Article Text

Abstract
BACKGROUND A randomised trial was performed on patients presenting to hospital with an exacerbation of chronic obstructive pulmonary disease (COPD) to compare outcomes in those managed at home with support with those admitted to hospital in the standard manner.
METHODS Over an 18 month period all patients presenting to the Royal Infirmary of Edinburgh on weekdays (n=718) with a diagnosis of an exacerbation of COPD were assessed for inclusion in the trial. Patients with impaired level of consciousness, acute confusion, acute changes on radiography, or an arterial pH of <7.35 or with other serious medical or social reasons for admission were excluded. Patients randomised to home support were discharged with an appropriate treatment package (antibiotics, corticosteroids, nebulised bronchodilators and, if necessary, home oxygen). They were visited by a nurse the following day and thereafter at intervals of 2–3 days until recovery when they were discharged from follow up. Parallel observations were made on patients allocated to normal hospital admission up to the point of discharge. Patients in both groups were assessed at home eight weeks after the initial assessment.
RESULTS Among weekday patients 353 (50%) were considered obligatory admissions, 140 (19%) were admitted because of co-morbidity, 17 (2%) because of poor social circumstances, and 24 (3%) did not consent to the trial. The remaining 184 (26%) were randomised (2:1) either to home support or to a standard hospital admission. The median time to discharge was 7 days for the home support group and 5 days for the admitted group (p<0.01); 25% of the home support group and 34% of the admitted group were readmitted before the final assessment at eight weeks (p>0.05). There were no significant differences between the groups in attendances by GPs and carers or in health status measured eight weeks after the initial assessment. Satisfaction with the service was good. The mean total health service cost per patient was estimated as £877 for the home support group and £1753 for the admitted group.
CONCLUSIONS This study shows that home supported discharge is a well tolerated, safe, and economic alternative to hospital admission for a proportion of patients referred to hospital for admission for an exacerbation of COPD.
- chronic obstructive pulmonary disease
- assisted discharge from hospital
- cost effectiveness
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a major cause of morbidity and mortality, placing large demands on both hospital and GP services. Exacerbations of COPD are one of the most common emergency admissions to hospital. Respiratory admissions constitute about 25% of medical emergency admissions in Scotland and COPD accounts for almost half of these.1 It has been estimated that inpatient costs for exacerbations account for 70% of the total health costs for COPD.2 Thus, any intervention that can reduce the number of admissions for exacerbations of COPD would be useful if it can be shown to be cost effective and not detrimental to patients.
Recently published British Thoracic Society guidelines for the management of COPD3 include criteria by which the severity and the appropriateness of admission for an exacerbation of COPD can be assessed, and suggest that there are a number of potentially avoidable admissions which could be managed at home if adequate support was provided.
To assess the potential for reducing emergency admissions for exacerbations of COPD we established an Acute Respiratory Assessment Service (ARAS) and undertook the first randomised trial to compare outcomes among patients presenting to hospital with an exacerbation of COPD between those managed at home with support and those admitted to hospital in the standard manner. The trial was conducted over an 18 month period; most of the patients were sent by their GPs but a few cases (1%) referred themselves for hospital admission with an acute exacerbation of COPD. A previously published study of domiciliary support for exacerbations of COPD was not a randomised controlled trial4 but related to a population of patients directly referred for advice concerning possible admission, and was therefore unable to make a valid comparison with outcomes for patients admitted to hospital. By contrast, our study was conducted in an unselected population of patients representing all patients referred to our hospital for admission with an exacerbation of COPD.
The study was designed to answer the following questions:
What proportion of patients can be safely managed at home?
Are there any differences in recovery in terms of readmission rates and quality of life measures between home supported patients and comparable patients admitted to hospital?
Is patient satisfaction with the home supported service as good as that for admitted patients?
Is a home supported discharge service economically viable?
Methods
The study was conducted in the Royal Infirmary of Edinburgh which has the only accident and emergency department (A&E) in Edinburgh. The admission pathway for respiratory patients to this hospital is that patients are referred largely by their GP or, in the case of a small proportion, by self-referral to the hospital. During the period of the study only 1% of patients with exacerbations of COPD self-referred. All of the patients are all seen initially by the staff in the A&E for immediate resuscitation or by the medical registrar on call and are either discharged home or, if admission is considered necessary, are moved to the medical admissions unit where they are all seen by the respiratory team on call and remain under their care thereafter, both in the admissions unit and later in the respiratory unit. Since there is no other admission pathway and the respiratory team see all respiratory admissions, we had information on all exacerbations of COPD presenting to the hospital over the study period.
The ARAS was available on weekdays from 09.00 hours to 17.00 hours so patients presenting overnight (after 17.00 hours) were assessed at 09.00 hours the following morning in the admissions unit. All patients presenting to the Royal Infirmary of Edinburgh between 17.00 hours on Sunday and 17.00 hours on Friday with a diagnosis of an exacerbation of COPD as the main reason for admission were assessed with respect to 13 indicators of severity of the exacerbation, as described in the British Thoracic Society guidelines for the management of COPD (table1).3 Patients with any of the following four indicators—impaired level of consciousness, acute confusion, acute changes on the radiograph, or an arterial pH of <7.35—were deemed obligatory admissions. A number of other patients were also judged obligatory for concomitant medical conditions or for social reasons. All remaining patients were considered potentially suitable for supported discharge.
Indicators of severity of exacerbation in COPD from BTS guidelines3
The purpose of the trial was explained to patients and their written consent obtained. An information sheet on the trial aims and protocol was sent to local GPs and their approval to include their patients was sought. Initial assessments including clinical history, spirometry, chest radiography, sputum culture, oxygen saturation breathing air and, if necessary, arterial blood gas tensions were performed by the ARAS nurses and reviewed by the respiratory on-call team (consultant and registrar) who made the final decision on inclusion in the trial. Those who had consented were randomised using a set of computer generated random numbers in a 2:1 ratio either to immediate supported discharge or admission to the respiratory medicine unit. A 2:1 randomisation was chosen to allow greater experience for the nursing staff of supported discharge. Randomisation occurred at the time when the patient reached the admissions unit and was assessed by the respiratory team on call.
Patients randomised to home support were discharged home with an appropriate treatment package arranged by the ARAS (antibiotics, corticosteroids, nebulised bronchodilators and, if necessary, an oxygen concentrator on loan). They were visited at home by an ARAS nurse the following day and thereafter at intervals of 2–3 days to monitor the need for treatment. The progress of the patients was assessed in consultation with the two ARAS nurses weekly at a review meeting by the consultant in charge of the trial (WMcN). Medical advice was available daily from the on call respiratory medical team (respiratory registrar and consultant) and changes in prescription could be obtained by consultation with the patient's GP. When patients were considered by the nursing staff to have recovered sufficiently no longer to require nursing support at home, they were discharged from the ARAS service and were left a short questionnaire on satisfaction with the service. Patients who were randomised to the inpatient (admission) limb of the trial were treated by the hospital team on the respiratory unit. In a similar way they were discharged when the medical team felt they had recovered sufficiently. The treatment offered at home and in hospital (oxygen, nebulisers, antibiotics, corticosteroids) was prescribed and reviewed according to BTS guidelines and clinical judgement.3
The patient's GP was informed immediately of his or her inclusion in the trial and kept informed of the patient's progress during follow up by the ARAS team and by letter at the time of discharge from ARAS/hospital. Eight weeks after the initial assessment all trial patients were assessed at home. Spirometric parameters were measured by the ARAS nurse, quality of life was assessed using the Chronic Respiratory Questionnaire,5 and patients were asked about any additional care they had received GPs, social work services, or informal carers since discharge from ARAS or from hospital. General practitioners were also asked about their satisfaction with the service by means of a short postal questionnaire.
ECONOMIC ANALYSIS
An economic evaluation was carried out by Dr Kathy McGregor of Lothian Health in relation to the financial year 1997–8. The cost of the ARAS care was calculated taking into account staffing, non-staffing, and drug costs in relation to number of days each patient remained under the care of the service. Inpatient costs were based on the length of hospital stay and average cost per bed-day in the respiratory unit. Detailed information on drug usage was extracted from case notes for a subset of patients admitted to hospital with an exacerbation of COPD and was included in average bed-day cost. Additional GP costs were calculated using unit costs estimated by the Personal and Social Services Research Unit, Kent.6
STATISTICAL ANALYSIS
Mann-Whitney and χ2 tests were used to compare the distributions of time to discharge and readmission rates of the two groups. Changes in respiratory function were evaluated using pairedt tests and comparison of these changes and of final quality of life scores between the groups were made using independent sample ttests.
Results
Between November 1996 and mid May 1998, excluding Christmas periods, there were 534 days of observation and 1024 patient referrals with an exacerbation of COPD. Eighteen patients were seen and discharged directly from A&E leaving 1006 patients who were assessed in the admissions unit (fig 1). Two hundred and eighty eight of these referrals (29%) were at weekends (17.00 hours on Friday until 17.00 hours on Sunday) and were not randomised. Among the remaining weekday referrals 353 (50%) were patients requiring obligatory admission according to the four criteria described above, most (n=253) because of a new abnormality on the chest radiograph, mainly signs of consolidation. A further 140 (19%) were admitted because of the co-existence of another medical condition (mainly cardiovascular, ischaemic cardiac pain, possible pulmonary thromboembolus, or cardiac failure) and 17 (2%) because of poor social circumstances which precluded home supported discharge; 24 (3%) did not consent to be involved in the trial. The remaining 184 (26%) were randomised in a ratio of 2:1 either to home support (n=122) or to a standard hospital admission (n=62). There were no statistically significant differences between these groups with regard to age, sex, smoking status, or home circumstances (table 2). In an analysis of 1002 patients in whom all of the severity indicators were recorded (four weekend patients did not have all indicators measured) respiratory function tests measured at the time of the exacerbation, including FEV1, respiratory rate, oxygen saturation, and arterial blood gas tensions (measured breathing air) were also similar in patients presenting on a weekday or at the weekend (table 3). A greater proportion of those presenting at the weekend were housebound (p<0.001) and more had worsening peripheral oedema (p<0.01) than those presenting during the week.
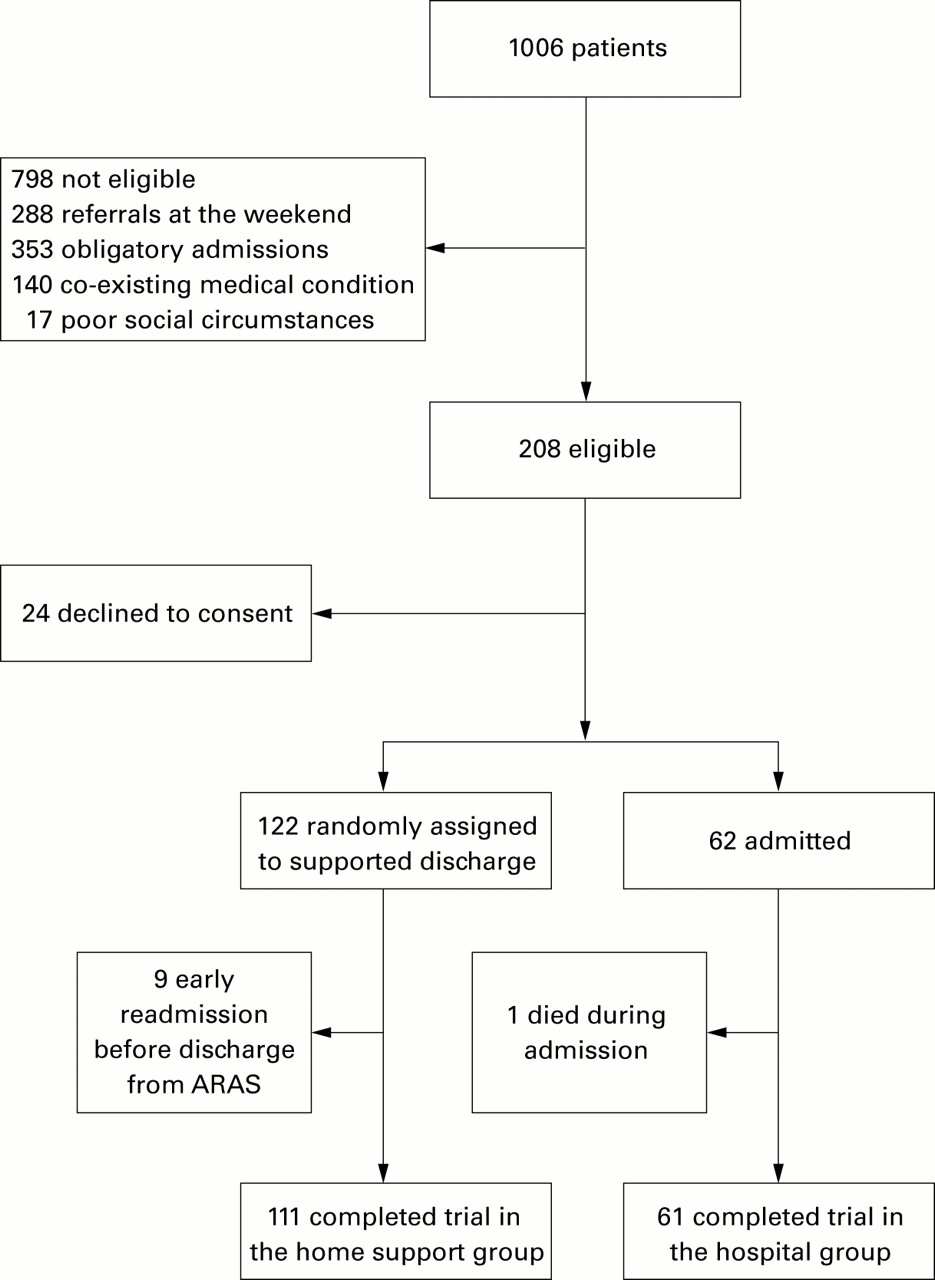
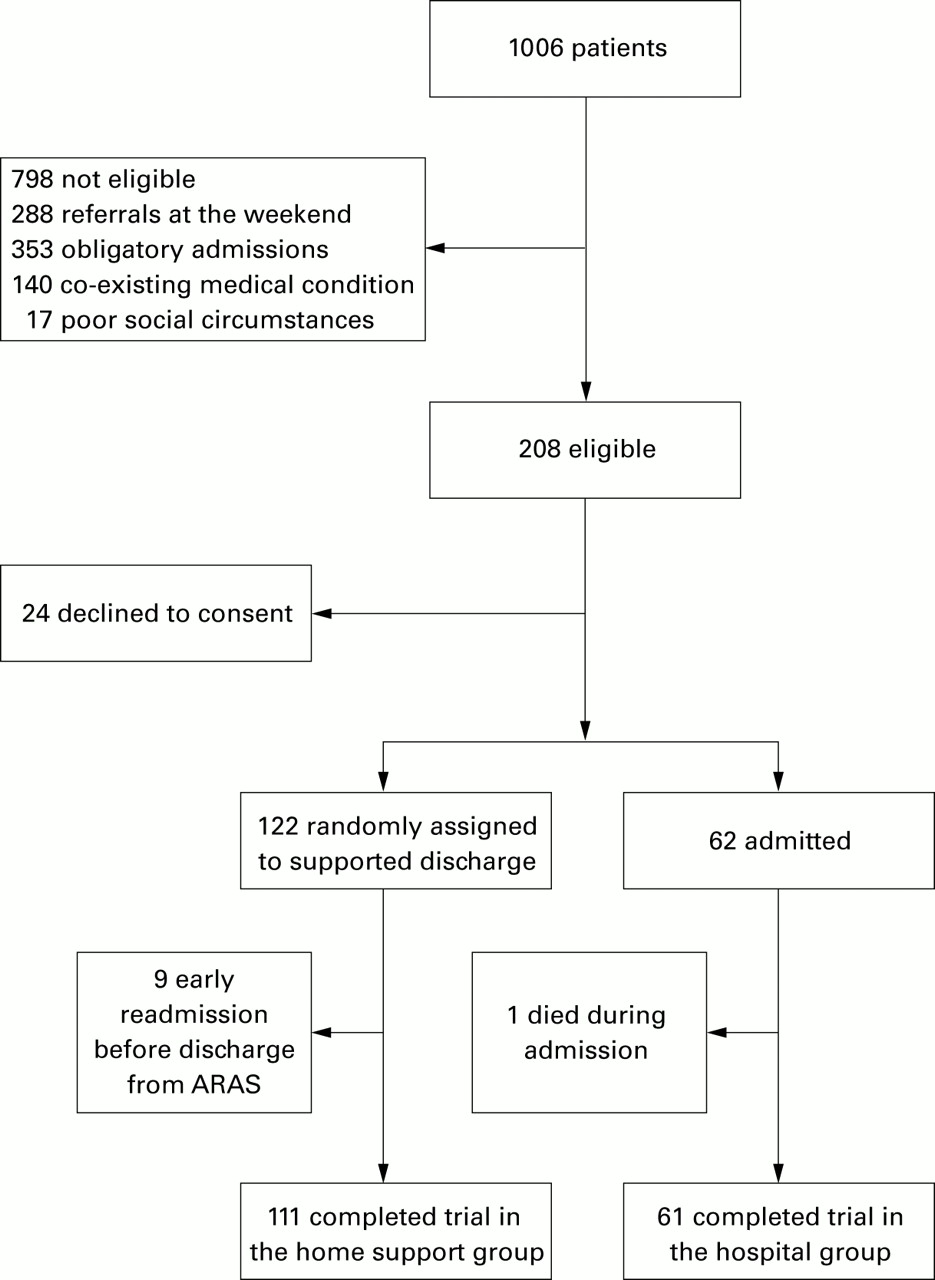{kind=link}
Trial profile.
Patient characteristics for the home support and admitted groups
Comparison of weekday and weekend exacerbations of COPD
Table 4 compares follow up and readmission in the two groups of patients; 7% of those supported at home were admitted to hospital for respiratory related problems before they were discharged from ARAS follow up, all of them on the advice of the visiting ARAS nurse. Among those discharged at the end of the exacerbation, 25% of the home support group and 34% of the hospital admitted group were readmitted before the final assessment at eight weeks (difference not significant). The median time to discharge was 7 days for the home support group and 5 days for the admitted group (p<0.01; table 5). Home support patients received an average of 3.8 visits at home from the ARAS nurses before being discharged. Attendance by GPs and carers did not differ significantly between the groups during the eight week follow up period (table 5).
Readmission rates
GP and nurse support
Both groups had better respiratory function at the time of discharge from home or hospital care than at the time of the initial referral, which were all significantly different except for the change in FEV1 in the admitted group. Between discharge and the final assessment at eight weeks measurements of respiratory function did not change significantly except for an increase in oxygen saturation of 2.4% in the admitted group (table 6).
Changes in respiratory test results
There were no significant differences between the groups on any dimension of the Chronic Respiratory Questionnaire (data not shown) when measured at the eight week follow up visit. Replies to the questionnaires on satisfaction with the service were received from 69% of patients treated at home, 95% of whom said they were “completely satisfied” with the service and 90% felt they had been cared for just as well or better at home than they would have been in hospital.
Fifty percent of GPs replied to the postal questionnaire. All of them were satisfied with the decision to provide domiciliary support and the information they received on the patient's progress; 65% of responding GPs felt that managing the patient at home by the ARAS did not increase the demands on their practice; 33 % reported decreased demands and only 2% reported increased demands.
The mean health service cost per patient was £877 for the home support group and £1753 for patients admitted to hospital. The mean cost of GP care between discharge and final assessment was slightly greater for the hospitalised patients than for ARAS patients.
Discussion
This study has shown for the first time in a randomised parallel group study that home supported discharge for a proportion of patients with exacerbations of COPD can provide an acceptable alternative to hospital admission. The study also provides information on the potential number of patients who are eligible and would benefit from this service. Our hospital serves a population of 400 000 and receives 14 000 medical admissions per year. The on call respiratory team undertake a twice daily ward round in the medical assessment unit and assess and provide continued care for all respiratory admissions to the hospital. Over the 18 month period of the trial there were 1006 admissions with a main diagnosis of an acute exacerbation of COPD, which represents 7.2% of acute medical admissions. About half the presenting patients were considered to be obligatory admissions based on the four criteria in the BTS guidelines. However, 19% were considered obligatory because of other concomitant medical conditions—mainly cardiovascular disease—and a small percentage were considered obligatory for social reasons. About 26% of weekday patients therefore were initially assessed as suitable for home supported discharge (excluding those who refused to enter the trial). However, 7% of ARAS patients required to be admitted before discharge from the home support service. Thus, using a more conservative estimate of 23% of patients eligible for the service, we would estimate that about 115 of 500 patients per year presenting on weekdays with exacerbations of COPD could be supported at home without admission. Patients admitted at weekends (17.00 hours on Friday until 17.00 hours on Sunday) were very similar to those who presented on weekdays in terms of the severity indicators suggested in the BTS guidelines, except that more of the weekend patients were housebound and more had worsening peripheral oedema. A full service available at all times would therefore be able to support about 150 out of 700 patients per year. In addition, there is potential for early supported discharge after admission of about 30 patients per year whose initial admission was considered obligatory.
Trial patients were randomised to home support or hospital admission in a ratio of 2:1. This gave a power of 80% to detect a difference of 20% in readmission rates following discharge (using a 5% significance level).
In both groups there was the potential to arrange for immediate unsupported discharge, but in practice this did not happen in either group. The groups were initially similar with respect to the indicators of severity of their exacerbations and remained similar in terms of their spirometric parameters at the final assessment eight weeks after the exacerbation.
The mean follow up time before discharge in the home support group was slightly longer than the length of hospital stay in the admitted group; this may have reflected the fact that the nurses' home visits were not always daily during follow up. The groups showed similar readmission rates between the time of discharge and the final assessment at eight weeks and had similar quality of life measures on the Chronic Respiratory Questionnaire. These data indicate that immediate or next day supported discharge is safe and does not compromise recovery in patients with mild/moderate exacerbations of COPD. Patient satisfaction with the home support service was excellent and most GPs indicated that no increased burden had been placed on their practice as a result of this service.
A recent report by Gravil and coworkers4 of a similar service also indicated the benefits of nurse-led home support for patients with exacerbations of COPD. There were, however, important differences between our study and that of Gravil and coworkers. Their patients had a mean FEV1 of 1.02 l compared with 0.74 l for patients in our study. Patients in our study were unselected before presenting to hospital for admission, selection for inclusion in the trial being on the basis of severity assessment in the hospital, but in the study by Gravil et al it was effectively GPs who selected which patients should be sent for assessment. Such a service may actually attract more patients than would have been the case had the service not been available. It appears that only selected patients who had less severe exacerbations were assessed. There was also no randomised comparison between admission and supported discharge in the study by Gravil and colleagues and therefore the true potential to prevent admissions could not be assessed.
In order to assess whether the introduction of our service had attracted more patients we compared the numbers of referrals to the hospital for admission with exacerbations of COPD during the last 12 months of the study with the number in the year before the service was in place. We found no major difference in the numbers of patients referred in the two periods. It is therefore unlikely that the establishment of our service attracted more referrals to the hospital for exacerbations of COPD than would otherwise have occurred. Few patients presenting with an exacerbation of COPD were sent home from the A&E department in either of these two periods.
The readmission rate during the eight weeks following discharge from either service was high, although it was lower for patients in the home care service. This is in line with a retrospective analysis which we conducted in Lothian in the year before this study which showed that exacerbations of COPD were the most common reason for readmission of patients in the 65–84 age range (unpublished data).
The calculated costs per patient in the two arms of the trial are not strictly comparable for several reasons. The existence of fixed costs means that average bed-day costs overstate the value of any potential savings resulting from a reduction in bed-days. However, even if only 50% of inpatient bed-day costs in the respiratory medicine unit of the Royal Infirmary of Edinburgh were included in the comparison, the ARAS would still represent an apparent cost saving (£877 versus £891). A better comparison would be to evaluate the use to which any freed resources in the hospital were put and attempt to estimate whether inpatients with COPD consume more or less resources than other respiratory patients in the same ward. There was no evidence to suggest increased costs of community services by the home supported patients, and in an ideal comparison a value would be placed on the increased satisfaction reported by these patients.
We believe that this study has shown that supported discharge is possible in patients with mild to moderate exacerbations of COPD. The study also indicates the potential numbers of patients who can be managed in this way and the resource implications for such a service. This should enable others to decide whether such a service should be established in their hospitals.
Footnotes
This study was supported by the Scottish Office and the Royal Infirmary of Edinburgh and Associated Hospitals Trust Endowments.