Article Text

Abstract
Background: The diagnosis of smear-negative pulmonary tuberculosis (TB) is problematic. There are limited data on the profile of alveolar TB antigen-specific T cells, and their utility for the rapid immunodiagnosis of pulmonary TB is unclear.
Methods: Antigen-specific interferon γ (IFNγ) responses to the RD-1 antigens ESAT-6 and CFP-10 (T-SPOT.TB and QuantiFERON-TB-Gold-In-Tube), heparin-binding haemagglutinin and purified protein derivative were evaluated, using alveolar lavage cells, in 91 consecutively recruited South African patients suspected of having TB.
Results: Of 85 evaluable patients (29% HIV+), 24, 11, 48 and 2 had definite TB, probable TB, non-TB and an uncertain diagnosis, respectively. Between 34% (T-SPOT.TB) and 41% (QuantiFERON-TB-Gold-In-Tube) of all test results were inconclusive. Failure of the positive control was significantly higher with the QuantiFERON-TB-Gold-In-Tube than with T-SPOT.TB (85% vs 46% of inconclusive results; p = 0.001). Using staphylococcal enterotoxin B, compared with phytohaemagglutinin, substantially reduced failure of the positive control (25% to 3%; p = 0.02). In evaluable samples, when the definite and non-TB groups were used for outcome analysis, the percentage sensitivity, specificity, positive predictive value and negative predictive value for T-SPOT.TB (⩾20 spots/million alveolar mononuclear cells) and QuantiFERON-TB-Gold-In-Tube (0.35 IU/ml) were 89, 94, 89 and 94% (n = 55) and 55, 86, 77 and 69% (n = 46), respectively. Rapid diagnosis of TB was achieved more frequently with T-SPOT.TB than with smear microscopy (14/24 (58%) vs. 7/24 (29%) of definite TB cases; p = 0.02). Heparin-binding haemagluttinin and purified protein derivative alveolar lymphocyte IFNγ responses had poor performance outcomes.
Conclusion: Provided evaluable results are obtained, the RD-1, but not the heparin-binding haemagglutinin or purified protein derivative, alveolar lymphocyte IFNγ ELISPOT response is a useful rapid immunodiagnostic test for TB. However, test utility in high-burden settings may be limited by the high proportion of inconclusive results.
Statistics from Altmetric.com
Sputum-scarce and smear-negative tuberculosis (TB) continues to pose a diagnostic conundrum to clinicians because the yield of rapid diagnostic tools is low and obtaining representative biological samples may be challenging. Smear microscopy has a poor sensitivity, and culture results take several weeks to obtain. Empiric treatment exposes patients to prolonged treatment with toxic drugs, and, if this fails, possible unnecessary therapy for drug-resistant TB. The only alternative rapid diagnostic tool, nucleic acid amplification testing (NAAT), has a variable and suboptimal sensitivity (∼40% in smear-negative pulmonary TB).1
Pulmonary TB is characterised by a robust Th1 (T helper 1) response, raising the prospect of rapid immunodiagnosis using TB antigen-driven alveolar T cell interferon γ (IFNγ) responses.2 3 4 5 6 7 Alveolar purified protein derivative (PPD)-specific T cell responses have been investigated as a TB diagnostic tool.8 However, PPD may drive pulmonary memory T cell responses in those with latent TB infection6 and/or exposure to non-tuberculous mycobacteria, and thus may have limited specificity. More recently, standardised rapid immunodiagnostic assays (T-SPOT.TB and QuantiFERON-TB Gold-In-Tube (QFT-GIT)), which evaluate IFNγ responses to the RD-1 antigens ESAT-6 and CFP-10, have been shown to be highly sensitive and specific tests for the diagnosis of TB infection9 10 11 but they cannot distinguish latent from active disease when using peripheral blood mononuclear cells (PBMCs).12 However, at the site of active TB, in contrast to non-tuberculous disease, there is an ∼10-fold higher frequency of TB antigen-specific T cells.13 14 15 Thus, it is reasonable to hypothesise that lung-orientated rapid immunodiagnosis of TB is possible using cells from affected pulmonary segments. Indeed, a preliminary study performed in Europe indicated that TB could be rapidly and accurately diagnosed with the T-SPOT.TB assay using bronchoalveolar lavage mononuclear cells (BALMCs).16 However, it remains unclear whether these outcomes can be reproduced in routine clinical practice, particularly in a high-burden TB and HIV setting where it would be most useful.
There are also several other unresolved questions. It is unclear whether alveolar antigen-specific responses distinguish between active and latent TB infection, how HIV infection impacts upon pulmonary immune responses and which antigens are most useful. The comparative diagnostic utility of the different standardised RD-1 assays (QFT-GIT and T-SPOT.TB) and other novel antigens (heparin-binding haemagglutinin (HBHA)) have not previously been evaluated using BALMCs. HBHA, a novel and relatively TB-specific antigen, may distinguish latent from active disease17 18 and may therefore be particularly well suited to pulmonary immunodiagnosis. However, in general, data about the immunological profile of TB antigen-specific pulmonary T cells are limited,8 15 16 and the optimal cell number and cut-off point needed for reliable immunodiagnosis are unclear.
To address these questions we prospectively evaluated antigen-specific IFNγ responses, including a head-to-head comparison between the T-SPOT.TB (RD-1 ELISPOT) and QFT-GIT (RD-1 ELISA) assays, and HBHA and PPD responses, using whole blood and BALMCs, in a well categorised cohort of 91 patients from Cape Town, South Africa suspected of having pulmonary TB.
Methods
Patient recruitment and investigation
Ninety-one consecutive patients with suspected pulmonary TB who were unable to expectorate sputum (sputum-scarce) or who were smear negative were prospectively recruited at Groote Schuur Hospital in Cape Town, South Africa (a study plan is outlined in fig 1). The study protocol was approved by the University of Cape Town Ethics Committee. Six patients were excluded (fig 1). There were thus 85 patients from whom evaluable samples were obtained. All patients had a history taken, detailed physical examination performed, routine investigations including testing for HIV infection, chest x ray, and bronchoscopy performed by an experienced pulmonologist under local anaesthesia and conscious sedation. Approximately 150–300 ml of sterile saline was used to lavage a radiologically involved lung segment. The aspirate (∼100–150 ml) was collected in a sterile glass bottle. Aliquots of bronchoalveolar lavage (BAL) fluid were sent for smear microscopy, Gram and fungal staining, cell differential count, cytology for malignant cells and Pneumocystis jirovecii, bacterial and fungal culture, and culture for Mycobacterium tuberculosis (MGIT 960). When appropriate, 3–5 transbronchial biopsies were performed.

Overview of study recruitment and the laboratory assays evaluated. BAL, bronchoalveolar lavage; HBHA, heparin-binding haemagglutinin; IRGA, interferon γ release assay; M.tb, Mycobacterium tuberculosis; PCP, Pneumocystis carinii pneumonia; PPD, purified protein derivative; QIF GIT, QuantiFERON-TB Gold-In-Tube; TB, tuberculosis.
The reference standard for TB was culture positivity for M tuberculosis and/or histology in keeping with TB (caseous necrosis or acid-fast bacilli with or without granuloma formation). Patients were thus characterised by an investigator blinded to the IFNγ release assay (IGRA) results as (1) definite TB (meeting the reference standard); (2) non-TB (alternative diagnosis made and not treated for TB); (3) probable TB (empiric anti-TB treatment with clinical response but not meeting the reference standard); and (4) uncertain diagnosis (patient lost to follow-up but not treated for TB and no alternative diagnosis made; thus TB could not be confirmed nor excluded).
Alveolar lymphocyte antigen-specific IFNγ responses (see online supplement for more detail)
The following alveolar antigen-specific IFNγ responses were evaluated.
RD-1 ELISPOT IFNγ responses to ESAT-6/CFP-10 peptide pools (T-SPOT.TB; Oxford Immunotec, Oxford, UK) were performed using 2×105 BALMCs per well (cell number selected by performing optimisation experiments in five patients; see online data supplement for details).
RD-1 ELISA-measured IFNγ responses to ESAT-6/CFP-10 and TB 7.7 antigens (QuantiFERON-TB Gold-In-Tube assay; Cellestis, Victoria, Australia) were performed using 1×106 BALMCs re-suspended in 1 ml of serum-free medium in each tube. The cell number and volume used were derived through optimisation experiments using BALMCs from 10 patients (see online data supplement).
PPD (10 μg/ml; Staten Serum Institute, Copenhagen, Denmark) IFNγ ELISPOT responses were performed in duplicate using IFNγ-pre-coated ELISPOT plates (Mabtech, Stockholm, Sweden) seeded with 2×105 BALMCs per well.
IFNγ ELISPOT responses to HBHA (concentration of 100 μg/ml derived from optimisation experiments; see online supplement) were performed in duplicate using IFNγ-pre-coated ELISPOT plates. Methylated HBHA antigen was produced in cultures of Mycobacterium smegmatis 3.38 as previously described.19 20 21
Results were deemed to be inconclusive if there were insufficient cells to perform the assay, if the positive control failed (indeterminate), if there was a high spot count/level in the negative control well/tube or, if there was high background discoloration of the ELISPOT wells precluding meaningful evaluation of the plate. In the second half of the study, in addition to phytohaemagglutinin (PHA), staphylococcal enterotoxin B (SEB) was used as a positive control.
Peripheral blood-derived antigen-specific IFNγ responses
Peripheral blood IFNγ responses (T-SPOT.TB, QFT-GIT, PPD and HBHA) were evaluated in each patient according to the methods already described.
Details of the statistical methods used are presented in the online repository. The study satisfies the Standards for Reporting of Diagnostic Accuracy (STARD initiative) checklist.22
Results
Demographic and clinical details
Demographic characteristics of the recruited patients are shown in table 1. Six patients were excluded from further analysis; thus there were 85 patients from whom evaluable cellular samples were obtained. Of the 85 patients, 24, 11, 48 and 2 had definite, probable, non-TB and an uncertain diagnosis, respectively. Of the tested patients (23/78), 29% were HIV positive.
Sociodemographic and clinical characteristics of the TB (n = 35) and non-TB (n = 48) groups
Smear microscopy, BAL fluid culture and transbronchial biopsies (tissue culture and histology) were positive in 7, 23 and 1 of the 24 definite TB cases, respectively, and, by definition, in none of the non-TB cases. None of the probable TB cases was culture or biopsy positive but all were treated empirically for TB based on clinical suspicion; all responded to anti-TB treatment. The most common causes of pulmonary infiltrates in the non-TB group are outlined in the online data supplement. The median BAL fluid volume recovered was 100 ml (range 40–200 ml).
RD1-driven ELISA and ELISPOT assays
Of the 85 evaluable BAL samples, the QFT-GIT assay was not performed in 3 patients, and was inconclusive (no interpretable result generated) in 34/82(41%) patients, thus leaving 48 samples with evaluable results. In contrast, the T-SPOT.TB was inconclusive in 28/83 (34%) patients, thus leaving 55 samples with evaluable results. A summary of the inconclusive BAL results is given in table 2 (full details are contained in the online supplement; table E8). Inconclusive results were defined as one of the following: (1) failed positive control; (2) failed negative control (high IFNγ level or spot count as defined by the manufacturer); (3) isolation of an inadequate number of cells (as defined in the Methods section) to perform the assay; or (4) high background discoloration of the well precluding determination of the result (applicable to the ELISPOT assay only).
Summary of the number of patients recruited, assay-specific inconclusive IGRA results, and the final number of participants used in the analysis
In 35 ELISPOT assays, paired positive controls (PHA and SEB; positive, negative or indeterminate) results were available; of these significantly more PHA-driven than SEB-driven positive controls failed (1/28 (3%) vs 7/28 (25%); p = 0.02; χ2; table E2 online supplement). In the analysis presented here a failed PHA but functional SEB control was accepted as a valid result. High spot counts in the negative control well occurred in a higher proportion of HIV-positive versus negative subjects (54% vs 22% p = 0.01), but was not associated with a history of previous TB or BAL bacterial or fungal culture results.
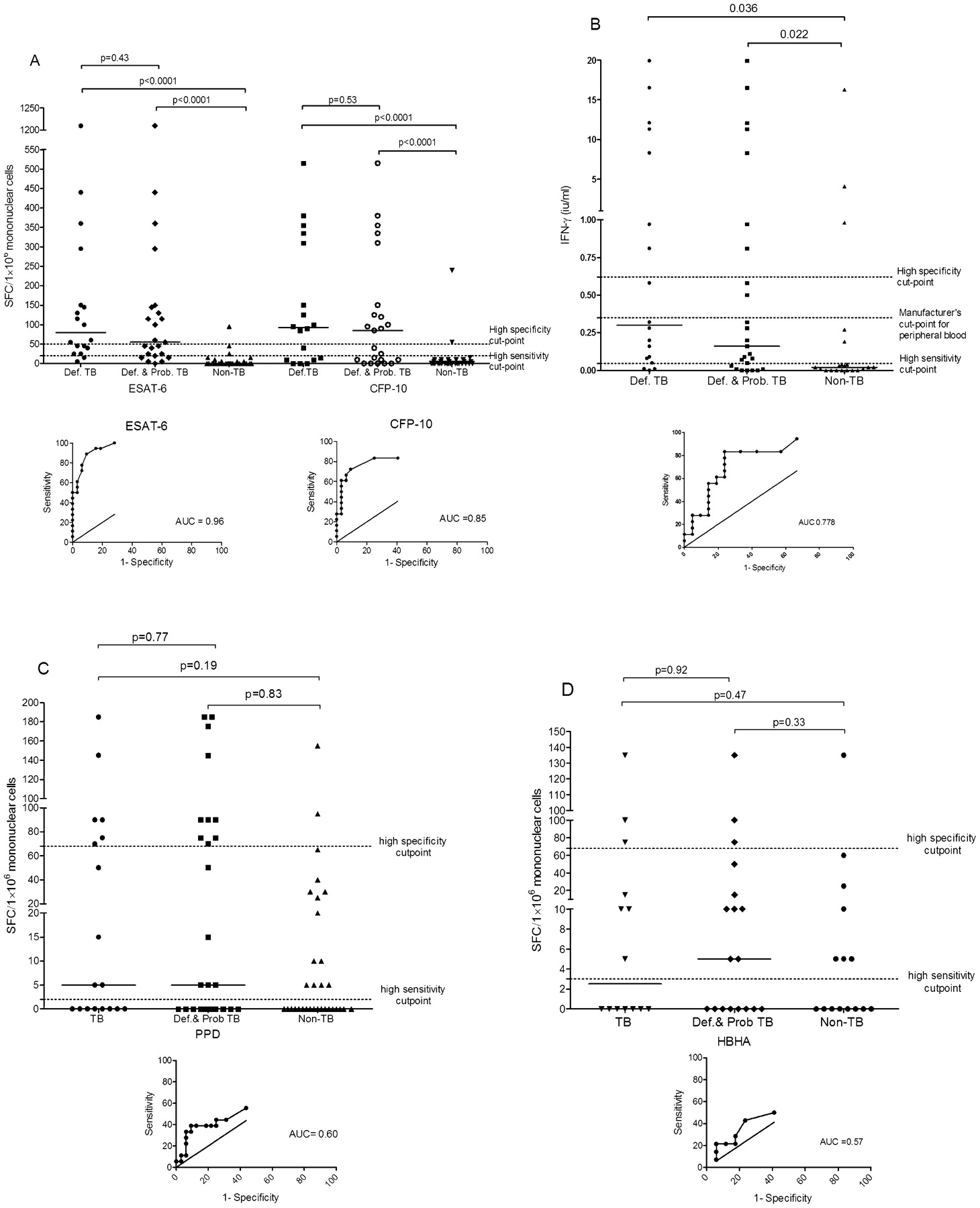
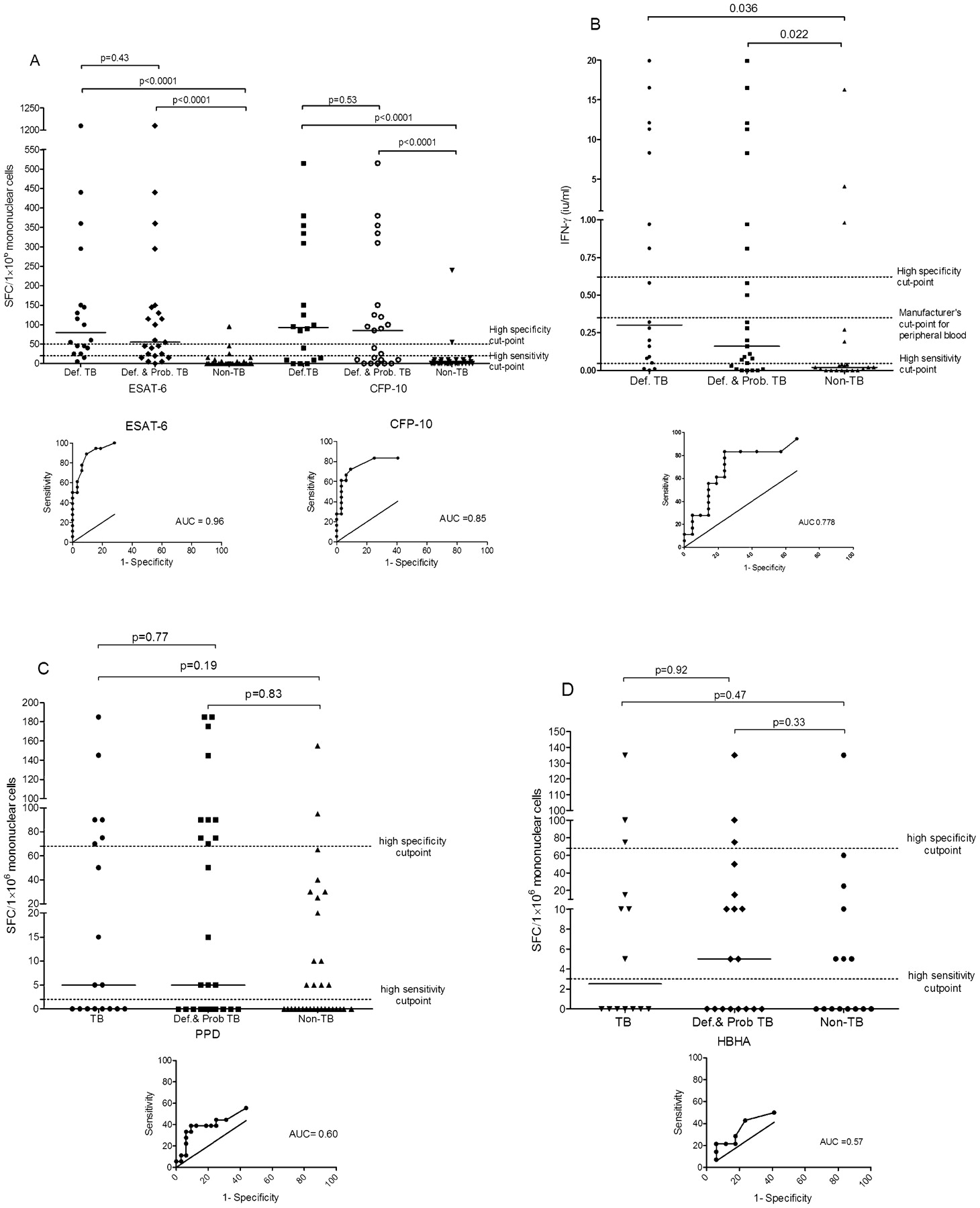
The assay-specific (QFT-GIT and T-SPOT.TB) sensitivity, specificity, negative and positive predictive values, and area under the receiver operating characteristic (ROC) of BAL samples are shown in table 3 (three cut-off points are shown: manufacturer-recommended for peripheral blood and two area under the curve (AUC)-derived cut-off points for optimal/high sensitivity and/or specificity). In evaluable samples, when the definite and non-TB groups were used for outcome analysis, the percentage sensitivity, specificity, positive predictive value and negative predictive value for T-SPOT.TB (⩾20 spots/million mononuclear cells) and QFT-GIT (0.35 IU/ml) were 89, 94, 89, 94% (n = 55) and 55, 86, 77 and 69% (n = 48), respectively. Rapid diagnosis of TB was achieved more frequently with T-SPOT.TB than with smear microscopy (14/24 (58%) vs 7/24(29%) of definite TB cases; p = 0.02). Also shown in table 3 are comparative values when peripheral blood RD-1 responses were evaluated. Outcome values for BAL and blood RD1 responses when the definite and probable TB groups were combined are shown in table E3 in the online data supplement. Scatter plots and AUC of the ROC of the RD-1 ELISPOT and ELISA BALMC IFNγ responses are shown fig 2A and B, respectively. There was moderate agreement between T-SPOT.TB and QFT-GIT (76% agreement, κ = 0.47, p = 0.001).
{kind=link}
{kind=link}
Scatter plots of alveolar lavage mononuclear cell RD-1-driven ELISPOT (T-SPOT.TB (A) ELISA (QuantiFERON-TB Gold-In-Tube) responses (B), purified protein derivative (PPD)-driven ELISPOT responses (C) and heparin-binding haemagglutinin (HBHA)-driven ELISPOT responses (D) in the tuberculosis (TB), combination of definite (Def.) and probable (Prob.) TB, and non-TB groups, respectively. Area under the curve (AUC)-derived cut-off points favouring a high sensitivity or specificity are shown. The AUC receiver operating characteristic (ROC) for each antigen used in the ELISPOT assay and for the ELISA (QuantiFERON-TB Gold-In-Tube) assay is depicted below each graph. SFC, spot-forming cell.
Performance outcomes (95% CI) of IRGAs (T-SPOT.TB, QFT-GIT) using alveolar lavage cells and whole blood, at different cut-off points, in patients suspected of having pulmonary TB (definite TB (n = 24) and non-TB groups (n = 48) used in the analysis).
Clinical details and laboratory results of non-TB patients with a positive BAL T-SPOT.TB or QFT-GIT are shown in table E4, whilst clinical details and laboratory results of all definite and probable TB patients with a negative BAL T-SPOT.TB or QFT-GIT are shown in table E5 (online data supplement). In an attempt to improve the discriminatory value of the ELISPOT assay we compared the IFNγ BALMC/PBMC ratio in the TB and non-TB groups. We hypothesised that patients with TB would have a higher proportion of antigen-specific lymphocytes at the site of disease. Whilst this ratio had a high diagnostic accuracy (AUC = 0.87; 93% sensitivity and 71% specificity at a cut-off point of >0.092; fig E4, online data supplement) it was no better than the BAL ELISPOT alone. HIV status did not impact on RD-1 ELISPOT or ELISA assay outcomes (see online data supplement; fig E5).
PPD and HBHA ELISPOT assay
Sensitivities and specificity of the BAL and blood PPD- and HBHA-driven ELISPOT assay using the definite and non-TB groups, and when definite and probable TB groups were combined, and depending on the cut-off point used, are shown in tables E6 and E7 (online data supplement). Outcome values when the definite and probable TB groups were combined are shown in table E4 (online data supplement). Scatter plots and AUC of the ROC of the PPD- and HBHA-driven ELISPOT BALMC IFNγ responses are shown fig 2C and D, respectively.
Discussion
There are limited data about the profile of alveolar TB antigen-specific (ESAT-6, CFP-10, TB 7.7 and HBHA) immune responses,7 8 15 16 and the utility and feasibility of a lung-orientated immunological approach for the rapid diagnosis of TB requires clarification. To our knowledge this is the first comparative diagnostic study of standardised antigen-specific (ESAT-6, CFP-10, TB 7.7 and HBHA) and non-specific (PPD) pulmonary lymphocyte responses. We found that although the ELISPOT assay was inconclusive in almost a third of cases, when an evaluable result was generated, it had a high sensitivity and specificity. Moreover, TB was rapidly diagnosed more frequently by the ELISPOT assay than by smear microscopy.
Although the specificity of the RD-1 ELISPOT assay was high (94% at a cut-off point of ⩾20 spot-forming cells (SFCs)/106 BALMCs) the sensitivity in the definite TB group was 88%. The only published study examining pulmonary RD-1 responses using the T-SPOT.TB assay found a sensitivity of 100% using a cut-off point of ⩾30 spots per million BALMCs.16 However, this preliminary study had a small sample size (n = 8 definite and n = 4 probable TB) and was performed in a setting of low TB and HIV prevalence. Factors such as a larger sample size, HIV co-infection (though we found no difference when results were stratified by HIV status), host human leucocyte antigen (HLA) phenotype, strain differences, immunosuppressive cytokines (eg, interleukin-10 and transforming growth factor β23), immunoregulatory T cells,24 bronchoscopic technique and our propensity to treat empirically for TB may have all contributed to the greater variability in sensitivity in our study. In keeping with our observations, a recent study, using flow cytometry, showed that 19% of definite TB cases had no measurable ESAT-6 protein-specific lung immune responses.8 There were 5 out of 48 non-TB patients (2 with lung carcinoma and 2 HIV positive) in whom the BAL ELISPOT IGRAs were positive. Although the relationship between lung cancer and TB is well described,25 and we cannot be certain that concomitant TB was not present, on follow-up we found no evidence of TB. Other possible explanations include transient or latent infection.
Test outcomes were poorer for the QFT-GIT assay despite using 1×106 cells per tube. The reasons for this are unclear. Varying the cut-off point or the volume of medium in the QFT-GIT tube did not meaningfully improve results. We therefore presume that performance was poorer because the ELISA is inherently a less sensitive immunological technique. We cannot exclude the possibility that the QFT-GIT-specific antigen, TB 7.7, may be driving inhibitory pathways or immunosuppressive regulatory T cells.24
A major practical limitation of the BAL assays was the high proportion of inconclusive results (34–41%). The most common cause was a non-functional positive control. There was no correlation with HIV status. Immunosuppressive cytokines23 26 27 or cells, including immunosuppressive pulmonary macrophages and regulatory T cells,24 may explain these findings. We estimate that if SEB was used as a positive control throughout the study then the proportion of inconclusive RD-1 ELISPOT results would have dropped from 34% to 25%. Further studies are now required to determine whether user-friendly depletion of immunosuppressive cells can further improve the performance outcome. This would make the assay clinically more useful. The second most common reason for inconclusive results was a high spot count in the negative control. Adjustment of the negative control ELISPOT cut-off point did not significantly improve outcomes without compromising sensitivity. Notably, 22% of the cohort had evidence of colonisation (positive bacterial or fungal culture in the absence of clinical disease), and high spot counts were significantly associated with HIV infection. Thus, although not proven, it is likely that airway pathogen colonisation, more common in high HIV and resource-poor settings, induces high spot counts in the T-SPOT.TB assay by activating the BAL alveolar T cells. Other reasons for inconclusive results were significant discoloration (blue-out) of the ELISPOT wells and low numbers of cells harvested at bronchoscopy, particularly in technically difficult procedures.
Interestingly, there were many non-TB patients with presumed latent TB infection (blood RD-1 IGRA positive) who were BAL RD-1 IGRA negative. How do we explain these findings given that the lung is a major site of latent infection? In contrast to the peripheral blood compartment, which contains circulating lymphocytes, the alveolar compartment may not reflect what is happening in the interstitial tissue (site of infection) or mediastinal lymph nodes where the majority of T cells reside. Compared with the RD-1 ELISPOT assay the specificity of the PPD assay was relatively poor. A likely reason is the high exposure to environmental mycobacteria in a resource-poor setting. It is therefore, similar to the findings in a recent UK-based study (76% specificity),8 not useful as a rule-in test in clinical practice. In contrast, the sensitivity of PPD in our study was surprisingly and inexplicably low.
HBHA, whose antigenicity is dependent on methylation of the C-terminal domain and is upregulated in murine lungs infected with M tuberculosis,20 is a novel and relatively TB-specific virulence factor.18 HBHA responses may be a sensitive marker of TB infection with the ability to distinguish latent from active TB.17 28 We therefore hypothesised that HBHA responses, which have not previously been evaluated using alveolar lavage cells, would be useful for the detection of pulmonary TB. However, HBHA, in both peripheral blood and BAL, had poor discriminatory value. The regulatory T cell profile, which may modulate HBHA responses,29 is likely to be different in high burden countries and may explain these findings. The differential effect of M smegmatis-19 20 21 vs M bovis BCG-derived HBHA on IFNγ responses, if any, is unclear.
We have taken several steps to limit study bias, including initial experiments to determine optimum cell number and antigen concentration, blinding an experienced laboratory scientist to clinical details, performing BAL in a standardised manner, recruiting consecutive patients suspected of having TB over a fixed time period and performing comparative analysis using several different antigens, assays and in both blood and BAL compartments. Nevertheless, the lack of association with HIV could be due to type 2 error. Larger studies are now required in different geographical settings to confirm these observations. Although the appropriateness of the ELISPOT assay in a resource-poor setting may be argued, it could have utility in diagnostically challenging cases in a tertiary care setting in South Africa.
In summary, when an evaluable result is obtained, the lung RD-1 ELISPOT response is a useful rapid immunodiagnostic test with a reasonably high sensitivity and specificity for pulmonary TB. However, clinical utility may be limited by the high number of inconclusive results. A lung-orientated approach to TB diagnosis is thus feasible, but further work is necessary, using alternative test formats, biomarkers and/or antigens, to develop an improved assay prototype that will minimize inconclusive results.
REFERENCES
Supplementary materials
Web only appendix for 64;10:847
Files in this Data Supplement:
Footnotes
Funding This work was supported by the South African National Research Foundation (SARChI), the South African Medical Research Council and the UCL–UCT Collaboration Initiative.
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
Ethics approval The study protocol was approved by the University of Cape Town Ethics Committee.
▸ Additional methods, figures and tables are published online only at http://thorax.bmj.com/content/vol64/issue10