Article Text

Abstract
Background Tuberculous pleuritis remains the commonest cause of exudative effusions in areas with a high prevalence of tuberculosis and histological and/or microbiological confirmation on pleural tissue is the gold standard for its diagnosis. Uncertainty remains regarding the choice of closed pleural biopsy needles.
Objectives This prospective study compared ultrasound-assisted Abrams and Tru-Cut needle biopsies with regard to their diagnostic yield for pleural tuberculosis.
Methods 89 patients (54 men) of mean±SD age 38.7±16.7 years with pleural effusions and a clinical suspicion of tuberculosis were enrolled in the study. Transthoracic ultrasound was performed on all patients, who were then randomly assigned to undergo ≥4 Abrams needle biopsies followed by ≥4 Tru-Cut needle biopsies or vice versa. Medical thoracoscopy was performed on cases with non-diagnostic closed biopsies. Histological and/or microbiological proof of tuberculosis on any pleural specimen was considered the gold standard for pleural tuberculosis.
Results Pleural tuberculosis was diagnosed in 66 patients, alternative diagnoses were established in 20 patients and 3 remained undiagnosed. Pleural biopsy specimens obtained with Abrams needles contained pleural tissue in 81 patients (91.0%) and were diagnostic for tuberculosis in 54 patients (sensitivity 81.8%), whereas Tru-Cut needle biopsy specimens only contained pleural tissue in 70 patients (78.7%, p=0.015) and were diagnostic in 43 patients (sensitivity 65.2%, p=0.022).
Conclusions Ultrasound-assisted pleural biopsies performed with an Abrams needle are more likely to contain pleura and have a significantly higher diagnostic sensitivity for pleural tuberculosis.
- Tuberculosis
- pleural effusions
- ultrasound
- Abrams
- Tru-cut
Statistics from Altmetric.com
Introduction
Approximately one-third of the world's population is infected with Mycobacterium tuberculosis1 and, among communicable diseases, tuberculosis (TB) is the second leading cause of death.2 Pleural TB remains a common form of extrapulmonary TB, particularly among HIV-positive individuals,3 4 and it is the most common cause of exudative effusions in areas with a high prevalence of TB.2 5 6
Although a presumptive diagnosis of pleural TB is often based on raised levels of adenosine deaminase (ADA) and interferon γ in pleural fluid, actual histological and/or microbiological confirmation of TB pleuritis remains the gold standard.5 6 Pleural tissue can be harvested either by means of closed biopsies, thoracoscopy or open surgical biopsies.5 6 Access to thoracoscopy and open surgical biopsies is limited in many parts of the world and closed biopsies are therefore the preferred initial investigation.6
Closed pleural biopsy needles were introduced in the mid-1950s and early 1960s and various types were used, including the Abrams, Cope and Vim-Silverman needles.7–11 Of these devices, the Abrams needle was consistently shown to have a high yield and became the most widely used device.11–13 In 1989 Macleod et al described blind cutting needle (Tru-Cut) biopsies as an alternative to Abrams needles in patients who present with large pleural effusions.14 Around the same time, transthoracic ultrasound (US)-assisted biopsy techniques were pioneered, and the indications were soon expanded to include cutting needle pleural biopsies.15–18 Focal pleural abnormalities (eg, thickening) and fluid collections could be identified by means of US, and biopsy may be aimed at these areas of interest.19 Moreover, estimating the size of an associated effusion decreases the risk of visceral pleural lacerations, which is particularly relevant in cases with minimal pleural effusion and where pointed cutting needle biopsy devices are employed.19
One small prospective study found a superior diagnostic yield for pleural TB with US-assisted Tru-Cut compared with traditional Abrams needle biopsies.17 In that study, which was performed in an area with a moderate TB prevalence, only two of 10 Abrams needle biopsies were diagnostic for pleural TB. As most authors have reported diagnostic sensitivities in the order of 50–85% for Abrams needle biopsies,6 13 uncertainty remains as to which of these closed pleural biopsy techniques is superior for pleural TB.
The aim of this prospective study was to compare US-assisted Abrams needle biopsies with US-assisted Tru-Cut needle biopsies with regard to their diagnostic yield for pleural TB.
Methods
Study population
All adult patients (≥18 years) referred to the Division of Pulmonology of Tygerberg Academic Hospital with radiological evidence of a pleural effusion and clinical suspicion of pleural TB were potential candidates for this study. Our institution is a 1200-bed academic hospital in Cape Town, South Africa. It is one of two academic referral centres in the city and renders a tertiary service to a population of approximately 1.5 million. In 2006 the incidence of pulmonary TB in this population was 940 cases per 100 000.1
Patients referred to the division's pleural theatre were screened for indicators of a high clinical suspicion of TB which, for the purposes of the study, included (1) known HIV infection, (2) persistent cough lasting >3 weeks, (3) haemoptysis, (4) weight loss >4 kg (5) intermittent fever >3 weeks and (6) drenching night sweats >2 weeks. Patients were included in the study only if transthoracic US confirmed a pleural effusion of at least 10 mm (as measured from the parietal pleura) and they had at least two clinical indicators of possible TB.
Transthoracic US
A consultant respiratory physician or a senior registrar under supervision performed the sonography (Toshiba Just Vision 200 SSA-320A; Toshiba Medical Systems Corporation, Tochigi-ken, Japan). The preferred patient position for the procedure was the sitting position, with the subject's arms folded across the chest and supported by a bedside table. Surveillance of the dorsolateral thoracic wall was performed by means of a standard 3.75 MHz sector probe. The presence of an effusion was confirmed by standard means.19 The size of the effusion was documented as follows: minimal (if the echo-free space was confined to the costophrenic angle); small (if the space was greater than the costophrenic angle but still within the range of the area covered with a 3.75 MHz curvilinear probe); moderate (if the space was greater than a one-probe range but within a two-probe range; and large (if the space was larger than a two-probe range).19 The biopsy site was subsequently identified, with safety being a main determinant. As a rule, the aspirations and biopsies were performed in the midscapular line. For minimal to moderate effusions, the biopsies were taken from the site of maximum effusion as determined by US. In case of a large effusion, the puncture site was chosen to be as low as possible, but not within 25 mm of the diaphragm. All aspirations and biopsies were performed ‘freehand’ (not under direct US guidance) and patients were requested to remain motionless during the procedures.
Diagnostic thoracentesis
Under sterile technique and local anaesthesia with lignocaine 1%, samples were obtained for pH analysis by means of an on-site blood gas analyser (Bayer Rapidlab 865 Blood Gas Analyzer, Siemens, Midrand, South Africa), chemical analysis, microbiology, cell counts and cytology. The chemical analyses included serum and pleural total protein, albumin, lactate dehydrogenase and pleural fluid ADA levels. Microbiological investigations included routine gram stains and cultures, as well as stains for acid-fast bacilli (Ziehl-Nielsen staining) and TB cultures (MGIT 960 liquid culture system, Becton Dickinson, Sparks, Maryland, USA). We defined a lymphocytic predominant effusion as one with >75% lymphocytes and/or a lymphocyte to neutrophil ratio >0.75.6
Closed pleural biopsies
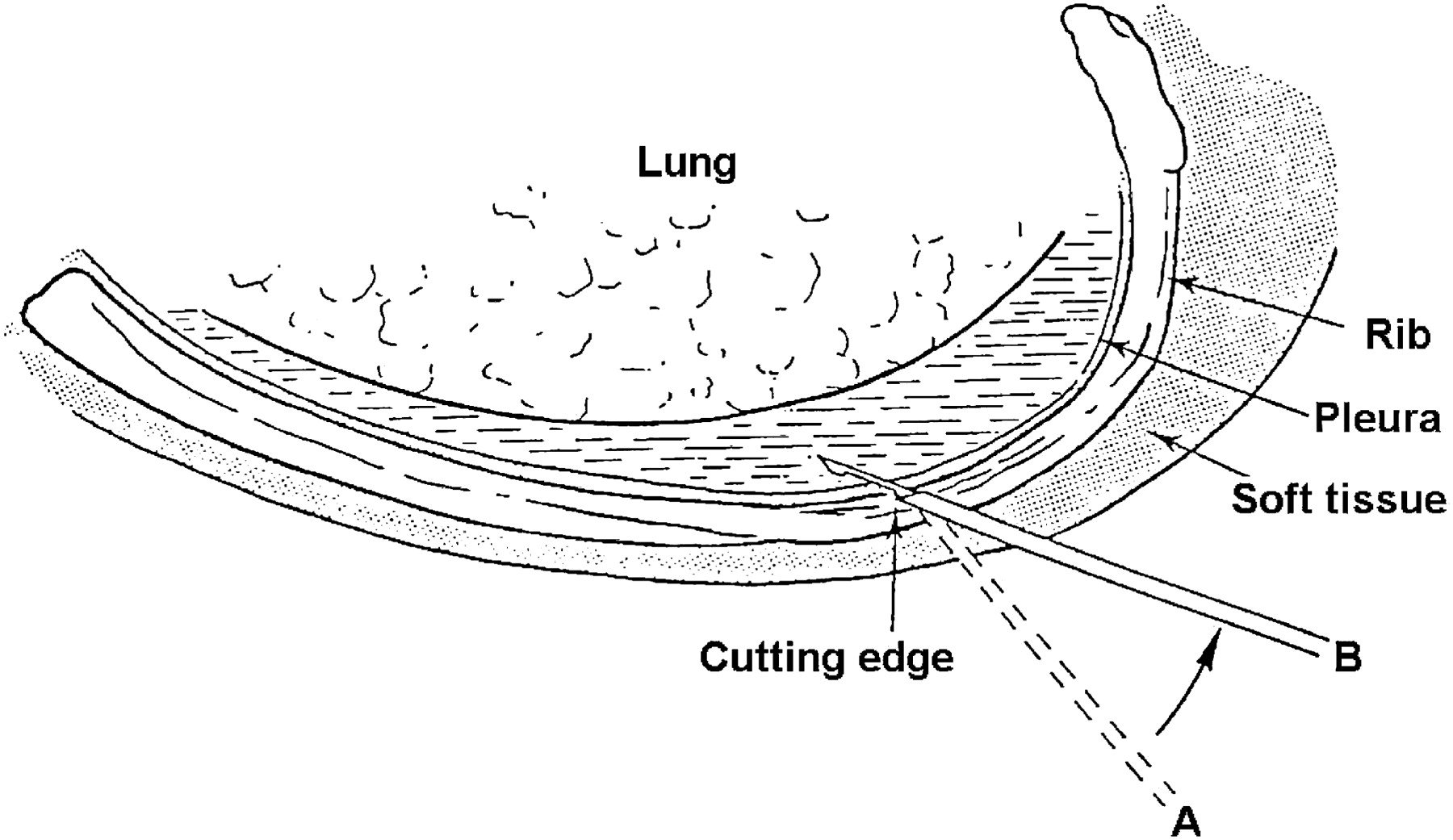
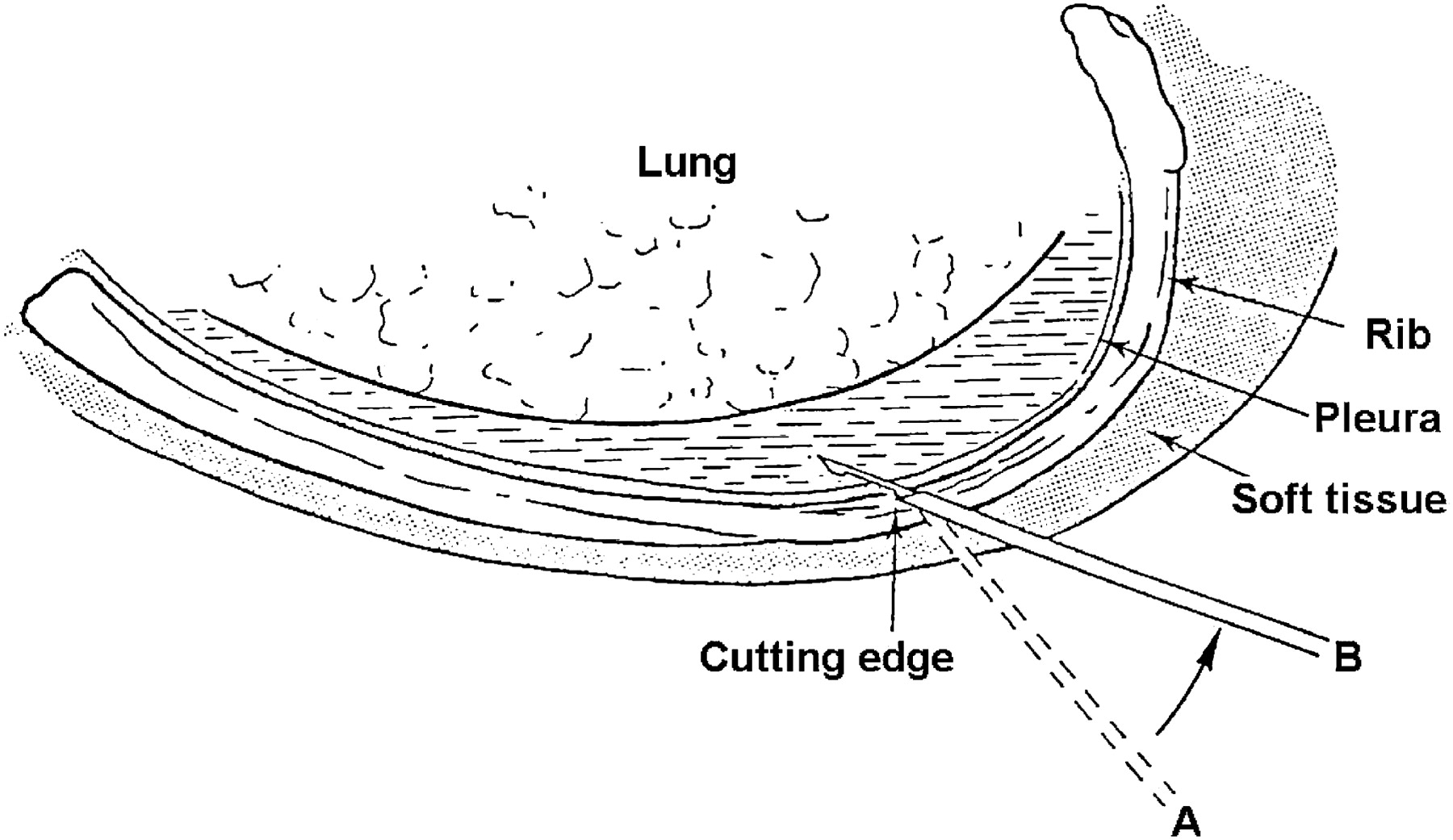
Under sterile technique and local anaesthesia, closed pleural biopsies were subsequently performed on all patients. Patients were randomly assigned (in blocks of six) to undergo either ≥4 Abrams needle biopsies followed by ≥4 Tru-Cut needle biopsies or ≥4 Tru-Cut needle biopsies followed by ≥4 Abrams needle biopsies. These biopsies were performed from the same incision site (5 mm in length) and by experienced clinicians. Abrams needle biopsies were performed according to standardised guidelines.20 21 Biopsies were taken with the distal tip of the needle facing up to 45° down in order to avoid laceration of the intercostal vessels. Cutting needle biopsies were performed by means of manually operated 14-gauge Tru-Cut biopsy needles with a specimen notch of 20 mm (Allegiance, Chateaubriand, France) and technically comparable to the way described by McLeod and coworkers (figure 1).16 Abrams and Tru-Cut needle biopsy specimens were harvested until each technique yielded at least three macroscopically satisfactory specimens for histological evaluation (transported in 4% formalin) and at least one specimen for microbiological investigations (transported in 0.9% saline).
{kind=link}
Cross section through an intercostal space showing the position of the open Tru-Cut needle immediately before harvesting a specimen. The Tru-Cut needle is cautiously introduced through an incision at 45° to the skin in the direction of the chosen intercostal space above the lower rib. Adjacent areas of pleura are then sampled. A distinct ‘give’ indicates entry into the pleural space, which is confirmed by the ease of advancement of the inner stylet. The whole Tru-Cut needle is then angled towards the skin (position A to B), allowing the inner stylet to be advanced along the inner aspect of the thoracic wall and away from the lung. The outer cutting sheath is subsequently advanced over the inner stylet, yielding biopsy samples of up to 2 cm of parietal pleura and intercostal muscle (adapted from McLeod et al14).
Immediate post-procedure care
The incision site was re-examined by means of US immediately after the procedures for suspected pneumothoraces, and a chest x-ray was obtained if the pre- and post-procedure US findings differed and at the discretion of the attending physician. All patients were observed for at least 1 h before discharge and complications were noted. Patient discomfort was documented, and excessive pain was defined as any pain requiring at least a single dose of parenteral or opiate analgesics. The presence or absence of minor or major haemorrhage as well as iatrogenic pneumothoraces was specifically documented. Major haemorrhage was defined as any haemorrhage that required additional measures above and beyond localised pressure and a single superficial suture.
Further assessment and follow-up
All patients with a non-diagnostic closed biopsy or thoracentesis were referred for medical thoracoscopy. Those who remained undiagnosed following medical thoracoscopy were followed up for a total of 6 months, and the choice of further investigations was guided by the patients' attending chest physicians. These could have included observation, video-assisted thoracoscopy or open surgical procedures. Cases that remained undiagnosed after 6 months were deemed ‘undiagnosed pleural exudates’. As the negative predicative value of medical thoracoscopy (when combining histology and microbiology) for TB pleuritis is practically 100% and its sensitivity for malignancy, in combination with fluid cytology and closed needle biopsies, is 97%, we decided upfront to retain these patients in the ‘non-tuberculous’ group for statistical analysis.6 22
Statistical analysis
We expected a diagnostic sensitivity of 80% for both devices based on our own historical data and data from Chang et al.6 17 Using the McNemar test for equal proportions, it was estimated that a total sample size of 220 patients was required to prove non-inferiority (difference of less than 10%). We were, however, unsure if the diagnostic sensitivity achieved by Chang et al17 in a relatively small study population would be reproducible, and given the paucity of data, practical constraints as well as patient safety aspects, it was decided to calculate the diagnostic yield for pleural TB of both needles after 36 months or after the inclusion of 100 patients, whichever came first. At 36 months (with 89 patients included), it became apparent that the yield of the Abrams needle for TB was consistent with the estimate,6 but that the yield for the Tru-Cut biopsy was clearly lower than anticipated. We terminated the study as the sensitivities for pleural TB differed significantly between the devises and subsequently analysed all the data at this point (McNemar test for equal proportions and χ2 tests with p<0.05 accepted as significant). Unless stated otherwise, data are displayed as mean±SD. We used standard methods to calculate the sensitivity, specificity, and positive and negative predictive values.23 For the purposes of the study, we accepted either histology compatible with TB (epithelioid granulomas with central necrosis, with or without acid-fast bacilli) or microbiological proof (pleura yielding a positive culture for M tuberculosis) on any pleural specimen as the gold standard.
Results
Patient characteristics and transthoracic US finding
A total of 89 patients (54 men) of mean±SD age 38.7±16.7 years were enrolled over a 3-year period: 8 had minimal effusions, 19 had small effusions, 36 had moderate effusions and 26 had large effusions. Pleural TB was diagnosed in 66 cases (74.2%; mean±SD age 35.1±15.5 years; 35 men). Of the remaining 23 patients (mean±SD age 49.1±15.9 years; 19 men), 20 (22.5%) had an alternative diagnosis and 3 (3.4%) remained undiagnosed (table 1). The HIV status of 37 patients was known at the time of enrolment: 16/26 (61.5%) of patients who were ultimately diagnosed with pleural TB were HIV positive compared with 4/11 (36.4%) in the group where TB was excluded (p=0.159).
Final diagnoses established in all patients (n=89)
Diagnostic thoracentesis
The pH analysis, biochemistry and microbiological results are summarised in table 2. In patients ultimately diagnosed with pleural TB, 90.9% had a lymphocyte predominant effusion and 89.4% had an ADA >50 IU/l. Combining these parameters yielded a sensitivity of 83.3%, specificity of 95.7%, positive predictive value of 98.2% and negative predictive value of 66.7% for pleural TB (table 3). Seven patients were found to have complicated parapneumonic effusions (with bacterial cultures) and malignant cells were present in five. None of these 12 individuals had histological evidence of pleural TB.
Diagnostic thoracentesis results of tuberculous versus non-tuberculous effusions: continuous and categorical variables
Diagnostic accuracy of pleural fluid analysis
Closed needle biopsies: diagnostic yield
Pleural tissue was present at histology in 91.0% of Abrams needle biopsies and 78.7% of Tru-Cut biopsies (p=0.015, table 4). Abrams needle biopsies had a yield for all diagnoses of 78.7% compared with 62.9% for Tru-Cut needles (p=0.014).
Diagnostic yield of Abrams and Tru-Cut needle biopsies (n=89)
In the 66 patients diagnosed with pleural TB, Abrams needle biopsies provided proof in 81.8%; 77.3% had histological evidence of TB and biopsies from 63.6% were culture positive for M tuberculosis. Tru-Cut needles yielded evidence of pleural TB in 65.2% (p=0.022); 60.6% of patients had histological evidence of TB (p=0.029) and biopsies from 39.4% were culture positive (p<0.001). Two of the 12 cases without a histological diagnosis of TB with Abrams needles were diagnosed on specimens harvested with Tru-Cut needles (a total of 56 patients were thus diagnosed with pleural TB on the basis of closed pleural biopsies).
Malignant pleural effusions were diagnosed in 12 patients. All had diagnostic closed pleural biopsies: Abrams needle biopsies yielded histological confirmation in 10 (83.3%) and Tru-Cut needle biopsies yielded histological confirmation in 8 (66.7%). Two cases not diagnosed with Abrams needles were both diagnosed on specimens obtained with Tru-Cut needles, and the four cases with false negative Tru-Cut biopsies (for malignancies) had positive Abrams needle biopsies. With regard to patients diagnosed with parapneumonic effusions (all with positive gram stains and cultures for bacteria on pleural fluid), acute pleuritis and/or non-specific inflammation were present in six specimens obtained by Abrams needles and five obtained by Tru-Cut needles.
Closed pleural biopsies: complications
The procedures were generally well tolerated and no pneumothoraces or major haemorrhages were documented. Two patients required parenteral analgesics; one complained of severe pain following Abrams needle biopsies and one following Tru-Cut biopsies (on both occasions the analgesics were administered following the second procedure). Two women (aged 20 and 22 years) experienced syncope following Abrams needle biopsies, both of whom recovered fully within 60 s (neither required any specific medical intervention). No procedure was abandoned due to complications.
Further assessment and follow-up
Thoracocentesis and closed pleural biopsy established aetiological diagnoses in 75 of the 89 patients. Diagnostic medical thoracoscopies were performed in 14. Aetiological diagnoses were subsequently made in a further 11 patients (10 cases of pleural TB and 1 of sarcoidosis). Three men aged 18, 51 and 63 years, respectively, remained undiagnosed. All were HIV negative, had minimal (n=1) or small (n=2) effusions, and specimens obtained during thoracoscopy either showed non-specific pleuritis (n=2) or pleural fibrosis (n=1). A complete radiological recovery was documented in all three cases and all were asymptomatic at 6-month follow-up.
Discussion
To the best of our knowledge, this is the largest prospective and the first randomised study performed to compare US-assisted Abrams needle biopsies with US-assisted Tru-Cut needle biopsies with regard to their diagnostic yield for pleural TB. We enrolled a relatively large population with a moderate to high pretest probability of pleural TB, and randomised patients to undergo either biopsy technique first in order not to disadvantage either needle. Abrams needle biopsies were more likely to contain pleural tissue (p=0.015) and to confirm the diagnosis of TB (p=0.022) than pleural biopsies obtained with Tru-Cut needles.
US-assisted Abrams needle biopsies had an overall diagnostic yield of 81.8% for TB pleuritis in a study population with a high pretest probability for the disease. We previously found medical thoracoscopy to have a diagnostic sensitivity of 100% for pleural TB.6 The present study establishes US-assisted Abrams needle biopsies as the principal technique for obtaining pleural tissue in patients with suspected TB pleuritis, with medical thoracoscopy being reserved for the small number of cases who are not diagnosed with closed biopsies.
In general, blind Abrams needle biopsies have a yield of 50–85% for TB pleuritis.6 24–28 Valdés and coworkers reported a diagnostic sensitivity of 79.8% when they analysed the case histories of 254 patients with confirmed pleural TB in a Spanish university hospital.27 Diacon et al found Abrams needle biopsies to have a diagnostic yield of 79% in patients with undiagnosed exudative pleural effusions who presented to our institution.6 We specifically enrolled patients with at least a moderate pretest probability of TB, which may account for the relatively high sensitivity. The use of US prior to closed pleural biopsies is currently advocated,19 29 30 both as a safety measure and to detect localised pleural thickening and other abnormalities.29 30 Pleural TB is a diffuse disease process,25 and it can therefore be postulated that the addition of US prior to the Abrams needle biopsies is unlikely to affect the sensitivity. Although we did not specifically employ US to detect localised abnormalities, our findings certainly support this.
Tru-Cut biopsies yielded pleural tissue in 78.7% of patients in the study, with a diagnostic sensitivity of 65.2% for pleural TB and 66.7% for malignancy. Chang et al conducted the only other prospective study that specifically compared the diagnostic yield of US-guided pleural biopsy with a Tru-Cut needle and (blind) pleural biopsy with an Abrams needle.17 They enrolled 49 patients with unilateral pleural effusions, 24 of whom underwent pleural biopsy with an Abrams needle and 25 underwent US-guided pleural biopsy with a Tru-Cut needle. Only 17 patients had pleural TB. Abrams needle biopsies were diagnostic in 20% (2/10) whereas Tru-Cut needle biopsies were diagnostic in 86% (6/7). The diagnostic yields for malignancies were 44% and 77%, respectively. Four major differences in the studies should be highlighted. We enrolled almost four times as many patients with pleural TB, performed thoracic US before all biopsies, used both biopsy needles in all cases and specifically reported the presence of pleural tissue at histology. Furthermore, we used liquid culture media which have a proven superior yield for the culture of M tuberculosis.31 32
We encountered a number of unexpected results. All pleural malignancies were diagnosed by means of either the Abrams or Tru-Cut needles, and the combined diagnostic yield was therefore 100%. Although this study was not designed to specifically address this issue, this figure is significantly higher than reported figures.33 Malignant disease tends to give rise to focal involvement,25 and the lower thoracic and diaphragmatic parietal pleura are more likely to contain secondary seeding from visceral pleural metastases.34 35 We aimed to use relatively low (supradiaphragmatic) biopsy sites, which may partially explain the relatively high yield observed in our study. Moreover, we harvested at least six specimens per patient for histology, and it is known that the yield of closed biopsies increases with increasing number of biopsies.25 We did not specifically evaluate the role of US in predicting pleural malignancies, as recently reported by Qureshi and coworkers.36 In their study, US correctly identified 73% of malignant effusions on appearance alone.36 The yield of US-assisted closed pleural biopsies in experienced hands may be much higher than previously believed and certainly deserves to be studied prospectively.
We found the Abrams needle to have a significantly superior yield for all diagnoses, and our data even suggested a comparable yield for pleural malignancy. Tru-Cut pleural biopsies can safely be performed in the presence of very little pleural fluid and have a diagnostic yield for pleural malignancy that is generally reported to be superior to that of Abrams needle biopsies.17 19 26 30 Maskell and co-workers previously found CT-guided Tru-Cut pleural biopsies to have a superior sensitivity of 87% for pleural malignancies compared with 47% for unaided Abrams needle biopsies.33 Local disease prevalence may therefore dictate the choice of biopsy needle, and the Tru-Cut needle may still be the needle of choice in patients with suspected pleural malignancy.
Kitinya et al found that the HIV status of a patient impacted on pleural biopsy results.37 Their data suggested that granulomas were less likely to be observed, whereas pleural tissue from HIV positive patients was more likely to be culture positive. However, in our study population the majority of patients diagnosed with pleural TB by means of closed pleural biopsies had granulomas on histology, and the addition of TB culture only marginally increased the overall diagnostic yield.
Our data confirm previous findings on the very high specificity of an ADA >50 IU/l in the presence of a lymphocyte predominant effusion.6 38 We found specificity of 95.7% and a positive predictive value of 98.2%. More important was the observation that, in a population with a high pretest probability for TB, pleural TB could be diagnosed in the majority of cases without the need for a pleural biopsy.
After 3 years it became evident that we had to abandon the original non-inferiority design as the sensitivity of the Tru-Cut biopsies was significantly lower than the original estimation at this point. While this certainly could be viewed as a weakness in the original study design, we strongly believe that this had no impact on the conclusion of the study. We collected robust data with complete follow-up. The end points used were dichotomous objective laboratory parameters which are not subject to random variation. Furthermore, the study design was on par with other studies in the field and the achieved sample size was at the higher end of the spectrum.6 14 17 18 33
In conclusion, US-assisted pleural biopsies performed with an Abrams needle are more likely to contain pleura and have a significantly higher diagnostic sensitivity for pleural TB. The Abrams needle should be the needle of choice for closed pleural biopsies in the setting of probable tuberculous effusions.
Acknowledgments
The authors thank Professor Martin Kidd (The Centre for Statistical Consultation, University of Stellenbosch) for his assistance with the statistical analysis of study data.
References
Footnotes
Linked articles 131219.
Funding Holland Stellenbosch Medical Foundation.
Competing interests None.
Ethics approval The Committee for Human Research of the University of Stellenbosch approved the study and written informed consent was obtained from all subjects on enrolment and prior to any invasive procedures.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Airwaves