Article Text

Abstract
A 24 year old woman with airway injury, lung infiltration and pleural effusion due to pyoderma gangrenosum is reported.
- pyoderma gangrenosum
- pleural effusion
Statistics from Altmetric.com
Pyoderma gangrenosum is an unusual skin disease of unknown aetiology that is frequently diagnosed by its cutaneous appearance together with systemic involvement. Histological examination shows marked infiltration with neutrophils in the dermis.
Lung manifestations of pyoderma gangrenosum are rare. We report a case of pyoderma gangrenosum with a characteristic cutaneous appearance and extensive pulmonary lesions that improved dramatically with corticosteroid and immunosuppressive therapy.
Case report
A 24 year old woman was admitted in July 1996 with cough, fever, multiple nodules, and ulcerations over both legs that had been present for more than nine months. She had reported a dry cough and slight fever in October 1995, at which time several nodules had appeared on her abdomen and both legs. The nodules were about 2 cm in diameter and were tender. In January 1996 her temperature rose to 39°C from 37.5°C, the cough worsened, and shortness of breath developed. Biopsy specimens of the inguinal lymph node showed “fibrolipoma with infection”. Cefazolin was given for 20 days and her temperature fell to 38°C and the nodules disappeared, but her cough did not improve. In April 1996 a chest radiograph showed shadowing in the right upper lung with a right pleural effusion. A presumptive diagnosis of “tuberculous pleurisy” was made. She was treated with prednisone 10 mg tid, rifampicin, isoniazid and pyrazinamide for one week after which the effusion disappeared. The anti-tuberculosis drugs were then continued for four months.
Two months before readmission nodules with an erythematous halo recurred on her legs. Pustules then appeared on the nodules, the surface of most of the pustules became enlarged and the central overlying skin began to develop necrosis. The results of bone marrow aspiration, liver, and spleen punctures were all normal. On 2 July she had a haemoptysis of 100 ml. Her temperature ranged from 37.5°C to 38°C.
On admission her body temperature was 39.2°C, pulse rate was 100/min, respiratory rate 20/min, and blood pressure was 110/70 mm Hg. Multiple tender pustular and necrotic skin lesions were observed mainly on her legs. Some pustules exhibited central necrosis surrounded by an indurated erythematous halo. There were multiple extensive ulcerations of variable size (5–10 cm in diameter) which were covered with a necrotic and haemorrhagic material with a bluish undermined margin surrounded by an active zone of erythema (fig 1). There was dullness on percussion of the right lower lung. The cardiac rhythm was regular and no murmurs were audible. The liver and spleen were not palpable.

Multiple ulcerations on legs.
Peripheral blood examination showed WBC 12.9 × 109/l with a differential count of 88% granulocytes, 12% lymphocytes; Hb 130 g/l, and platelet count 382 × 109/l. Blood gas tensions were pH 7.436, Pao 2 77.9 mm Hg (10.39 kPa), Paco 2 36.7 mm Hg (4.89 kPa). Biochemical tests showed C reactive protein (CRP) 12.2 mg/dl (normal value <2.5 mg/dl); erythrocyte sedimentation rate 105 mm in first hour; protein electrophoresis: albumin 36.36% (range 54–74), α1 9.65% (1–3), α2 13.53 (6–9), β 14.52% (9–12), γ 25.94% (15–20); IgG 13.3 g/l (6.0–16.0), IgA 2.19 g/l (0.2–5.0), IgM 2.12 g/l (0.6–2.0). Urine and stool routine tests were all normal. The chest radiograph indicated patches in the right lower lung and a right pleural effusion (fig 2A). Thoracentesis revealed an exudate with a protein content of 24 g/l, glucose content of 29.1 mmol/l, and leucocyte counts of 680/μl with 60% neutrophils and 40% mononuclear cells. Repeated cultures for bacteria, mycobacteria, Nocardia and fungi from the skin specimens, blood, urine and sputum failed to reveal any infection.
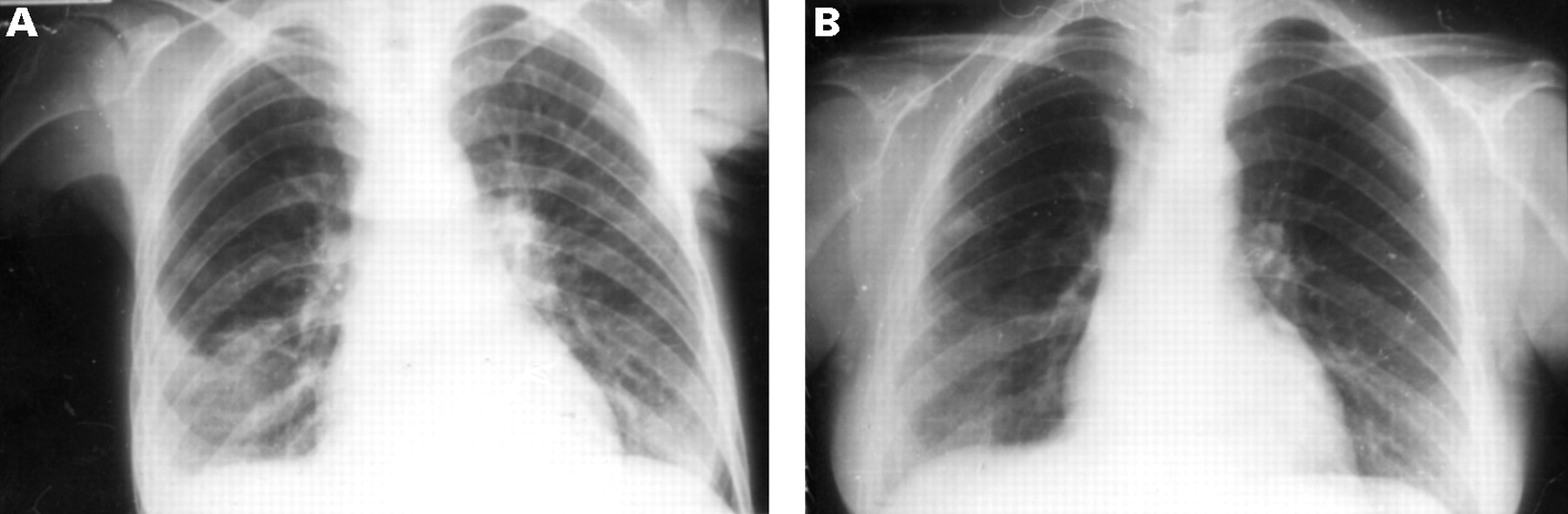
Chest radiographs (A) before admission showing disease in the right lung and right pleural effusion and (B) after four months of treatment showing minor residual infiltration on the right lung.
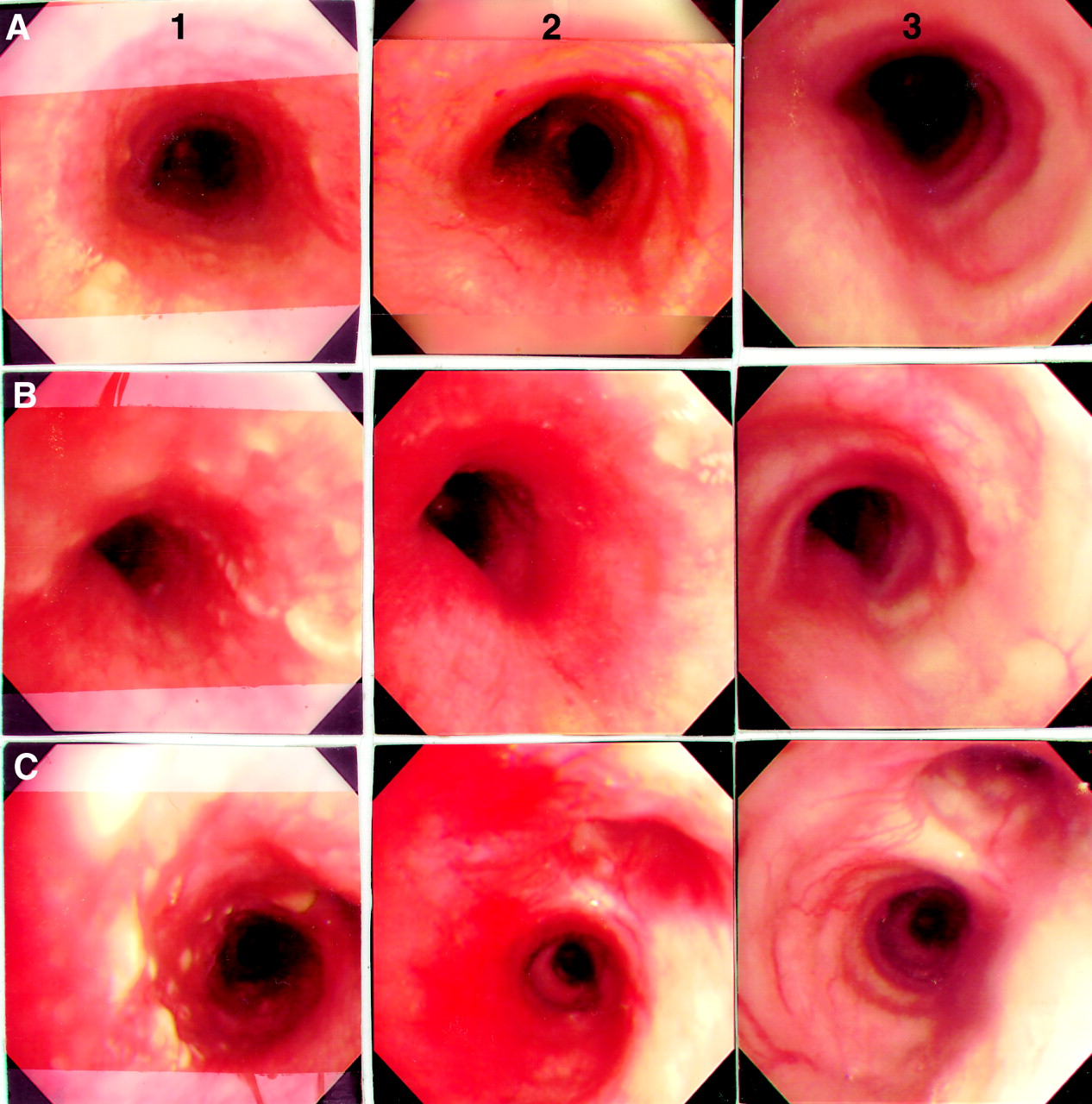
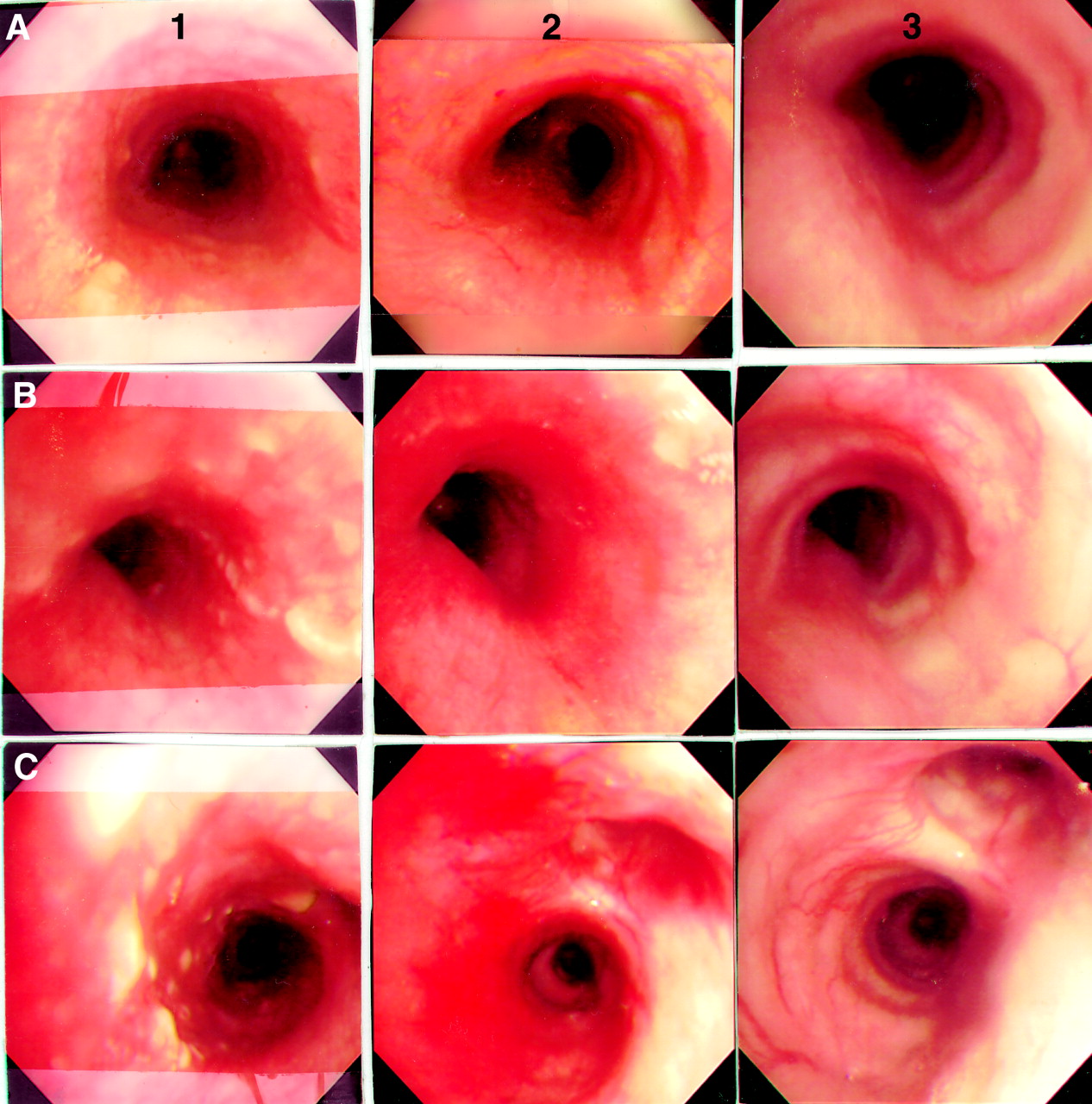
Fibreoptic bronchoscopic examination showed white and yellowish nodules (0.4–4 mm in diameter) spread diffusely on the trachea and the right and left bronchi with blood vessel engorgement (fig 3). Histopathological examination of the tracheal lesions showed infiltration with neutrophils and monocytes, while the skin ulcer lesions had marked infiltration with neutrophils, lymphocytes and histocytes; no vasculitic or granulomatous features were seen.
{kind=link}
{kind=link}
{kind=link}
Fibrobronchoscopic appearance of (A) the trachea, (B) the left bronchus, and (C) the right bronchus (1) before treatment with nodules widely spread in blood engorged airway mucosa, (2) after 10 days of treatment showing scattered nodules, and (3) after two months of treatment showing a normal appearance.
The patient was treated with antibiotics (cefaperazone, vancomycin), and anti-tuberculosis therapy was continued, but no improvement was seen. On the eighth day after admission these drugs were stopped and she was given intravenous hydrocortisone 300 mg/day and cyclophosphamide 200 mg three times a week. Her cutaneous lesions responded dramatically after 10 days, oral prednisone 80 mg/day was substituted for hydrocortisone and the cyclophosphamide was stopped after 20 days.
Ten days after initiation of corticosteroid therapy, a chest radiograph showed that the infiltration and effusion in the right lower zone had diminished and bronchoscopy showed that the nodules had almost disappeared with mucosal blood vessel engorgement (fig 3). After two months of treatment the bronchoscopic appearance was normal (fig 3). At discharge (four months after admission) the chest radiograph showed minor residual infiltrations (fig 2) and blood gas analysis was normal.
Discussion
The pathogenesis of pyoderma gangrenosum is still unclear but may involve a derangement in immunity and/or neutrophil function.1 Pyoderma gangrenosum is frequently associated with inflammatory bowel disease, autoimmune diseases, haematological disorders, and can be induced by trauma in some patients. Our patient had none of these illnesses.
We thought initially that the diagnosis might be an infectious process, particularly tuberculosis, in view of the systemic involvement and the limited response to antibiotic therapy before admission. However, the lack of a positive bacterial culture and lack of response to broad spectrum antibiotics or anti-tuberculosis drugs suggested pyoderma gangrenosum as a possible diagnosis. Pyoderma gangrenosum was diagnosed from the clinical and histological appearances of the skin and the pathology of the tracheal lesions. The good response to corticosteroid and immunosuppressive agents also suggested that the diagnosis was correct.
Although systemic involvement with pyoderma gangrenosum is very rare, previous reports have described changes in the lungs,2-7heart,8 liver, and pancreas.9 The main clinical manifestations in lungs included cavitation, pleural effusion,3 ,4 and infiltration.5-7 Lebbeet al 4 reported marked intra-alveolar neutrophilic infiltration in the lung in patients with pyoderma gangrenosum. Our patient is the first in whom airway injury, lung infiltration, and pleural effusion due to pyoderma gangrenosum has been reported. We found no evidence of any other systemic abnormality.
The main differential diagnosis of pyoderma gangrenosum is Wegener’s granulomatosis which can be associated with similar lesions and systemic involvement. It is characterised by classical clinicopathological features of necrotising granulomatous vasculitis. Almost all patients have lung involvement, and nodular lesions can occur with infiltration by inflammatory cells. Skin lesion characterised by vasculitis with or without granulomas are seen in 45% of patients. In some cases several ulcerative lesions, 1–5 cm in diameter, have been found with features like those of pyoderma gangrenosum.10 However, the absence of nasopharyngeal or renal lesions and the pathological findings of the tracheal and skin lesions ruled out Wegener’s granulomatosis in our case.
Some antimicrobial agents have been found to be useful in treating pyoderma gangrenosum—for example, sulpha drugs, colfazimine, minocycline, rifampicin, vancomycin and mezlocillin. Their mode of action is believed to depend on alteration of neutrophilic function or anti-inflammatory effects.1 However, in our patient rifampicin and vancomycin had no effect. Systemic corticosteroids are the most consistently successful drugs, particularly in treating the acute, rapidly progressive form of pyoderma gangrenosum. Alternatively, immunosuppressive agents such as cyclophosphamide can be added. Cyclosporin is one of the most promising immunosuppressants for treating pyoderma gangrenosum,1 in keeping with previous reports. Our patient achieved a dramatic response after treatment with hydrocortisone 300 mg/day and cyclophosphamide 200 mg three times per week for 10 days.
In conclusion, lung involvement is a rare feature of pyoderma gangrenosum and our report should raise awareness of the respiratory symptoms and signs produced by the neutrophilic dermatoses. Most reports suggest that corticosteroids can effectively treat such pulmonary and skin manifestations of the disease.