Article Text

Abstract
Two cases of formes frustes variants of Churg–Strauss syndrome are reported, who were treated with an antibody against immunoglobulin E as an addition on rescue therapy.
Statistics from Altmetric.com
Churg–Strauss syndrome (CSS), or allergic granulomatous angiitis, is a form of systemic vasculitis characterised by eosinophilia in patients with a background of allergy.1 According to the American College of Rheumatology (ACR), four of six criteria lead to a diagnosis of CSS. These criteria are asthma, eosinophilia (>10%), paranasal sinusitis, pulmonary infiltrates, histological proof of vasculitis with extravascular eosinophils and mononeuritis multiplex or polyneuropathy.2 A “forme fruste” CSS can develop after withdrawal of steroids administered by inhalation or systemically as an asthma therapy. Steroids may have masked the underlying CSS in these cases.3 Although CSS has a good prognosis in general, some patients do not respond to therapy, including corticosteroids and cyclophosphamide. Patients with a poor prognosis may benefit from, for example, azathioprine, interferon α, ciclosporin, plasma exchange or intravenous immunoglobulin (Ig). Results of these rescue therapies are contradictory.4 To date, no report of a rescue therapy in CSS with omalizumab, an IgE antagonist, has been described.
CASE REPORTS
Case No 1
A 60-year-old woman had a history of bronchial asthma for more than 40 years, seasonal allergic rhinitis and nasal polyposis. She received occasional short courses of inhaled and oral steroids for exacerbations of asthma. In skin prick testing she was allergic to grass and herbs pollen. In the winter of 2000 she developed talocrural arthritis with cutaneous reaction. She had an eosinophilia of 44%, which was observed for the first time. Skin biopsy demonstrated leucocytoclastic eosinophilic vasculitis. With four of six ACR criteria fulfilled, CSS was felt to be the most likely diagnosis. As long term use of systemic and inhaled steroids seemed to have masked the underlying CSS, we considered a “forme fruste” CSS to be the correct classification.
After treatment with oral prednisone, the clinical symptoms disappeared. In 2004, on low dose therapy, she developed perimyocarditis with a left ventricular ejection fraction of 30%. After high dosage treatment with systemic prednisone and cyclophosphamide, the patient recovered. However, she developed proteinuria, and cyclophosphamide had to be exchanged for azathioprine. We decided to initiate a weight (72 kg) and serum IgE level adapted omalizumab therapy in February 2006 (150 mg subcutaneously) because of progressive worsening of the clinical presentation despite high dose immunosuppressive treatment. The reason for this experimental and off label treatment was the observation that patients with a hyper-IgE syndrome often also show elevated eosinophils which diminish under anti-IgE therapy.5 After the first two doses of omalizumab were administered, the patient showed marked clinical improvement and gained the weight that she had lost before (8 kg in 6 months). Therefore, we decided to continue the therapy every 2 weeks. Eosinophils reached normal values and immunosuppressive treatment was tapered. Since May 2006, azathioprine has been stopped and while preparing this manuscript the patient is on 2.5 mg of prednisone/day. Omalizumab has been administered every 4 weeks (150 mg) since June 2007.
Case No 2
The second case describes a 65-year-old woman with a history of hay fever with allergic conjunctivitis and pollinosis nasi since 1982. In allergy testing a sensibility towards hazel, alder and willow was observed. Over the course of the disease, she developed increasing symptoms of bronchial asthma and was treated annually in the spring and summer with inhaled and systemic steroids from 1990. Under adequate therapy the patient was almost free of symptoms. In 2002 the patient described progressive distal dysaesthesia in both arms. A neurological and diabetological exploration detected no cause of these symptoms. In the autumn of 2004, she presented with persistent dyspnoea, even in the absence of allergens. Lung function tests proved bronchial obstruction with reversibility after administration of inhaled betamimetics. Chest radiography showed diffuse bilateral interstitial infiltrates. Bronchoscopic biopsy revealed eosinophil infiltrates with vasculitis. Blood eosinophilia was 48%.
CSS was regarded as the appropriate diagnosis with five of the six ACR criteria being fulfilled. Also, in this case a “forme fruste” CSS was the most accurate classification as withdrawal of steroids had exposed the masked CSS. Symptoms resolved after initial treatment with oral and topical steroids and later cyclophosphamide for steroid sparing. Cyclophosphamide was replaced by azathioprine because of proteinuria. Clinical status, especially bronchial obstruction, deteriorated again despite elevation of prednisone to 70 mg/day in combination with 50 mg azathioprine/day. As the patient has kept exact records about her disease and dosage of steroids, we believe that non-adherence to steroids was not the problem.
Given a refractory CSS, we decided to start weight and IgE level adapted (64 kg) anti-IgE therapy in February 2006. The patient improved clinically, dyspnoea disappeared and eosinophils declined to 1%. Up until February 2007, the patient received 150 mg of omalizumab every 2 weeks and the dose of prednisone was tapered to 7.5 mg/day. Administration of azathioprine was stopped in December 2006. In May 2007, the patient also wished to stop therapy with omalizumab. In July 2007, the patient relapsed with progressive bronchial obstruction and elevated eosinophils. Interestingly, the IgE count did not change while not receiving omalizumab. Chest x ray again showed diffuse interstitial infiltrates which had completely resolved. Oral prednisone was increased to 70 mg/day and anti-IgE therapy was started again, with 150 mg every 2 weeks. The clinical status improved dramatically within 6 weeks. Also, the elevated eosinophils reached normal values. As of October 2007, the patient is doing well clinically, and systemic steroids were tapered to a daily dose of 5 mg. Chest x ray has not normalised but it has improved markedly compared with at the time of relapse.
DISCUSSION
The observed effects in both patients persisted for 18 months from the beginning of administration of omalizumab. Moreover, the structured treatment interruption in patient No 2 with consecutively observed relapse underlines the apparent improvement and stabilisation of two patients with a forme fruste CSS.
Data on blood eosinophilia and IgE counts are shown in table 1 and fig 1. In both patients eosinophils were reduced significantly whereas total IgE count in serum declined only in patient No 2. The reason for this is that commercially available IgE test kits only detect total IgE which is composed of free IgE and IgE in complex with anti-IgE. Therefore, it is meaningless to measure IgE in this way. Free IgE was not measured.
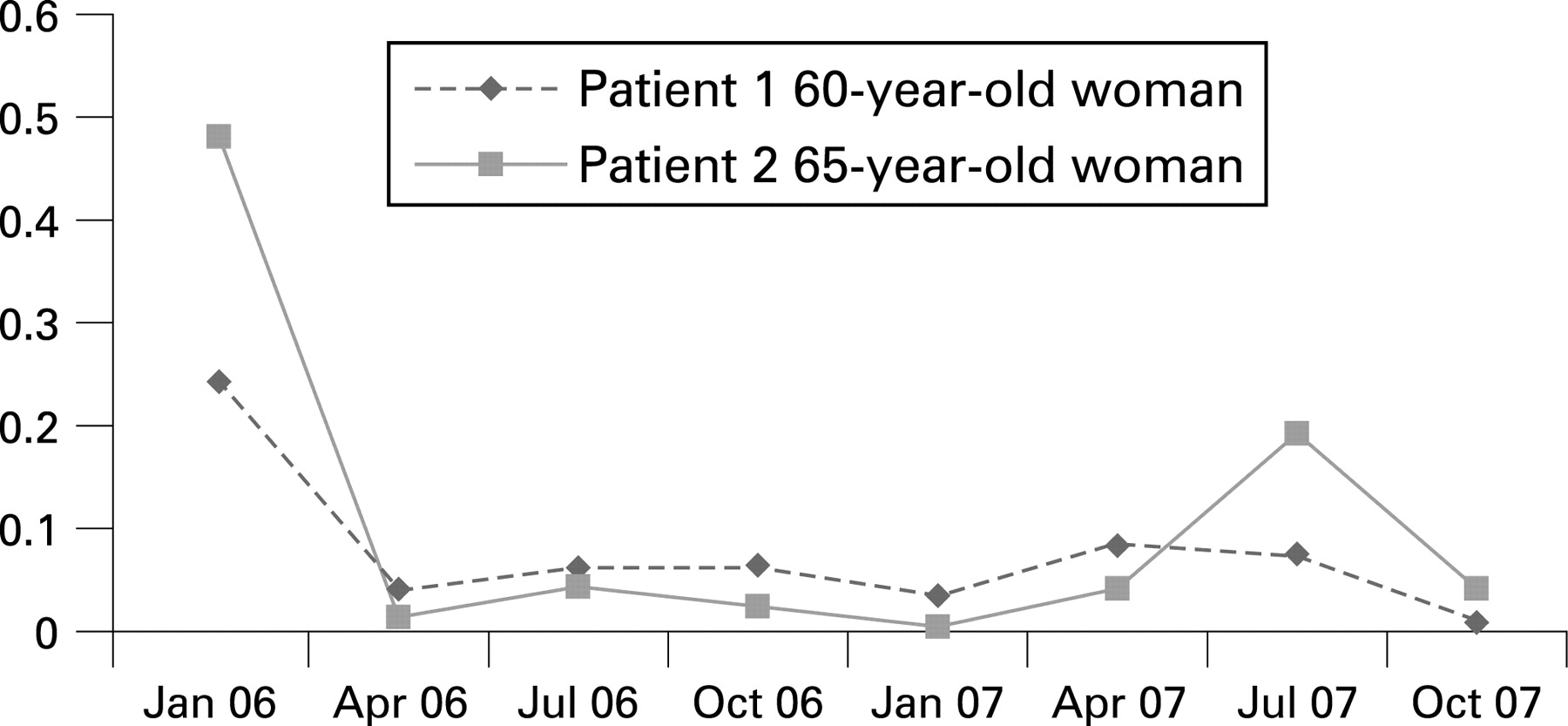
{kind=link}
Omalizumab is a recombinant monoclonal antibody that binds to human IgE that inhibits the binding of IgE to the high affinity IgE receptor (FcϵRI) on the surface of mast cells and basophils. Reduction in surface bound IgE on FcϵRI bearing cells limits the degree of release of mediators of the allergic response. But there are other potential pharmacological and immunoregulatory effects which also lead to the reduction in eosinophils.5 6 The mechanisms by which omalizumab decreases airway eosinophilia has not been specifically investigated to date but probably involves inhibition of IgE dependent mechanisms of eosinophil accumulation. For example, this possibly includes allergen induced cross linking of IgE on the surface of effector cells, such as mast cells, causing release of eosinophil active cytokines. It is remarkable that patient No 1 showed a very low IgE level at the beginning of the therapy. However, eosinophils decreased significantly under therapy. This raises the question of whether there are other as yet uncovered underlying mechanisms.
Omalizumab has been approved for the therapy of severe asthma bronchiale since 2003. As the pathomechanisms and clinical presentation in bronchial asthma and CSS seem to overlap, we considered anti-IgE therapy in severe cases as helpful. In the two cases reported here, the clinical benefit was impressive together with a reduction in the standard immunosuppressive therapy. As the “forme fruste” variant of CSS offers a challenge to standard treatment, anti-IgE therapy may be helpful, in particular if therapy with cyclophosphamide has to be replaced because of side effects. The long term benefit and individual strategy to treat patients with CSS should be taken into account.
Footnotes
Competing interests: None.
Ethics approval: Ethics approval was obtained.
Patient consent: Obtained.