Definition of outcomes
All patient records were searched to identify diagnoses of CVD, stroke and DM. Our definition of CVD included diagnoses of angina, myocardial infarction (MI), heart failure, peripheral vascular disease and aortic aneurysm, and having undergone a previous angioplasty procedure. Cardiac arrhythmias and valvular heart disease were excluded because of their wide range of potential aetiologies; right-sided heart disease was excluded as it frequently results from primary pulmonary pathology. Our definition of stroke included diagnoses of subarachnoid and intracranial haemorrhage and transient ischaemic attack. To increase the sensitivity of our case definition for DM, we included all patients who had received prescriptions for oral hypoglycaemic agents or insulin.
Analysis strategy
Two analyses were carried out, a cross-sectional analysis to establish the prevalence of comorbid disease among patients with and without COPD and a survival analysis to determine whether individuals with COPD are at increased risk of subsequent first acute MI or stroke. The baseline date for both analyses was 25 February 2005.
Cross-sectional analysis
Our primary outcome was the relation between prevalent COPD and a diagnosis of each of CVD, stroke or DM on or prior to the baseline date. Logistic regression models were used to estimate the relevant ORs. Separate multivariable models were built for each disease to look for confounding or effect modification by age, sex, smoking status, quintile of postcode level Townsend index of deprivation,12 region of residence (grouped by Strategic Health Authority13) and each of the other comorbidities of interest. Factors which changed the summary OR for the main comorbidity of interest by at least 10% were retained. Likelihood ratio testing (with threshold p=0.05) was used to determine whether models incorporating interaction terms provided a better fit. Where evidence of effect modification was found, ORs were calculated separately for each level of that factor.
Survival analysis
Crude rates of stroke and acute MI were calculated for patients with and without COPD. Cox proportional hazards models were used to produce adjusted HR estimates to determine whether individuals with COPD have a greater risk of subsequent MI or stroke than those without. Any new record subsequent to the baseline date was noted to indicate an incident event. Patients with a previous diagnosis of stroke or CVD prior to the baseline date were excluded from the stroke and acute MI analyses respectively as the risk of a second event is likely to differ from that of the first. End of follow-up was defined as the last date of data collection at the patient's practice or date of death or transfer to another practice. Increase in all-cause mortality in those with COPD has been determined previously using this dataset and was therefore not repeated.9 Likelihood ratio testing was used to determine whether there was evidence of effect modification, and a change of 10% or more in the HR estimate was deemed to indicate confounding. Consistency with the proportional hazards assumption was assessed using tests based on scaled Schoenfeld residuals.14 All analyses were carried out using Stata 10 SE (Stata Corp, Texas, USA).
Sensitivity analyses
Several sensitivity analyses were performed to explore the possible effects of misclassification of smoking status (see online data supplement). In brief, we repeated our analyses recategorising ex-smokers as current smokers and those with unknown smoking status as never smokers and as current smokers. We also performed the analyses excluding those with COPD but without a record for FEV1. Finally, we repeated the survival analysis for both outcomes excluding patients with previous diagnoses of either stroke or CVD for comparison.
Results
Study population
A total of 1 204 110 active patients aged >35 years on 25 February 2005 were identified, 2.5% of whom had COPD. More patients resided in areas of least deprivation (22.5%) than in the most deprived areas (9.2%). In addition, the south-east region of the UK was over-represented, contributing 17.6% of patients compared with the north-east, for example, which contributed around 3%. Eighty-six percent of patients with a diagnosis of COPD were current or ex-smokers. Spirometry data were available for 61.9% of patients, the majority of whom had mild (37.5%) or moderate (19.1%) disease (table 1).
Demographic characteristics of study population by diagnosis of COPD
Cross-sectional analysis
In the univariable analysis, COPD was associated with a fivefold increase in the odds of having had CVD (OR 4.98, 95% CI 4.85 to 5.81; p<0.001), a threefold increase in the odds of having had a stroke (OR 3.34, 95% CI 3.21 to 3.48; p <0.001) and twofold increase in the odds of having DM (OR 2.04, 95% CI 1.97 to 2.12; p<0.001) compared with those without COPD. In the multivariable analysis there was evidence of effect modification by smoking history and age group (table 2).
Crude and adjusted† ORs from multivariable analysis of having COPD and a previous diagnoses of CVD, stroke or DM in different strata of smoking status and age in years
Cardiovascular disease
The association between diagnoses of COPD and CVD was strongest in the younger age groups, with never smokers with COPD having a 7.7-fold increased prevalence of CVD compared with those without COPD. This association persisted across all ages but reduced as age increased and, in almost all age groups, was stronger among never-smokers than among ex-smokers or current smokers of the same age (table 2).
Stroke
The increase in odds of having had a stroke among individuals with COPD was generally lower than that for CVD for all age groups and was less consistently associated with smoking status. The effects were greatest in the youngest current smokers (OR 5.1, 95% CI 2.6 to 9.9) and this association reduced in magnitude with advancing age (table 2).
Diabetes mellitus
COPD was associated with a small increase in the odds of DM in the younger age groups and was generally slightly higher in never smokers. The greatest effect was seen in the youngest current smokers (OR 2.4, 95% CI 1.6 to 3.6) and 45–55-year-old never smokers (OR 2.4, 95% CI 1.5 to 4.0). In older age groups, COPD was associated with a reduction in DM regardless of smoking status (OR 0.7, 95% CI 0.7 to 0.8 for current smokers; table 2).
Survival analysis
The median duration of follow-up was 895 days (IQR 893–895), during which time 2699 first acute MIs and 9691 first strokes were recorded. The last day of the follow-up period for both outcomes was 20 August 2007. All models were found to be consistent with the proportional hazards assumption.
Acute myocardial infarction
Crude rates of MI were higher in women and in ex-smokers and current smokers and increased with advancing age and increasing deprivation (table 3). There was evidence of effect modification by age and confounding by smoking; sex was included as an a priori confounder. Region, Townsend score and diagnoses of stroke and DM had minimal impact on the final model and were excluded. In the crude analysis, COPD was associated with a 3.5-fold increase in the rate of acute MI (95% CI 3.02 to 4.13; p<0.001). In the adjusted analysis, HRs were greatest among those in the youngest age group (HR 10.34, 95% CI 3.28 to 32.60; p<0.001) and lowest in those aged >75 years (HR 1.34, 95% CI 1.03 to 1.73; p<0.001; table 4). Cumulative incidence plots are shown in figure 1.
Crude rates of acute myocardial infarction (MI) and stroke by diagnosis of chronic obstructive pulmonary disease (COPD) and demographic characteristics
Increase in rate of developing acute myocardial infarction (MI) and stroke in those with chronic obstructive pulmonary disease compared with those without in strata of age in years and adjusted for sex and smoking status
Cumulative incidence of first time acute myocardial infarction in people with and without chronic obstructive pulmonary disease (COPD) during the follow-up period.
Stroke
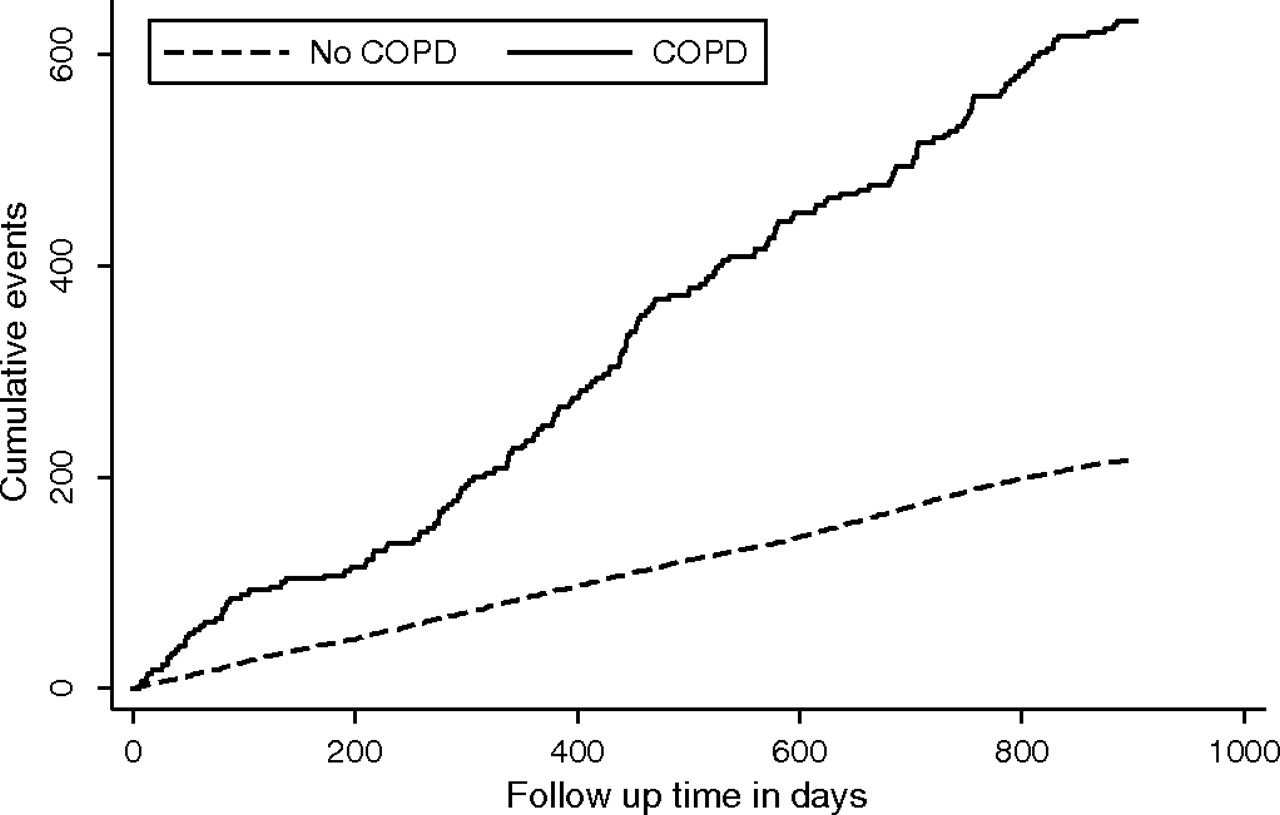
Crude rates of stroke were higher in men and ever smokers and increased with age and quintiles of deprivation (table 3). The multivariable analysis identified age and smoking as confounders and sex was again included as an a priori confounder. Region, Townsend score and diagnoses of CVD and DM had no impact on the final model and were excluded. In the crude analysis, COPD was associated with a 2.8-fold increase in the rate of acute stroke (95% CI 2.56 to 3.04, p<0.001). The adjusted model again found the highest HR in the youngest age group (HR 3.44, 95% CI 0.85 to 13.84; p<0.001) and a clear gradual reduction with advancing age, with the oldest age group having a HR of 1.10 (95% CI 0.98 to 1.23; p<0.001; table 4). Cumulative incidence plots are shown in figure 2.

{kind=link}
{kind=link}
Cumulative incidence of first time stroke in people with and without chronic obstructive pulmonary disease (COPD) during the follow-up period.
Sensitivity analyses
In the cross-sectional analysis, recategorising those with unknown smoking status as never smokers resulted in a small increase in the adjusted OR for CVD and DM and a greater increase in the OR for stroke (adjusted OR 8.2 for stroke in never smokers aged 35–44 years, 95% CI 2.0 to 33.4). These effects were greatest in younger patients, and for all three outcomes the OR was greatest in never smokers compared with current smokers. No change was seen in the results for the survival analyses with this grouping. When patients with unknown smoking status were recategorised as current smokers, there was again an increase in adjusted OR for all outcomes and across all age groups with the greatest increase seen for stroke and in younger patients. As in the original analysis, the OR for CVD and DM was greater in never smokers whereas, for stroke, the trend changed from showing no real relation with smoking status to being greater in current smokers (adjusted OR 7.4 for stroke in current smokers aged 35–44 years, 95% CI 3.9 to 13.9). In the survival analysis the adjusted HRs were slightly higher for both acute MI and stroke across all ages, with the greatest effects in the younger patients. Recategorising patients who were ex-smokers as current smokers made no difference to the results of the cross-sectional or survival analyses for any of the outcomes. When we repeated the analyses excluding patients with COPD who did not have a record for FEV1, there was no clinically important change to the results. Finally, results from the survival analysis were similar when excluding either patients with a previous diagnosis of stroke or previous diagnoses of both stroke and CVD at baseline (see online data supplement).
Discussion
As expected, our cross-sectional analysis identified a strong association between having COPD and a past diagnosis of CVD, with the strongest effect seen in the youngest patients. A similar but weaker association was found between COPD and having had a stroke. COPD was associated with increased odds of DM in younger patients but a decrease in odds in older age groups. We also found strong evidence of an increased risk of subsequent stroke (more than threefold) and acute MI (more than tenfold) in patients with COPD compared with those without, again with the greatest effect in younger patients.
Our results should be representative of the UK population as it includes patients from all UK regions.9 The overall percentage of missing data was small and our results were consistent when we repeated the analyses excluding these patients. Although participating GP practices in THIN are self-selecting, this is unlikely to result in inaccurate reporting of the diseases of interest. There is a slight over-representation of younger more affluent patients in THIN, but our observed prevalence of COPD is comparable with national data.15
Use of routine medical records should eliminate differential misclassification due to recall or interviewer bias. The prevalence of stroke in our dataset was relatively low compared with national data,16 which may be due to some affected individuals not requiring ongoing monitoring or medication and therefore being less likely to have a diagnosis in their records. In contrast, CVD and DM usually require regular monitoring and symptom control in primary care and are thus more likely to be recorded; additionally, we used prescription records to increase the sensitivity of our definition for DM. It was not possible to check the validity of diagnoses for COPD, although availability of spirometry results for many patients partly mitigates this and our prevalence of COPD was comparable to national data. We were unable to adjust for ethnicity as these data are not included in THIN.
We did not use the lung function data for our analyses because, contrary to current guidelines,10 38% of patients with COPD had no spirometry records. These tended to be older patients (45% were aged >75 years) and are likely to be those with more severe disease. No clinically important difference was seen in the results after excluding patients with COPD but without spirometry records from the analysis, suggesting misclassification of COPD in our dataset was not a significant problem.
The main limitation of our study is the potential for differential misclassification of smoking status: patients with COPD or CVD are more likely to be questioned about smoking than healthy individuals or infrequent primary care attendees. While previous studies suggest that GP records may be an unreliable indicator of smoking status,17 the proportion of smokers in our population is similar to national data18 and the proportion of patients without a record of smoking status was acceptable. Importantly, the sensitivity analyses that we performed to explore the possible effects of misclassification of smoking status found little impact on the overall results, which suggests this was not a major problem in our dataset (see online data supplement).
COPD and CV disease
To our knowledge, no large studies have investigated the difference in prevalence of CVD between patients with and without diagnoses of COPD or performed stratified analyses by age or smoking. It is well recognised that people with COPD4 or smokers with impaired lung function19 have high cardiovascular-related mortality; some suggest this is especially common in people with mild to moderate COPD compared with those with severe disease where the primary cause of death is usually respiratory disease.20 Furthermore, in people without COPD and with almost normal lung function, percentage predicted FEV1 has been shown to be inversely associated with CVD. In a study of >15 000 patients followed for 15 years, the Relative Risk (RR) of cardiovascular-related mortality was 1.56 (95% CI 1.26 to 1.92) comparing lowest with highest quintiles of FEV1 (range 73–113%).21 Other studies have found similar results using percentage predicted FEV1 and less specific markers of lung function.22 23 Conversely, the Whitehall study found an association between possible symptoms of COPD (chronic phlegm production) and increased cardiovascular-related mortality, but this disappeared after correcting for percentage predicted FEV1.24
COPD and stroke
No studies were identified describing the risk of stroke in people with either COPD or low percentage predicted FEV1. However, several cohort studies have used absolute values for FEV1, the majority finding an inverse association between FEV1 and incidence of stroke or mortality due to stroke.21 25–27 The Whitehall study of 18 403 men aged 40–64 years found that those with an FEV1 <3.0 litres, independent of other risk factors, were almost twice as likely to die from a stroke as those with an FEV1 >3.5 litres.26 However, other studies have observed this only in subgroups of the population25 27 or have detected no association.28
COPD and diabetes mellitus
Rana et al reported a prospective cohort study of >100 000 patients which found an adjusted RR of 1.8 (95% CI 1.1 to 2.8) for DM in those with COPD compared with those with asthma.7 Other cohort studies have not looked specifically at COPD but have identified a consistent inverse relation between forced vital capacity and the risk of developing DM and reported similar results with FEV1.29
This study provides robust evidence that patients with COPD are at significantly higher risk than the general population of having CVD, cerebrovascular disease and (to a lesser extent) DM, and therefore at a much higher risk of premature mortality. While the highest relative risks are for individuals in the youngest age group, the highest absolute burden of comorbid disease lies in the older age group which constitutes 39% of the population with COPD, despite the comparatively low relative risks of this group (probably a consequence of healthy survivor bias). In addition, COPD is underdiagnosed in primary care,30 so the true difference in risks between those with and without COPD may be even greater.
Overall, the extent to which COPD, CVD, stroke and DM are interrelated is striking; almost 40% of all individuals with COPD have an existing diagnosis of at least one of these other diseases and are at substantially increased risk of experiencing future acute arteriovascular events. While one obvious explanation for these observations is shared risk factors such as smoking, poor diet and low socioeconomic class, there is good evidence that, even after adjusting for these and other confounders such as age, an independent relation still exists.31 It is increasingly recognised that these diseases are all characterised by chronic systemic inflammation7 32 and that the coexistence of these conditions in individuals may be because they represent different facets of a single syndrome.33 The observation that the greatest effect of COPD on having CVD appears to be in patients without a history of smoking is intriguing. For DM and, to a lesser extent, stroke, the effect is greater in current smokers for the youngest patients and, after the age of 45 years, becomes greater in never smokers. Our sensitivity analyses confirm that this relation with smoking is likely to be real and may result from complex interactions with smoking and the different impact of chronic inflammation on development of these conditions at different ages.
These data provide further evidence that, to improve patient care, health service models for people with COPD and national guidelines10 need to recognise the extent to which these conditions are co-incident. It also provides additional evidence that, at the time of diagnosis of COPD, healthcare professionals must be proactive and, where appropriate, must seek to promote early diagnosis and treatment and aggressively target risk factors in order to reduce the risk of premature mortality.34
References
Supplementary materials
Web Only Data thx.2009.128082
Files in this Data Supplement:
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics committees of the University of Nottingham and London School of Hygiene and Tropical Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves