Article Text

Abstract
The investigation and treatment of chronic cough in adults is generally rewarding, provided there is an understanding of its aetiology, particularly when it arises from sites outside the respiratory tract.
- cough
- adults
Statistics from Altmetric.com
Chronic cough is a common diagnostic and therapeutic problem. The exact prevalence has proved difficult to estimate and recurrent cough is reported by 3–40% of the population.1–,4 The results of questionnaire surveys such as these are clearly influenced by the population studied and the question posed. In a postal and telephone survey of over 11 000 patients from four general practices in south east England, cough was reported every day or on over half of the days of the year by 14% of men and 10% of women.2 A survey of 18 277 subjects aged 20–48 years from 16 countries worldwide reported nocturnal cough in 30%, productive cough in 10%, and non-productive cough in 10%.3 In this study the very high prevalence of nocturnal cough arose because a positive response to the question “Have you been woken by an attack of coughing at any time in the last 12 months?” was taken as indicating the symptom. However, since acute cough—by far the commonest symptom for which medical advice is sought5—could also lead to a positive response, significant nocturnal cough was probably overestimated in this study. Whatever the failings of individual surveys, chronic cough is clearly a very common symptom which, although associated with considerable morbidity, goes largely unheeded.
Unsurprisingly, cigarette smoking had a dose related influence on the prevalence of productive cough.3 In clinical practice, however, smokers readily ascribe their cough to tobacco and rarely seek medical advice specifically to combat this. As a consequence, the incidence of smoking related cough presenting as an isolated symptom in secondary care is low.2 The reasons why patients seek advice regarding chronic cough are not fully understood, but may be related to worry about the cough.6 Often, cough related morbidity—in terms of sleep disturbance (either of the patient or their relatives), urinary incontinence in women, or syncope—drives the patient to consult.6–,8 Indeed, chronic cough has been shown to be associated with a marked deterioration in quality of life which returns to normal on successful treatment.7–,9
In population surveys, men have reported cough more frequently.2,10,11 However, most patients referred to specialist cough clinics are women (table 1⇓). This paradox may be explained by differences in smoking habit, but women also appear to have an intrinsically heightened cough response. Inhalation cough challenge is augmented in both healthy female volunteers12–,16 and female patients with chronic cough.17 A higher frequency of ACE inhibitor induced cough18 is also found in women, suggesting that any sex related difference is unlikely to be due to augmented deposition of tussive stimuli in women. A hormonal influence is inferred by the observation that cough reflex sensitivity is similar in boys and girls,19 but the reason for the marked sex difference in adults remains obscure.
Most common causes of chronic cough in patients investigated in specialist clinics
Duration is important in determining the possible aetiology of cough. Classically, cough lasting less than 3 weeks has been considered as acute and that of more than 3 weeks duration has been defined as chronic.20 In recent years there has been a tendency to redefine chronic cough as cough lasting more than 8 weeks and, for further clarification, the term “subacute cough” was proposed to describe cough lasting 3–8 weeks.21 While these definitions remain arbitrary, the concept of chronic cough remains clinically important. In this review we will describe the assessment and management of patients with chronic cough.
CLINICAL EXPERIENCE OF CHRONIC COUGH
Chronic cough has frequently been considered to be an intractable problem. Such despondency, however, is not supported by the experience of specialist cough clinics. In these tertiary referral centres, which presumably concentrate on the most difficult diagnostic problems, an accurate diagnosis leading to effective treatment is achieved in over 80% of patients. This contrasts markedly with the experience in non-specialist clinics.22 The main reason for this difference is a failure to consider the potential origin of cough as being outside the lower respiratory tract. Because cough may arise from anywhere in the distribution of the vagus, the full assessment of the patient with chronic cough relies on a multidisciplinary approach and close cooperation between gastroenterology and ENT departments, as well as respiratory medicine. If this approach is adopted, only a small number of patients with idiopathic cough remain in whom no diagnosis is determined.
SYSTEMATIC ASSESSMENT OF COUGH
Twenty years ago Irwin and colleagues suggested that the investigation of patients with chronic cough could be based on an “anatomical diagnostic protocol” and that, if such an approach was used, “the outcome of specific therapy, almost without exception, is successful and sustained”.23 Our knowledge of the anatomical and cellular basis for cough receptor stimulation has evolved since that time, both in terms of conditions known to cause cough and the mechanisms whereby the cough reflex is stimulated in disease. However, the concept of a logical diagnostic pathway leading to successful specific treatment remains the basis of the organisation of the specialist cough clinics reported in the literature. In the absence of such an approach, the diagnostic yield and outcome of treatment is poor.22,24
Limited experience from general practice suggests that over 90% of patients with chronic cough, who represented approximately 6% of all new referrals, had their cough attributed to either bronchial hyperresponsiveness or upper airway disease.25 In contrast, a survey from a general respiratory clinic revealed that over half the patients with cough had underlying lung disorders such as chronic obstructive pulmonary disease (COPD), bronchiectasis, pulmonary fibrosis, or lung cancer.22 Thus, when examining the evidence obtained from tertiary referral clinics, it is important to realise that many of the common respiratory disorders associated with chronic cough have been excluded by the referral pattern. The spectrum of patients described below does not represent the total population with chronic cough, and conditions such as bronchiectasis and lung cancer are underrepresented. This observation may also go some way to explain the large variation in the reported incidence of the three common syndromes associated with chronic cough (asthma, gastro-oesophageal reflux, and rhinitis; table 1⇑).
Methodological differences in how a diagnosis is accepted as the cause of cough are also likely to be important. In the study by Palombini et al26 patients underwent more than 12 different diagnostic procedures and were considered to be positive for a diagnosis if a test result was abnormal. Unsurprisingly, this approach led to the claim that multiple causes of cough could be identified in over 60% of patients. Even when the investigation is tailored to the presenting symptoms, multiple diagnoses are made. For example, Irwin et al27 reported multiple aetiology for cough in a quarter of his patients. The more conservative approach of determining diagnosis, adopted particularly in European centres, has shown that in 89–100% of patients a single cause of chronic cough can be established.22,28–,30 However, a concomitant increase has been observed in the number of patients with idiopathic cough. Whereas Irwin et al23,27 and Palombini et al26 came to a diagnosis in all but one of 249 unselected patients, firstly Poe et al31 and subsequently several other groups28,32 have failed to achieve such diagnostic excellence, even when the anatomical diagnostic protocol was rigorously followed.
O’Connell et al30 were the first to suggest that a different approach based on the empirical treatment of cough could lead to an improved diagnostic yield. In this study patients were allotted treatment when intensive investigations had failed to provide a diagnosis. The finding that a number of patients did not achieve a primary diagnosis is perhaps unsurprising in the knowledge that more recent studies have described previously unrecognised causes of chronic cough such as eosinophilic bronchitis,29 eosinophilic tracheobronchitis,33 and oesophageal dysmotility.34–,36 The plan of investigation used at that time would not have been capable of picking up these newly discovered associations and it is likely that those patients currently classed as having idiopathic cough will have as yet undiscovered syndromes.
Several investigators have attempted to enhance diagnosis with the evaluation of upper airway inflammation,37 the analysis of induced sputum for cytokines, interleukins or TNF-alpha,38 and the measurements of exhaled nitric oxide levels.39 These efforts have, however, met with limited success. Conversely, it is possible that a simplified approach with a therapeutic trial as the main diagnostic arm of a cough clinic protocol may be successful. This strategy could be used earlier to provide a diagnosis without the need for specialised investigations. The approach of symptom led therapeutic trials requires a thorough knowledge of the likely aetiology and incidence of the various cough syndromes.
CHRONIC COUGH SYNDROMES
There are three common causes of chronic cough: asthma, oesophageal disease, and rhinitis. This “diagnostic triad”26 contains the overwhelming majority of patients who suffer from chronic cough.
Asthma related syndromes
The diagnosis of asthma as provided in the UK guidelines relies on the evidence of variability of airflow obstruction, either spontaneous or pharmacologically induced.40,41 However, the US National Institutes of Health definition42 states that asthma is “a clinical syndrome characterised by increased responsiveness of the tracheobronchial tree to a variety of stimuli”. This latter definition allows for asthma without airflow obstruction such as that which occurs in cough variant or, more accurately, cough predominant asthma. Our concentration on measures of variable airflow obstruction in the diagnosis of adult asthma has been led by practice in clinical trial design.43 Here reversibility to salbutamol or diurnal variation in peak expiratory flow are almost universally used as entry criteria to establish the diagnosis. Reversibility to β agonists is very good for proving that patients have asthma but is not reflected in the generality of asthma patients. Indeed, less than 10% of an asthmatic population may exhibit spirometric reversibility sufficient to satisfy the entry criteria for most clinical studies of asthma.44
The problematic nature of defining asthma in epidemiology has been extensively discussed45 and it is clear that no single test has sufficient sensitivity and specificity to diagnose reliably a syndrome with such protean manifestations.46 This is particularly relevant when cough is the primary presenting complaint. The term “variant asthma” or “cough variant asthma” to describe asthma associated with cough was originally introduced by Glauser.47 This entity was more clearly defined in 1979 by Corrao and colleagues who described six patients with chronic cough, bronchial hyperresponsiveness, and a response to anti-asthma medication but without wheezing and airflow obstruction.48 Subsequently, the term “cough predominant asthma” was proposed by Pratter and colleagues49 based on the suggestion that cough is not a separate entity but part of the spectrum of asthma together with dyspnoea and airflow obstruction. In our experience, this term more accurately describes the patients seen in clinical practice.
Niimi et al50 demonstrated the presence of eosinophilic inflammation in cough predominant asthma and a further variant, eosinophilic bronchitis, is characterised by airway eosinophilia but without bronchial hyperresponsiveness. Originally described by Gibson and colleagues,51 eosinophilic bronchitis may be detected in patients with chronic cough where reliable sputum induction and analysis is available.29,37 Whether cough with sputum eosinophilia but without airflow reversibility or hyperresponsiveness is a form of asthma remains debatable. The different facets of the syndrome may be due to the differential location of inflammatory cells, particularly mast cells, within the airway.52,53 However the terms “eosinophilic bronchitis” and “cough predominant asthma” appear to be clinically useful (table 2⇓).
Corticosteroid responsive cough syndromes
All of these facets of the “cough/asthma syndrome” usually improve with inhaled corticosteroids. The early symptomatic response to inhaled corticosteroids in “classical asthma” may be delayed in chronic asthmatic cough.29,54 Similarly, in eosinophilic bronchitis significant improvements in cough threshold and sputum eosinophilia have been observed after 4 weeks of treatment with budesonide.55 However, treatment may be required for several months before maximum improvement is observed. In this regard, cough may be similar to the slow improvement in airway hyperresponsiveness seen with inhaled corticosteroids in “classical asthma”.56 This phenomenon of a delayed response is also true of treatment for the other cough syndromes.
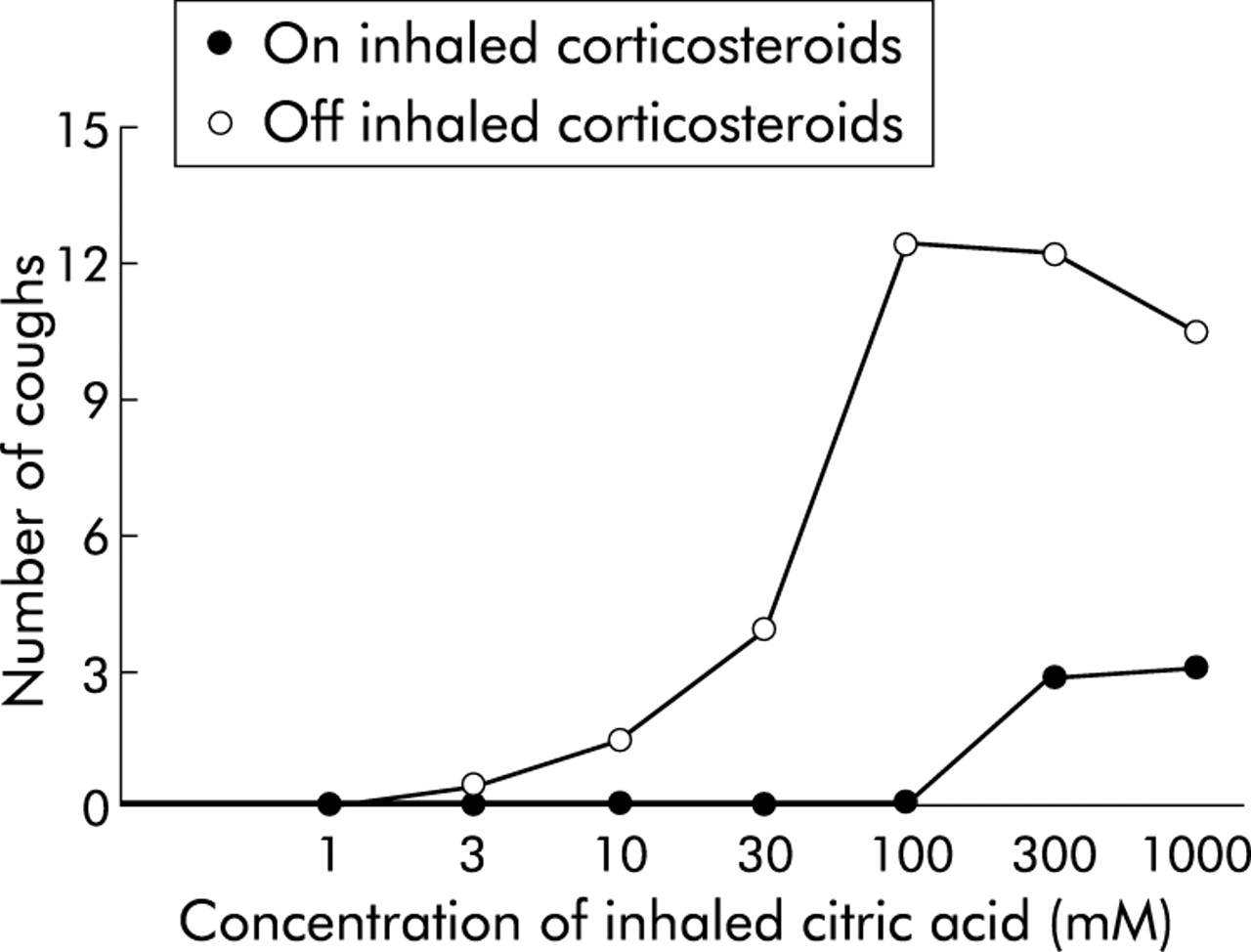
Patients with possible asthmatic cough presenting to secondary care (in the UK) are almost invariably on inhaled corticosteroids, and a poor response may indicate the usual problems with asthma therapy. Everard’s “three Cs”57 of competence, contrivance and compliance should be applied. An initial trial of prednisolone may be helpful.58 Since bronchoconstriction is not usually a major feature, an alternative diagnostic strategy is to stop inhaled corticosteroids. A progressive worsening of cough, with or without deterioration in peak expiratory flow, confirms the diagnosis. This also allows sputum examination since even moderate doses of inhaled corticosteroids cause a dramatic fall in the sputum eosinophil count.59 The subsequent symptomatic improvement on reinstitution of treatment reinforces the diagnosis and is associated with an improvement in cough sensitivity (fig 1⇓).

Improvement in cough reflex sensitivity measured by citric acid cough challenge in response to inhaled corticosteroids in a patient with cough variant asthma.
In patients who remain symptomatic on moderate doses of inhaled corticosteroids there is no clear evidence based strategy. Two recent studies reported on the effects of leukotriene receptor antagonists on the cough reflex.60,61 While zafirlukast had no effect on the normal cough response in classic asthma,60 it showed marked antitussive effects in patients with cough predominant asthma.61 The fact that lipoxygenase products have been shown to have a major modulatory role on the putative VR1 cough receptor62 may indicate a specific role for these agents in asthmatic cough. Fujimura et al33,63,64 have also described a response to antihistamines in a syndrome they termed eosinophilic tracheobronchitis or “atopic cough”.
As in all the conditions illustrated in table 2⇑ cough improves with corticosteroids, the term “corticosteroid responsive cough” as used by Gibson and colleagues in the original paper describing eosinophilic bronchitis51 may provide a convenient simplification. However, it is important to realise that non-asthmatic cough could be steroid responsive, both in rhinitis and in gastro-oesophageal reflux (GOR). An increased eosinophil count can be seen in the bronchoalveolar lavage fluid of patients with GOR related cough65 and airway inflammation is unsurprisingly seen in patients with reflux. This latter may be confirmed on direct examination of the endolarynx (fig 2⇓). Thus, in patients with laryngopharyngeal reflux, erythema or, more commonly, oedema of the arytenoid, interarytenoid area, and laryngeal surface of the epiglottis is present, together with oedema of the vocal cords and Reinke’s space (lamina propria of the true vocal cords).66,67 These changes may lead to a characteristic obliteration of the ventricle, the groove between the true and false vocal cords.

{kind=link}
{kind=link}
Oedema of the vocal cords, ventricles, and posterior commissurae seen during bronchoscopy in a patient with gastro-oesophageal reflux related chronic cough.
Chronic cough associated with gastro-oesophageal disorders
Gastro-oesophageal disease has been reported in 10–40% of patients with chronic cough. The pathophysiological mechanisms underlying this type of cough are not fully understood, but may include microaspiration of oesophageal contents into the larynx and tracheobronchial tree68 or local irritation of cough receptors within the lower oesophagus.69,70 It has been reported that 75% of patients with oesophageal cough have cough as the sole presenting symptom.69,71 However, we suggest that a careful clinical history focused on assessment of reflux symptoms such as heartburn, dysphagia, dysphonia, globus, acid regurgitation, and a bitter taste in the mouth is helpful. An association of cough with food—either eating certain types of food or the act of eating itself via the pharyngo-oesphageal reflex—is typical.72 Cough which is precipitated by adopting an upright posture is characteristic of reflux since it is accompanied by relaxation of the lower oesophageal sphincter.73 This history may be elicited by asking the patient when they start coughing in the morning at first waking, as Sir John Floyer observed in asthma,74 or on rising, typically to go to the bathroom.
An objective measurement of reflux using ambulatory oesophageal 24 hour pH monitoring is required in a proportion of patients in whom no diagnostic clues can be obtained from the history. Not all patients who have positive 24 hour pH monitoring respond to antireflux therapy and, similarly, a negative study does not preclude a therapeutic response.75–,78 An empirical trial with antireflux therapy has therefore been advocated.21,79 As in asthmatic cough, response may be delayed and treatment for at least 2 months with a high dose of a proton pump inhibitor may be required.
The gastroenterological definition of abnormality on 24 hour pH monitoring relies on a synthesis of the total number of reflux events, the fraction of time when pH <4, the number of events of pH <4 lasting longer than 4 minutes, and the longest upright and supine reflux events.80,81 In cough, however, such criteria may be irrelevant because even the briefest reflux event reaching the larynx could give rise to cough. Using the conventional parameters of abnormal oesophageal acidification, false negatives occur in a proportion of patients.69 Indeed, in some patients with reflux disease fundoplication is successful despite failure with intensive acid suppression,82 indicating that mediators other than acid in the refluxate may be important in cough.
In chronic cough the temporal association with reflux is also relevant. The number of coughs induced by a reflux event—that is, occurring simultaneously with or shortly after a fall in pH—should be measured.69,71,83 In an elegant experiment Ing et al70 demonstrated this effect by infusion of acid into the lower oesophagus. In a proportion of patients, however, cough can also be induced by intra-oesophageal infusion of 0.9% saline.69,70 This supports the hypothesis that cough may be induced not only by acidification, but also by other stimuli. Abnormal oesophageal manometry such as low gastro-oesophageal sphincter pressure leading to volume reflux and disordered oesophageal peristalsis also contribute in patients with chronic cough.34–,36 It is possible that the role of non-acid reflux may be further clarified by measuring oesophageal impedance.84,85
Chronic cough associated with gastro-oesophageal disorders frequently improves with antireflux therapy.69,71 Conservative measures such as weight reduction, high protein low fat diet, elevation of the head of the bed, and lifestyle modification including avoidance of caffeine, smoking, and chocolate are often recommended, although the basis for this advice is unclear. H2 antagonists,23,27,71 proton pump inhibitors,30,32,76 and prokinetic medication23,27,86 have been used, but proton pump inhibitors—particularly at high doses—seem superior in treating cough.49,79 In patients with abnormal oesophageal manometry but normal 24 hour pH monitoring, proton pump inhibitors also appear effective.36
The three placebo controlled trials reported to date have confirmed that both H2 antagonists and proton pump inhibitors correct chronic cough in patients with gastro-oesophageal reflux.75,77,78 These studies reported a relatively slow response in cough, ranging from 8 to 12 weeks. Occasionally, however, 6 months or longer may be required for the cough to improve.23,27 Unfortunately, antireflux agents do not fully suppress acid secretion and do not alter the frequency of reflux events.82,87 Antireflux surgery such as fundoplication may be successful in the face of an inadequate medical response.82,88 However, the role of surgery has yet to be fully evaluated.
Rhinitis, sinusitis, and postnasal drip
In contrast to the relative precision with which the asthma syndromes and oesophageal cough can be investigated, the association of chronic cough with upper airway disease frequently lacks objective verification. Many series, mainly from the US literature, report that postnasal drip syndrome (PNDS) is one of the most common causes of chronic cough.26–27,49,86 However, this term describes a symptom complex that does not have any objective or pathognomonic findings.20 The diagnosis of PNDS rests on eliciting symptoms that include the sensation of “something dripping into the throat”, frequent throat clearing, nasal congestion or discharge.23,27 Such symptoms are common in non-coughing individuals and vary enormously in different societies. A large telephone survey of cold symptomatology found that over 50% of subjects contacted in the USA associated a cold with PNDS, whereas less than a quarter in the UK and virtually no respondents from Latin America and India admitted to the symptom (Dr Hull, Procter & Gamble, personal communication).
Rhinitis is a much simpler term describing the location of airway inflammation. Sinusitis is present clinically when there is facial pain and may be associated with mucosal thickening, opacification of a sinus or an air-fluid level, and response to antibiotics.28,30 Sinus imaging has been suggested to support the diagnosis.32,37,86 However, in the context of chronic cough, sinus imaging appears to be unhelpful and of low predictive value.32,89
The common use of the term PNDS in cough has been led by clinicians who have observed that combinations of antihistamines and decongestants are effective in treating some patients with chronic cough.23,27 Pratter et al,49,89 using a stepped approach that involved the initial treatment of all patients with chronic cough with antihistamine decongestants, diagnosed PNDS in over 80% of cases. Some of these patients were asymptomatic apart from cough and they proposed the term “silent” postnasal drip syndrome since cough was the sole manifestation of PNDS. Obviously there are many more explanations for this therapeutic success than PNDS. However, these observations underscore the importance of histamine in chronic cough, either through a central activity90 or possibly due to its role in airway inflammation.91
A key question in cough associated with rhinitis is how the afferent sensory input generating the cough is developed. In animal studies no cough sensitive innervation can be seen above the larynx.92 Recently, based on the observation of a high frequency of asthma coexisting with allergic rhinitis, Grossman93 introduced a concept of “one airway, one disease”. Thus, upper and lower airway diseases are described as a continuum of inflammation involving one airway that may have a common origin for the underlying pathological process. In cough the coexistence of asthma and rhinitis has been reported for many years.23,27,94 Whether upper airway disease contributes to cough via PNDS or is merely a marker remains uncertain.32 Some support for the “one airway, one disease” concept in the pathophysiology of cough was provided by the response to histamine H1 antagonists and corticosteroids in patients with “atopic cough”.33,64 Better clarification of the description of rhinitis associated cough based on a scheme such as the ARIA guidelines95 needs to be developed.
OTHER CAUSES OF CHRONIC COUGH
Many other conditions can give rise to chronic cough. Typically, cough is the major component of a well recognised clinical syndrome such as chronic bronchitis, pulmonary fibrosis, or bronchiectasis. There are, however, a number of causes of cough which still provide diagnostic confusion.
ACE inhibitor cough
That a systemically active drug could cause cough as a side effect went unrecognised for many years.96,97 Cough associated with angiotensin converting enzyme (ACE) inhibition occurs in up to 15% of patients and has a very variable onset and offset.98,99 Because ACE inhibitors appear to alter the sensitivity of the cough reflex,100 underlying subclinical cough such as that from reflux may now declare itself. Cessation of treatment with ACE inhibitors returns the cough reflex to normal,30,98 but the plasticity of the reflex varies and it may take several months for the cough to settle in some individuals.101 Several small scale studies have reported a beneficial effect from a variety of agents in ACE inhibitor induced cough.102–,104 None have proved useful in clinical practice. The alteration in the sensitivity of the cough reflex precludes the full assessment of patients with cough while the patient remains on treatment. Indeed, alternative agents such as angiotensin II antagonists provide the beneficial effects of ACE inhibition without the tendency to cough.105
Occupational exposure
Cough may be an important symptom in a number of occupational lung diseases, particularly asthma. Cough as an isolated finding may occur following chronic exposure to low molecular weight irritants. In a glass bottle factory workers exposed to hydrochloric acid and organic oils developed chronic cough without airways hypersensitivity to methacholine. Cough reflex hypersensitivity was demonstrated by inhalation challenge with capsaicin and citric acid.106,107
Post infectious cough
Occasionally, patients give a striking history of prolonged cough following a relatively minor respiratory tract infection. If recurrent, then anatomical lesions such as bronchiectasis need to be excluded. Some agents such as Bordetella species are notorious for causing prolonged cough and recent studies have suggested that, in adults, infection and repeat infection are relatively common.108,109
CONCLUSION
The investigation and treatment of chronic cough is a rewarding and generally fruitful undertaking. By adopting an approach based on a careful history, simple investigations and therapeutic trials, dramatic improvements in quality of life can be achieved at little cost. The main reason for failure is a lack of understanding of the aetiology of cough, particularly when it arises from sites outside the respiratory tract.