Article Text

Abstract
Background: Increased numbers of activated neutrophils have been reported in the bronchial mucosa of patients with stable chronic obstructive pulmonary disease (COPD), particularly in severe disease.
Objectives: To investigate the expression of neutrophilic chemokines and adhesion molecules in bronchial biopsies from patients with stable COPD of different severity (GOLD stages I–IV) compared with age-matched control subjects, smokers with normal lung function and never smokers.
Methods: The expression of CCL5, CXCL1, 5, 6, 7 and 8, CXCR1, CXCR2, CD11b and CD44 was measured in the bronchial mucosa using immunohistochemistry, confocal immunofluorescence, real-time quantitative polymerase chain reaction (RT-QPCR) and Western blotting (WB).
Results: The numbers of CCL5+ epithelial cells and CCL5+ and CXCL7+ immunostained cells were increased in the bronchial submucosa of patients with stable severe COPD compared with control never smokers and smokers with normal lung function. This was also confirmed at the level of mRNA expression. The numbers of CCL5+ cells in the submucosa of patients with COPD were 2–15 times higher than any other chemokines. There was no correlation between the number of these cells and the number of neutrophils in the bronchial submucosa. Compared with control smokers, the percentage of neutrophils co-expressing CD11b and CD44 receptors was significantly increased in the submucosa of patients with COPD.
Conclusion: The increased expression of CCL5 and CXCL7 in the bronchial mucosa of patients with stable COPD, together with an increased expression of extracellular matrix-binding receptors on neutrophils, may be involved in the pathogenesis of COPD.
Statistics from Altmetric.com
Inflammation occurs in the central peripheral airways (bronchioles) and lung parenchyma of patients with COPD.1 2 3 4 Studies have emphasised the potential pathological role of many inflammatory cells including macrophages and T lymphocytes, whereas fewer investigations have examined neutrophil granulocytes despite increased numbers being present in the bronchial mucosa, particularly in severe disease.4 5 6 7 8 9 Furthermore, the need for more pathological investigations in patients with severe COPD has been highlighted.3
Several chemokines of the CXC and CC family are involved in neutrophil chemotaxis.10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 CXC chemokines were principally investigated using bronchoalveolar lavage (BAL) fluid or sputum samples, and increased levels of CXCL112 and CXCL821 in sputum or CXCL5 in BAL fluid14 have been reported in patients with COPD.
Fewer studies have investigated the expression of CC chemokines in COPD. CCL5 levels are increased in the sputum of patients with COPD.23 The leukocyte αMβ2 integrin (also known as CD11b/CD18) functions as an adhesion molecule facilitating diapedesis. Overexpression of CD11b has been reported in peripheral blood neutrophils26 27 and sputum28 of patients with COPD. Finally, hyaluronan, an extracellular matrix component, is the main ligand for CD44 and its expression is upregulated in neutrophils co-cultured with human primary bronchial epithelial cells and granulocyte-macrophage colony stimulating factor (GM-CSF).31 The expression of CD11b and CD44 on neutrophils in the bronchial mucosa of patients with COPD has not been previously reported (see online data supplement for a more detailed background).
The mechanisms responsible for tissue neutrophilia in COPD have not been fully clarified. The prevalence of neutrophils can be related to increased chemotaxis, increased adhesion to collagens or to prolonged survival. A partial loss of neutrophilic chemotactic response to CXCL8 stimuli has recently been reported for sputum neutrophils in patients with COPD after migration and residence in the bronchial lumen.10 Furthermore, a comprehensive analysis of chemokine expression in COPD bronchi is lacking.
The aim of the present study was to investigate the presence of relevant CXC and CC chemokines, cytokines and chemokine receptors involved in neutrophilic migration and activation in bronchial biopsies from patients with increasing disease severity. Since increased adhesion of neutrophils to extracellular matrix components may play a role in neutrophil permanence in the bronchial mucosa, the expression of two neutrophil receptors, CD11b and CD44, potentially involved in this process was also studied.
Methods
Subjects
All subjects were recruited from the Section of Respiratory Medicine of the Fondazione Salvatore Maugeri (Veruno, Italy). Table 1 and Tables E1–E3 (in the online data supplement) show the clinical characteristics of the subjects used for the immunohistochemistry (n = 49), confocal microscopy (n = 8), real-time PCR (RT-PCR, n = 31) and Western blotting (n = 12) studies. The severity of the airflow obstruction was staged according to the GOLD criteria.1
Characteristics of subjects for the optical immunohistochemical study
Lung function tests and volumes
Pulmonary function tests were performed as previously described6 according to published guidelines (see online data supplement).
Fibreoptic bronchoscopy, collection and processing of bronchial biopsies
A standardised procedure, previously reported,6 was followed for fibreoptic bronchoscopy and collection of bronchial biopsies. Bronchial biopsies for immunohistochemistry, Western blot analysis and RT-QPCR were processed as previously described6 (see online data supplement for details).
Immunohistochemistry
A panel of antibodies was used (table 2) and primary antibodies were applied at optimal dilutions in TRIS-buffered saline and revealed with the use of appropriate secondary antibodies and fast-red substrate (see online data supplement for details).
Antibodies used to characterise inflammatory cells and CXC, CC chemokines, their receptors and other molecules involved in the neutrophilia of the bronchial mucosa
Immunofluorescence staining with confocal microscopy
Sections were fixed with 4% paraformaldehyde, washed with phosphate buffered saline (PBS) and incubated with blocking serums followed by incubation with primary antibodies and the revealing antibody system, as previously described32 (see online data supplement for details).
Scoring system for immunohistochemistry and confocal microscopy
Light microscopic analysis was performed at a magnification of 630×. Immunostained cells in the bronchial submucosa were quantified as previously described.6 The immunostaining was also scored in the bronchial epithelium. The quantitative estimation of co-localised proteins was performed calculating the “co-localisation coefficients”32 (see online data supplement for details).
Quantification of chemokine and cytokine mRNA levels in bronchial biopsies
Total RNA was extracted (Micro RNeasy Kit, Qiagen, Milan, Italy) from 30 μm thick cryostat sections of bronchial biopsies and 1 μg used for cDNA synthesis. Relative levels of mRNAs were expressed as the ratio of the Ct value for the gene of interest Ct/housekeeping gene Ct (see online data supplement for details).
Western blot analysis for CCL5, CXCL7 and CXCL8 in bronchial biopsies
Whole cell protein extraction from bronchial biopsies, gel electrophoresis, nitrocellulose filters transfer, incubation with appropriate primary antibodies, detection on nitrocellulose filters and protein quantification were performed as previously described6 (see online data supplement for details).
Data analysis
Group data were expressed as mean (SEM) for functional data or median (range) for morphological data. Differences between groups were analysed using analysis of variance (ANOVA or Kruskal-Wallis as appropriate) for functional data or non-parametric tests for morphological parameters (see online data supplement for details).
Results
Clinical findings
The characteristics of subjects used for immunohistochemistry are shown in table 1. Tables E1–E3 (see online data supplement) show the characteristics of subjects used for confocal immunofluorescence, RT-QPCR and Western blotting, respectively. The four groups of subjects were of similar age (table 1). Smoking history was similar in patients with mild/moderate COPD, severe COPD and healthy smokers with normal lung function. As expected from the selection criteria, the values of forced expiratory volume in 1 s (FEV1 % predicted) and FEV1/forced vital capacity (FVC) (%) were significantly different in the groups with mild/moderate and severe/very severe COPD compared with both control groups (healthy smokers and healthy never-smokers). Patients with severe/very severe COPD also differed significantly from those with mild/moderate COPD (for overall groups, p<0.001 (ANOVA) for FEV1% predicted and FEV1/FVC% values).
Immunohistochemistry
Neutrophils in bronchial submucosa
The number of neutrophils, as previously reported,6 was significantly higher in the bronchial submucosa of patients with severe/very severe COPD (274 (range 47–500)) compared with control healthy smokers (124 (17–308), p = 0.008) and healthy never smokers (110 (59–270), p = 0.009; table 3). Patients with mild/moderate COPD did not differ significantly from both control groups, nor did the two control groups differ significantly from each other.
Quantification of inflammatory cells and chemokines and their receptors in the bronchial epithelium and submucosa of patients with COPD stratified by GOLD stage of severity, control smokers with normal lung function and control non-smoking subjects
Neutrophilic chemokines and their receptors
Immunohistochemical expression of neutrophilic chemokines and their receptors in bronchial epithelium
CXCL1 expression was significantly increased in the bronchial epithelium in patients with severe/very severe COPD compared with control healthy never-smokers (p = 0.040, Mann-Whitney U test). Similarly, CXCL8 expression was significantly increased in the bronchial epithelium of patients with severe/very severe COPD compared with control healthy smokers (p = 0.022, Mann-Whitney U test). CCL5 showed significantly enhanced expression in the bronchial epithelium of patients with severe/very severe COPD compared with control healthy smokers (p = 0.042) and healthy never smokers (p = 0.048, Mann–Whitney U test). Finally, CXCR2 was significantly increased in patients with severe/very severe COPD compared with patients with mild/moderate COPD (p = 0.043) and control healthy smokers (p = 0.018, Mann-Whitney U test; table 3). No significant differences were observed between the four groups of subjects for all the other proteins investigated in the bronchial epithelium.
Immunohistochemical expression of neutrophilic chemokines and their receptors in bronchial submucosa
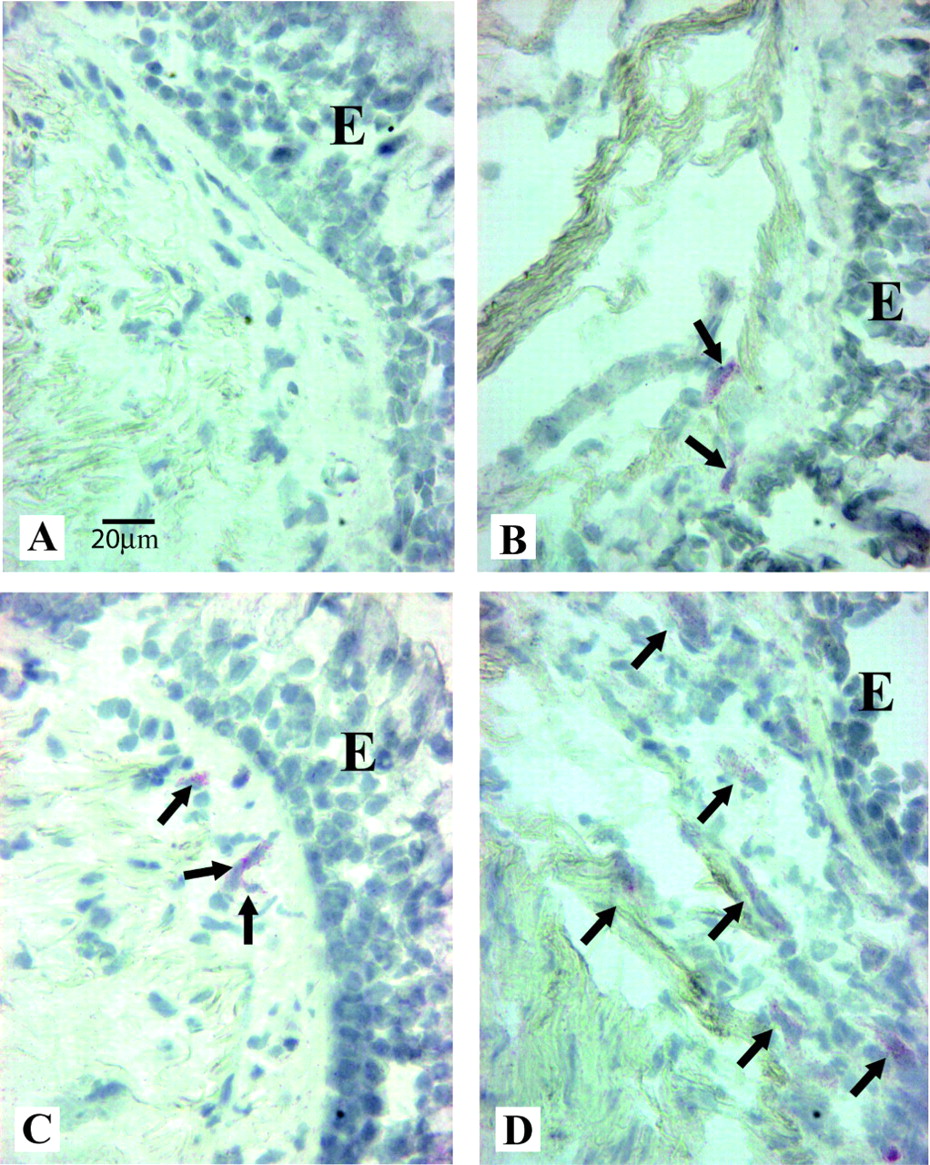
CCL5 immunostaining was the one most abundantly observed in this study and was present in inflammatory and structural cells—mainly in endothelial cells and occasionally in the smooth muscle—within the bronchial submucosa (fig 1). The number of CCL5+ cells was significantly higher in patients with severe/very severe COPD (281 (range 75–839)) than in control healthy never-smokers (77 (range 26–203), p = 0.002), but it did not differ from control smokers or patients with mild/moderate COPD (table 3).

Photomicrographs showing the bronchial mucosa from (A) a control non-smoker, (B) a healthy smoker with normal lung function, (C) a patient with mild/moderate stable chronic obstructive pulmonary disease (COPD) and (D) a patient with severe stable COPD immunostained for identification of CCL5+ cells (arrows) in the submucosa. The results are representative of those from 11 non-smokers, 13 healthy smokers, 12 patients with mild/moderate COPD and 13 with severe COPD. E = epithelium. Bar = 20 μm.
Immunostaining for CXCL7 was observed in inflammatory cells, endothelial cells, fibroblasts and submucosal glands in the bronchial submucosa (fig 2), but its expression was 2–7 times lower than that for CCL5. The number of CXCL7+ cells was significantly higher in patients with severe/very severe COPD (37.6 (range 0–82.9), p = 0.004) than in control healthy never-smokers (13.8 (0–32.3), table 3).
Photomicrographs showing the bronchial mucosa from (A) a control non-smoker, (B) a healthy smoker, (C) a patient with mild/moderate stable chronic obstructive pulmonary disease (COPD) and (D) a patient with severe stable COPD immunostained for identification of CXCL7+ cells (arrows) in the submucosa. The results are representative of those from 11 non-smokers, 13 healthy smokers, 12 patients with mild/moderate COPD and 13 with severe COPD. E = epithelium. Bar = 20 μm.
In contrast, immunostaining for CXCL1 and CXCL6 was observed in relatively few inflammatory cells and endothelial cells in the bronchial submucosa, and the numbers of CXCL1+ and CXCL6+ cells did not differ between the four groups studied. The number of CXCL1+ cells in the bronchial submucosa was 7–10 times lower than CCL5 and the number of CXCL6+ cells was 2–7 times lower than CCL5 (table 3).
CXCL5 immunostaining was localised in inflammatory and endothelial cells in the bronchial submucosa. The numbers of CXCL5+ cells was significantly lower in patients with severe/very severe COPD (78.3 (range 19–424), p = 0.025) than in those with mild/moderate COPD (167.7 (107–266), table 3).
CXCL8 immunostaining was observed in few inflammatory cells and occasionally in capillary vessels (endothelial cells) and smooth muscle cells in the bronchial submucosa, its expression being 5–15 times lower than that of CCL5. No significant differences were observed in the numbers of CXCL8+ cells between any of the groups studied (table 3).
Immunostaining for CXCR1 was observed in inflammatory cells, endothelial cells and, to a lesser extent, in fibroblasts within the bronchial submucosa. The number of CXCR1+ cells in the bronchial submucosa of control healthy smokers (161.3 (range 64–301), p = 0.038) was significantly higher than in control healthy never-smokers (69.1 (39.4–612.9)) but not than the other groups. Similar to CXCR1, immunostaining for CXCR2 was observed in inflammatory cells, endothelial cells and, to a lesser extent, in fibroblasts. No significant differences were observed in the numbers of CXCR2+ cells counted in the bronchial submucosa of the four groups studied (table 3).
CD11b staining was observed in inflammatory cells, endothelial cells, fibroblasts and occasionally in the smooth muscle with no significant differences being observed between any of the groups studied. CD44 staining was also observed in inflammatory cells, fibroblasts, endothelial cells and occasionally in the smooth muscle, and again no significant differences were observed in the numbers of CD44+ cells counted in the bronchial submucosa between any of the groups (table 3).
Immunofluorescence with confocal microscopy double staining for identification of neutrophil granulocytes co-expressing CD11b or CD44
Confocal microscopy showed that the percentage of neutrophils co-expressing CD11b in the bronchial submucosa was significantly higher in patients with severe/very severe COPD than in control healthy smokers (mean (SD) 46 (5)% vs 16 (4)%, p = 0.02). Similarly, the percentage of neutrophils co-expressing CD44 was significantly increased in patients with severe/very severe COPD compared with control healthy smokers (mean (SD) 48 (6)% vs 14 (4%), p = 0.02; fig 3).
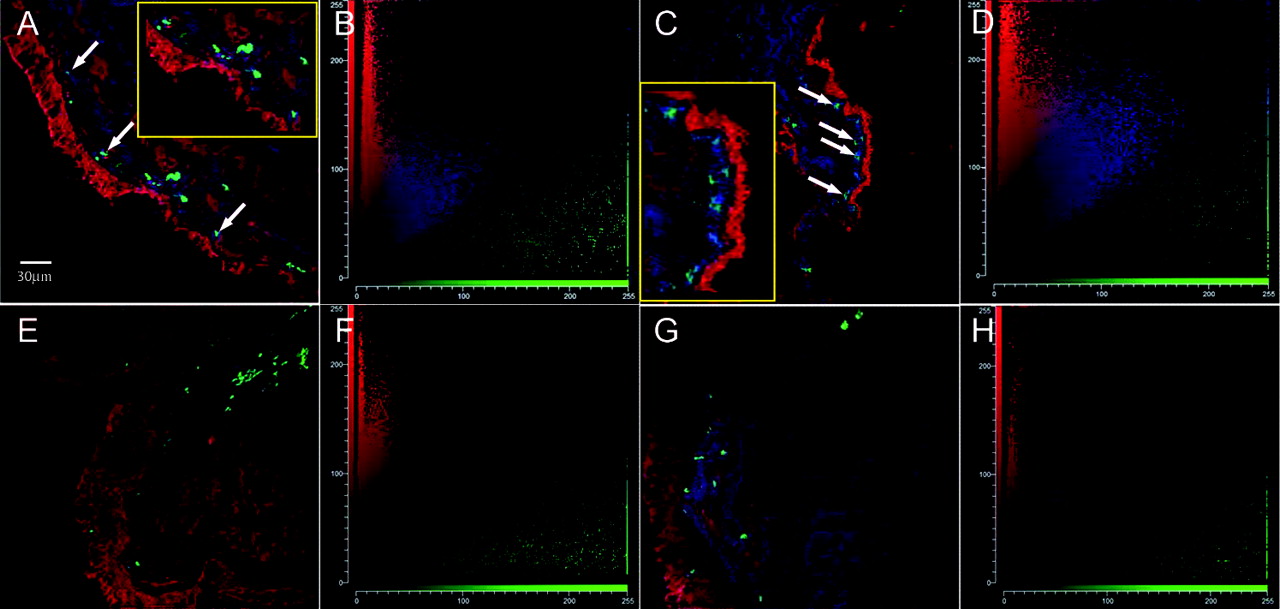
Representative double-labelled confocal fluorescence images showing double staining for neutrophil elastase and CD44 or CD11b in the bronchial mucosa from four patients with stable chronic obstructive pulmonary disease (COPD) (A–D) and four healthy smokers (E–H). Cryostat sections were fixed with paraformaldehyde and incubated with the primary and secondary antibodies. Images A and C were obtained from one patient with severe COPD. Images E and G were obtained from a control healthy smoker. Images A and E show the co-expression levels of neutrophil elastase (Alexa Fluor 488-green) and CD44 (Alexa Fluor 647-red), whereas images C and G represent the co-expression levels of neutrophil elastase (Alexa Fluor 488-green) and CD11b (Alexa Fluor 647-red). Co-localised pixels are shown in blue (arrows). Panels B, D, F and H show the correlation cytofluorogram of the images in A, B, C and E, respectively. Inserts show double-stained cells at higher magnification.
Quantification of neutrophilic chemokine mRNA levels
The mRNA levels expressed as 45−ΔCt and relative levels of mRNAs expressed as the ratio of the gene of interest Ct/housekeeping Ct (guanine nucleotide binding protein (G protein) – GNB2L) are shown in table 4. Whether measured as relative or absolute levels, the expression of CXCL7 and CCL5 mRNA was significantly higher in biopsy specimens from patients with COPD than in those from control healthy smokers with normal lung function. In contrast, there was no significant difference in the expression of CXCL8 mRNA between these two groups.
Results of the RT-QPCR study
Western blot analysis for CCL5, CXCL7 and CXCL8
From Western blot analysis, no significant difference was seen in the expression of CCL5 in bronchial biopsies from patients with COPD compared with healthy smokers with normal lung function (CCL5/actin ratio 0.84 (0.07) vs 0.63 (0.09), p = 0.06, fig 4). CXCL7 (data not shown) and CXCL8 expression (fig 4) were both below the detection threshold in the bronchial mucosa of patients with COPD and control healthy smokers with normal lung function.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Representative Western blot analysis of (a) CCL5 and (b) CXCL8 expression in bronchial biopsies of three patients with stable chronic obstructive pulmonary disease (COPD). Total cellular proteins were size-fractionated by SDS-PAGE and CCL5 and CXCL8 were detected using specific antibodies. The positive control lane in (b) has been loaded with human recombinant (hr) CXCL8. Western blotting was performed on five smokers with normal lung function and seven patients with COPD.
Correlations between inflammatory cell counts, neutrophilic chemokines and their receptors and clinical parameters
In all smokers the number of neutrophils in the bronchial submucosa correlated positively and significantly with CD44 epithelial expression (r = 0.47, p = 0.046). No other statistically significant correlations were found between inflammatory cells and neutrophilic chemokine expression or any clinical parameters.
Discussion
This study demonstrates for the first time the presence of an increased number of CCL5+ and CXCL7+ cells and an increased expression of both CCL5 and CXCL7 mRNA in the bronchial mucosa of patients with severe/very severe COPD in the stable phase as well as an increased number of neutrophils in the bronchial submucosa. We also found a significant upregulation of CD44 and CD11b receptors on neutrophils within the bronchial submucosa of patients with COPD compared with control healthy smokers.
CCL5 was the most abundant chemokine expressed in the bronchial mucosa of patients with severe COPD, showing levels of immunostained cells 2–15 times higher than those of other chemokines. The increased expression of both CCL5 and CXCL7 mRNA in the patients with COPD compared with control healthy smokers indicates that the expression of these chemokines is regulated at the transcriptional level and/or by increased mRNA stabilisation. Looking at the total protein expression by Western blot analysis, we found a trend towards increased CCL5 expression in the bronchial mucosa of patients with COPD compared with control healthy smokers, in agreement with RT-QPCR analysis. These findings are apparently in contrast to our quantification of CCL5+ cells by immunohistochemistry in the submucosa which showed a statistically significant difference only when patients with severe/very severe COPD were compared with control healthy never smokers. This may be due to the fact that quantification of the total amount of mRNA or protein by RT-QPCR or Western blotting, respectively, represents the sum of epithelial and submucosal mRNA expression or the sum of intracellular and extracellular proteins in the bronchial mucosa, not necessarily corresponding to the direct quantification of the number of cells expressing the same molecule as performed by immunohistochemistry in a single compartment (ie, the submucosa). CCL5 binding to glycosaminoglycans on the cell surface or in the extracellular matrix sequesters CCL5, thereby immobilising CCL5 to provide a directional signal.33 This may explain why increased levels of CCL5 have been reported in the BAL fluid of patients with COPD with a bronchodilator response compared with non-smoking subjects,34 and why lipopolysaccharide-stimulated COPD cultured lung explants release more CCL5 than control healthy smokers.25 In fact, part of this extracellular chemokine can be released after stimulation or recovered in the BAL fluid. Furthermore, the lack of a significant positive correlation between numbers of neutrophils and numbers of CCL5+ cells populating the bronchial mucosa, observed in the present study, may also be partly due to this intracellular and extracellular CCL5 protein distribution pattern. In addition, our finding that increased neutrophilia in the bronchial mucosa is dependent on different mechanisms such as the increased presence of chemotactic stimuli and increased neutrophil adhesiveness suggests that a direct correlation between numbers of neutrophils and every chemotactic factor could not be found, as we observed. These data also suggest that studies on the expression of neutrophilic chemokines obtained in different compartments such as blood, sputum and BAL fluid may not be fully representative of the inflammatory cascade recruiting cells in the lower airways of patients with COPD. In addition, the low levels of CXCL7 and CXCL8 expression seen by immunohistochemistry were reflected in the inability to detect these proteins by Western blotting, which requires a much higher level of protein expression than immunohistochemistry.
The chemokine receptors CXCR1 and CXCR2 were not significantly different in the four groups of subjects studied except for a significantly increased expression of CXCR2 in the epithelium of patients with severe COPD compared with control healthy smokers and patients with mild/moderate COPD. This suggests that there may be enhanced activation of CXCR2 in stable severe disease, possibly interacting with the increased CXCL7 ligand and both contributing, in part, to increased neutrophilia in patients with severe/very severe COPD. We believe, however, that the lack of a significant increase in CXCR1, CXCR2 and related CXC chemokines in the bronchial submucosa of our patients indicates that these receptors/chemokines do not have a major role during stable COPD, but they may have a more prominent role during COPD exacerbations as the expression of CXCL5, CXCL8, CXCR1 and CXCR2 has been reported to be increased in bronchial biopsies of patients with COPD with severe exacerbations.15
Functionally, CCL5 is a member of a family of CC chemokines that includes other members such as CCL2, CCL3 and CCL4 with strong chemoattractant activity towards monocytes and natural killer (NK) cells. We previously reported increased levels of CCL2 and CCL4 in the BAL fluid of patients with stable COPD compared with control smokers,35 and an upregulation of CCL3 in the bronchial epithelium and an increased number of NK+ cells in the bronchial submucosa of patients with severe/very severe COPD compared with control healthy smokers.5 Together these findings suggest that, in patients with stable COPD, CC chemokines may play a predominant role in sustaining tissue neutrophilia and infiltration of macrophages and NK cells. In contrast, CXC chemokines and their receptors predominate during COPD exacerbations.11 15 The fact that CXCL1, CXCL5 and CXCL6 were not changed in the submucosa of patients with COPD in comparison with both control groups in the present study further confirms our view of a major role for CC chemokines in the bronchial tissue of patients with stable COPD. CCL5 is also chemotactic for eosinophils, but an increased number of eosinophils in the bronchial mucosa has only been demonstrated during COPD exacerbations15 and not in stable disease.4 For this reason we did not quantify the number of eosinophils in the bronchial mucosa of patients with stable COPD.
Interestingly, we report here for the first time that expression of the receptors CD11b and CD44 in the neutrophils is 3–4 times higher in the bronchial submucosa of patients with COPD than in control healthy smokers, suggesting a greater activation state and higher adhesive capability of these cells to bind to submucosal extracellular matrix components. This further supports a role for these receptors in anchoring neutrophils to some components of the extracellular matrix such as hyaluronic acid molecules and adhesion molecules such as intercellular adhesion molecule 1 (ICAM-1) and endothelial-leucocyte adhesion molecule 1 (ELAM-1). ELAM-1 is highly expressed in bronchial capillary vessels whereas ICAM-1 is preferentially expressed in the epithelium of the bronchial mucosa.29 These data, obtained from segmental and subsegmental bronchi, need to be evaluated in the smaller bronchi and bronchioles of patients with COPD.
Differences in the environment between tissue and sputum may account for the differences in the activation status of neutrophils seen in the bronchial mucosa and those isolated from sputum which show a hypofunctional state and chemotactic response.10 The fact that sputum neutrophils are usually in a terminal stage of life may also contribute to these differences and further underlines the importance of data obtained from analysis of the bronchial tissue of patients with COPD.
In conclusion, the prominent expression of the chemokine CCL5 and, to a lesser extent, of CXCL7 together with higher neutrophil adhesiveness may account for the increased neutrophilia observed in the bronchial mucosa of patients with severe COPD. Identification of the individual contribution of each of these chemokines in inducing neutrophilia in patients with severe/very severe COPD will require clinical trials using selective antagonists or blocking antibodies to each of these molecules, many of which are already in development.
REFERENCES
Supplementary materials
web only appendix
Files in this Data Supplement:
Footnotes
▸ Additional details are published online only at http://thorax.bmj.com/content/vol64/issue11
ADS and GC contributed equally to this work.
Funding This work was supported by Fondazione Salvatore Maugeri, IRCCS, Ricerca Corrente and Regione Piemonte, Ricerca Sanitaria Finalizzata. IMA and PJB are supported by the Wellcome Trust.
Competing interests None.
Ethics approval The study conformed to the Declaration of Helsinki. Ethics consent was obtained, bronchial biopsies were performed according to the local ethics committee guidelines and informed consent was obtained from each subject.
Provenance and Peer review Not commissioned; externally peer reviewed.