Article Text

Abstract
Background: The performance of CURB65 in predicting mortality in community-acquired pneumonia (CAP) has been tested in two large observational studies. However, it has not been tested against generic sepsis and early warning scores, which are increasingly being advocated for identification of high-risk patients in acute medical wards.
Method: A retrospective analysis was performed of data prospectively collected for a CAP quality improvement study. The ability to stratify mortality and performance characteristics (sensitivity, specificity, positive predictive value, negative predictive value and area under the receiver operating curve) were calculated for stratifications of CURB65, CRB65, the systemic inflammatory response syndrome (SIRS) criteria and the standardised early warning score (SEWS).
Results: 419 patients were included in the main analysis with a median age of 74 years (men = 47%). CURB65 and CRB65 stratified mortality in a more clinically useful way and had more favourable operating characteristics than SIRS or SEWS; for example, mortality in low-risk patients was 2% when defined by CURB65, but 9% when defined by SEWS and 11–17% when defined by variations of the SIRS criteria. The sensitivity, specificity, positive predictive value and negative predictive value of CURB65 was 71%, 69%, 35% and 91%, respectively, compared with 62%, 73%, 35% and 89% for the best performing version of SIRS and 52%, 67%, 27% and 86% for SEWS. CURB65 had the greatest area under the receiver operating curve (0.78 v 0.73 for CRB65, 0.68 for SIRS and 0.64 for SEWS).
Conclusions: CURB65 should not be supplanted by SIRS or SEWS for initial prognostic assessment in CAP. Further research to identify better generic prognostic tools is required.
- ATS, American Thoracic Society
- AUC, area under the receiver operating curve
- BTS, British Thoracic Society
- CAP, community-acquired pneumonia
- EWS, early warning score
- ICU, intensive care unit
- NHS, National Health Survey
- NPV, negative predictive value
- PPV, positive predictive value
- PSI, pneumonia severity index
- ROC, receiver operating curve
- SEWS, standardised early warning score
- SIRS, systemic inflammatory response syndrome
Statistics from Altmetric.com
- ATS, American Thoracic Society
- AUC, area under the receiver operating curve
- BTS, British Thoracic Society
- CAP, community-acquired pneumonia
- EWS, early warning score
- ICU, intensive care unit
- NHS, National Health Survey
- NPV, negative predictive value
- PPV, positive predictive value
- PSI, pneumonia severity index
- ROC, receiver operating curve
- SEWS, standardised early warning score
- SIRS, systemic inflammatory response syndrome
Community-acquired pneumonia (CAP) is an important quality improvement target in acute medicine.1 Recent, major national and specialist society CAP guidelines suggest the use of prognostic (severity) assessment in guiding clinical decisions about the level of intervention required.2–,5 The British Thoracic Society (BTS)2, Infectious Diseases Society of America3 and the Canadian Thoracic Society4 guidelines recommend the use of validated prognostic tools6,7 on admission to hospital as adjuncts to clinical judgement in guiding the management of patients with CAP. The pneumonia severity index (PSI) has been used to identify low-risk patients who can be managed equally effectively at home or as inpatients.8,9,10
In the United Kingdom, the BTS guidelines promote the use of CURB65,7 which is based on four bedside and one laboratory based prognostic marker (table 1⇓). This tool, which is an evolution of two previously validated prognostic rules,11,12 was shown to have 75% sensitivity and 75% specificity for predicting death at 30 days in CAP in the validation set of a large prospective multicentre, multinational derivation/validation study.7 CRB65, which does not require a blood urea level, was shown to stratify mortality similarly, but had inferior performance characteristics. There is evidence that junior doctors, however, have poor awareness of the BTS recommendations. In a survey of 83 junior and middle grade doctors, only 4% could correctly state all four prognostic markers of the BTS CURB tool.13 Woodhead suggested that the use of a generic rather than a pneumonia-specific predictive tool might be easier for doctors to remember and use in the clinical management of patients.14
Definitions of each of the four prognostic tools studied
Ewig et al15 have previously compared the performance of CURB, the precursor of CURB65, with that of the PSI, the modified American Thoracic Society (ATS) rule for predicting the need for intensive care unit (ICU) admission, and the American College of Chest Physicians-Society of Critical Care Medicine’s definition of sepsis. The ATS rule performed the best with the PSI and CURB having similar performance characteristics. More recently, when compared with the PSI, CURB65 was shown to have equivalent performance.16 CURB65 has not been compared, however, with generic sepsis or early warning scores. The study reported in this paper compared the performance of CURB65 and CRB65 in predicting death with that of two commonly used generic scores, the systemic inflammatory response syndrome (SIRS) and the standardised early warning score (SEWS) (table 1⇑). SIRS is recognised worldwide as a component of the definition of sepsis.17 It is often used to define and stratify sepsis in research,18 and has been incorporated into our and other hospitals’ sepsis guidelines. SEWS19 is a modified version of an early warning score (EWS),20 which has increasingly been advocated for use in the acute medical environment to guide the intensity of nursing observation and medical management.20–,22 Our hypothesis was that SIRS and SEWS would perform at least as well, or better, than CURB65 and CRB65 in predicting mortality in CAP.
METHODS
A retrospective analysis of prospectively collected data was performed. The data used were collected as part of a controlled before-and-after study over two winter periods (November to April 2001/02 and 2002/03) to evaluate the implementation of a quality improvement programme to improve the delivery and appropriateness of prescribing antibiotics for patients hospitalised with CAP.23 Potential subjects were identified by a review of admission records from two hospitals, one a 1000-bed teaching hospital and the other a 500-bed district general hospital. Patients were included if they were receiving antibiotics for a suspected lower respiratory tract infection and had either a new infiltrate on the chest radiograph or had been clinically diagnosed as having CAP by a specialist registrar or consultant doctor. Patients were excluded if they had one or more of the following criteria: (1) a non-pneumonia diagnosis; (2) aspiration, hypostatic or hospital-acquired pneumonia; (3) the initial diagnosis of CAP was changed before discharge from the hospital; (4) the patient was HIV-positive, neutropenic (<1.0×109/l) secondary to chronic illness or treatment, or markedly immunosuppressed (long term (>2 weeks) prednisolone (or equivalent) of ⩾10 mg or immunosuppressive therapy such as methotrexate, azathioprine, mycophenalate, etc); (5) progressive malignancy; (6) the patient had chronic respiratory disease other than asthma or chronic obstructive pulmonary disease; (7) age <16 years.
Demographic, clinical and outcomes data were collected using a pre-piloted data collection form. The criteria used to establish the CURB65, CRB65, SIRS and SEWS scores were taken from the earliest recorded reading/result in the patients medical/nursing records (ie, on admission to hospital). Patients were reviewed on alternate days until discharge from the hospital or death. Deaths after discharge, but within 30 days of admission to hospital were established by the hospital’s computer database. Data were subsequently audited and double entered into an Epi-Info database (Centers for Disease Control, Atlanta and World Health Organisation, Geneva). Statistical analyses were performed using SPSS V.10. Descriptive statistics are given as medians or percentages with 95% confidence intervals (CI) where appropriate. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy were calculated for stratifications of the four tools. A receiver operator curve (ROC) was produced for each tool. The area under the curve (AUC) for each of these and associated standard errors (SE) and 95% CI were also calculated. Table 2⇓ shows the definitions of the above performance characteristics.24,25
Definitions of performance characteristics
Table 1⇑ shows the definitions of each of the four tools. Severity was defined according to how one would expect to use the tools in clinical practice. For CURB65, therefore, severe CAP was defined as a score of ⩾3.7 For CRB65, severe CAP was defined as a score of 3 or 4 as suggested by the findings of Lim et al.7 For SEWS, severe CAP was defined as a score of ⩾4 as it is at this level of score that the SEWS chart recommends early intervention by a doctor.19 We did not include a urine output score in the calculation of SEWS. SIRS was analysed in four different ways to establish the best performing variation of this tool and the most appropriate cut-offs to define severe CAP. For SIRS, hypotension was defined as a systolic blood pressure <90 mm Hg. Organ hypoperfusion was defined as new confusion (MSQ ⩽8/10 or a 2 point drop in MSQ). We did not attempt to separate patients with severe sepsis from those with septic shock as, by definition, septic shock cannot be diagnosed on admission to hospital until the patient has received adequate intravenous fluid resuscitation. We have therefore assumed that patients who went on to be diagnosed with septic shock shortly after admission are embedded in the cohort of patients with severe sepsis.
RESULTS
Of the 503 patients (a description of the whole cohort is provided in Appendix A available online at http://thorax.bmj.com/supplemental) included in the quality improvement study, full data for all four tools were available for 419 (83%) patients. Table 3⇓ shows the descriptive statistics for this cohort of patients. Reasons for exclusion from the original quality improvement study have previously been published.23 Most deaths occurred within the first week of admission (72%) with 14% occurring in the second week and the remainder (14%) between 15 and 30 days. Table 4⇓ shows the mortality for severity stratifications of the four tools and associated sensitivity, specificity, PPV and NPV. Based on the results of these analyses, for SIRS, we defined severe CAP as the presence of hypotension and/or organ hypoperfusion without SIRS or severe sepsis/septic shock (table 4⇓).
Demographic and clinical characteristics of the patients included
Operating characteristics of CURB65, CRB65, systemic inflammatory response syndrome criteria used in four different ways and standardised early warning score
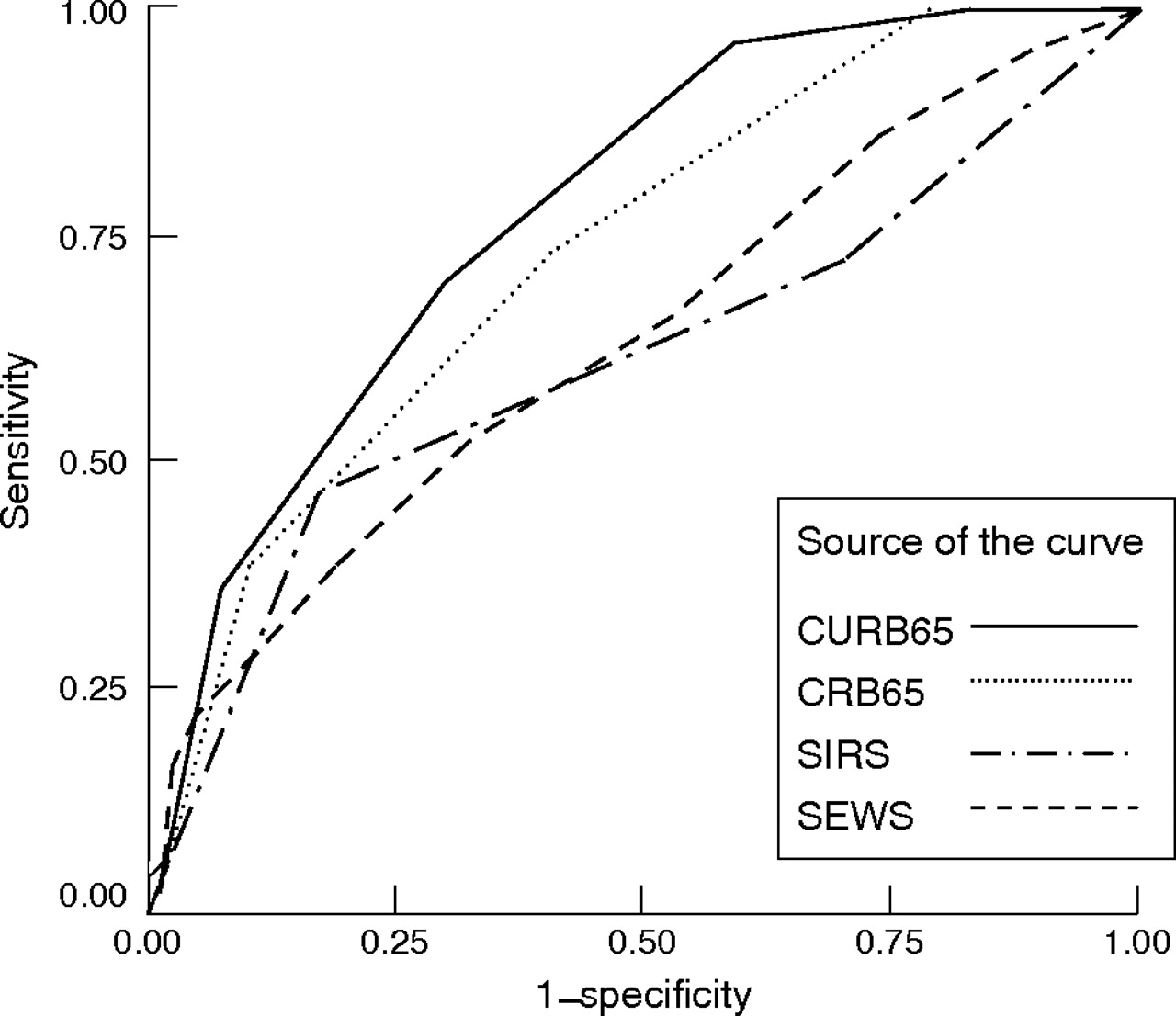
CURB65 and CRB65 were the only tools that identified a genuinely low risk group of patients (2% in CURB65 = 0 or 1 patients v 0% in CRB65 = 0 patients v 9% in the SEWS = 0 or 1 patients and 11% in patients without SIRS or hypotension or hypoperfusion). Figure 1⇓ shows the ROCs. The ROC for CURB65 had the greatest AUC (0.78, SE 0.025, 95% CI 0.73 to 0.83) followed by CRB65 (0.73, SE 0.029, 95% CI 0.67 to 0.79), SIRS (0.68, SE 0.035, 95% CI 0.61 to 0.75) and SEWS (0.64, SE 0.035, 95% CI 0.57 to 0.70). The overall accuracy of the four tools was 70% for CURB65, 79.5% for CRB65 (62% for a cut-off of ⩾2 for severe CAP; see later discussion), 71% for SIRS and 64% for SEWS.

{kind=link}
Receiver operating curve for each prognostic tool. SEWS, standardised early warning score; SIRS, systemic inflammatory response syndrome.
Sub-group analyses were performed on patients who had a chest radiograph reported by a consultant radiologist or seen by a consultant respiratory physician with associated documentation in the patient’s case notes (n = 218). The characteristics of this cohort are shown in Appendix B, available online at http://thorax.bmj.com/supplemental. The operating characteristics of the four tools in this cohort of patients are shown in Appendix C, available online at http://thorax.bmj.com/supplemental. The ROC for each tool is shown in Appendix D, available online at http://thorax.bmj.com/supplemental. As for the main analyses, CURB65 and CRB65 were the only tools to identify a low risk cohort of patients. In contrast to the main analyses, SIRS (as defined above) performed better than CURB65 with respect to sensitivity, specificity, PPV, NPV and accuracy. The ROC for CURB65 still had the greatest AUC (0.79, SE 0.037, 95% CI 0.72 to 0.86), however, followed by CRB65 (0.75, SE 0.043, 95% CI 0.67 to 0.83), SIRS (0.70, SE 0.057, 95% CI 0.59 to 0.81) and SEWS (0.61, SE 0.059, 95% CI 0.49 to 0.72). The overall accuracy of the four tools in this new cohort was 69% for CURB65, 86% for CRB65 (62% for a cut-off of ⩾2 for severe CAP; see later discussion), 76% for SIRS and 61% for SEWS. Table 5⇓ compares the results of this study with two previously reported validation studies.
Comparison of the performance characteristics of CURB65 in three different validation studies
DISCUSSION
Severity assessment is the key to appropriately managing patients with CAP. The results of this study show that two potential generic prognostic tools, SIRS and SEWS, should not be used in preference to CURB65 or CRB65 for predicting mortality in adult patients who present to hospital with CAP. CURB65 and CRB65 outperform both of these tools in two ways. Firstly, and most importantly, their stratification of mortality is more clinically useful and identifies a genuinely low risk group of patients, whereas SIRS and SEWS do not. This means that CURB65 and CRB65 can be used to identify patients who do not require inpatient care unless they have additional comorbidities or signs of respiratory failure.8,9,10 Secondly, they performed better with regard to most of the other performance criteria (except when compared with our modified definition of SIRS in the chest radiograph defined cohort) and had the greatest AUC in all analyses. It is worth noting, however, that none of the tools performed particularly well and all were well below the standard required of population screening tests. This emphasises the importance of combining predictive tools with clinical judgement.
The ease of using each tool in clinical practice should also be considered. CURB65 requires four bedside and one laboratory criteria. Although the laboratory criteria may delay a full assessment on admission to hospital, Lim et al7 have shown earlier that CRB65 stratifies mortality similarly and can therefore be used while awaiting the urea result. In contrast to the conclusions of Lim et al, the results of our study suggest that a CRB65 score of ⩾2 would be a safer cut-off for defining severe CAP. SIRS requires three bed-side and one laboratory criteria as well as an assessment of hypotension and hypoperfusion. Although SEWS requires the most data, all criteria can be measured at the bedside. It does require the availability of a pulse oximeter, however, and accurate measurement of urine output over a 3-h period (see discussion later).
This is now the third published study to assess the predictive performance of CURB65 in CAP.7,16 CURB65 stratified mortality similarly across all three studies (table 5⇑). More importantly, mortality in the two least severe stratifications (ie, 0 and 1) was similar (2%, 1.2% and 0.4%, respectively) thereby confirming that CURB65 can safely identify a low risk cohort of patients. The overall higher mortality seen in our study is likely to reflect the characteristics of the study cohort, in particular, the older median age (74 years v 69 years in the derivation/validation study and the greater proportion of patients with severe CAP; 38% v 29%7). The sensitivity, specificity, PPV and NPV were also similar. In our study these values were 71%, 69%, 35% and 91% when compared with 68%, 75%, 22% and 96% in the validation set and 75%, 75%, 23% and 97% in the derivation set of the validation/derivation study.7
CURB65 has recently been found to have similar performance to the PSI (AUC 0.87 v 0.89) in predicting a 30-day mortality in CAP,16 but is yet to be compared with the modified ATS criteria.26 Ewig et al15 recently compared both of these with the old BTS tool (CURB) and found that the modified ATS criteria performed the best in predicting mortality and the need for admission to an ICU. The performances of CURB and the PSI were comparable. Interestingly, when severe sepsis was used as the cut-off for severity in this study, it had better sensitivity (89% v 51%), PPV (20% v 16%) and NPV (99% v 96%), but worse specificity (70% v 80%) and overall accuracy (71% v 78%) than CURB in predicting mortality. One major caveat of this study is that 17% of patients (versus 3% in our study) were admitted to an ICU, which means that one may not be able to generalise these results to the NHS (National Health Service) setting.
The definition of sepsis, which incorporates SIRS, was published in a consensus statement in 1992 and has since been widely adopted in research and clinical practice.17 In our own hospitals, for example, the definitions given in table 1⇑ have been included in sepsis protocols to guide the intensity of antibiotic treatment. A North American study showed that mortality due to infection increased with the number of SIRS criteria (7% with two criteria, 10% with three criteria and 17% with four criteria) and with severe sepsis (20%) and septic shock (40%).27 Jones and Lowes28 also found a similar relationship in patients with bacteraemia (mortality in patients with no SIRS = 12%, SIRS 2 = 14%, SIRS 3 = 26%, SIRS 4 = 36%, severe sepsis = 38% and septic shock 56%) and it was suggested, on the basis of these studies, that SIRS was “of generalised use in predicting outcome from infection.” Interestingly, as with our study, Jones and Lowes also found a cohort of patients with clinical evidence of hypotension and/or hypoperfusion, but without the classical definition of SIRS. The mortality in this cohort of patients was 29% v 28% in our study, which explains the higher mortality (17% when these patients were included versus 11% when they were classified as a separate cohort) for patients without SIRS (ie, infection only patients).
Since then, the value of the SIRS criteria and the relationship between an increasing number of SIRS criteria and infection has been questioned. In a study of 300 internal medicine patients with a new onset of fever at a university teaching hospital in The Netherlands, Bossink et al29 found that although there was a statistically significant association between the number of positive SIRS criteria and mortality (SIRS 1 = 0%, SIRS 2 = 3%, SIRS 3 = 8%, SIRS 4 = 17%), the performance of the definition of sepsis for predicting mortality was not as good as an alternative model proposed in the paper. In our study, sepsis had a sensitivity of 73%, specificity of 30%, PPV of 20% and NPV of 83% for predicting mortality when compared with 63%, 60%, 13% and 94%, respectively, in the study by Bossink et al. A recent, multicentred study using data from 3608 ICU patients who had taken part in the European Sepsis Study found a gradation in mortality from uncomplicated infection or sepsis (25%) to severe sepsis (40%) to septic shock (60%).30 We found a similar association depending on how the sepsis definitions were used: from 13% (infection and SIRS) to 38% (severe sepsis/septic shock) with the classical definition and from 11% (infection and SIRS) to 28% (hypotension or hypoperfusion without SIRS) to 38% (severe sepsis/septic shock) with our alternative definition. As with our study, they did not find any difference in mortality between patients with infection without SIRS and sepsis or an association between the number of SIRS criteria and mortality in these groups. The SIRS criteria may also have performed less well in our study because two of the criteria, heart rate and white cell count, have not been strongly associated with outcome in CAP.7,31
In contrast to SIRS, there are less data supporting the use of SEWS in infection. This is a concern, given the increasing rate at which it is being implemented in acute medical admissions units in the UK. Indeed, implementation is being encouraged by major organisations interested in clinical effectiveness, such as NHS Quality Improvement Scotland.19 SEWS is based on an EWS, which was validated for use in acute medical patients in 2001.20 The AUC in the validation study was 0.67 compared with 0.62 in our study (versus 0.78 for CURB65 and 0.68 for SIRS). A subsequent study of 1695 acute medical patients, who were compared with a cohort of patients admitted to the same unit in the previous year, but before implementation of the EWS, did not show any change in mortality as a result of implementation.21 A recent study, again from the UK, of 1047 ward patients assessed by an intensive care outreach service, found a strong statistical association between the EWS and the need for intervention or mortality.32 As with SIRS, the EWS has been tested in different cohorts of patients in different contexts and it is debatable as to whether this evidence can be generalised to all patient populations. In our study, SEWS was better than SIRS at stratifying mortality. It is possible therefore, that it could still be used to identify patients at high risk of needing critical care, once the initial decisions about an appropriate site of care and antibiotic treatment have been made. Overall, however, SEWS performed less well than CURB65, CRB65 and SIRS with regard to other operating characteristics.
There are a number of caveats to the interpretation of the results of our study. Patients were included using a pragmatic, real-life definition of CAP. Sub-group analysis of a chest radiograph defined cohort of patients, however, confirmed the findings of our main analyses. Because the performance of all tests is context dependent, one may not be able to extrapolate our results to healthcare systems dissimilar to the NHS. We also used a limited definition of hypoperfusion to define severe sepsis and septic shock. We feel that this is justified given that the inclusion of acidosis in clinical practice would require an additional blood test, which is not performed in all patients with CAP. Indeed, the BTS guidelines recommend arterial blood gas measurement only when the patient’s oxygen saturation is <92% or other features of severe pneumonia are present.2 Additionally, acidosis probably affects only a relatively small number of the most severely ill patients. As urine output cannot be measured accurately on admission to hospital and would therefore delay the assessment of severity and reduce the practicality of the tool, oliguria was also excluded as a criterion of hypoperfusion and was not scored in SEWS. When using SEWS, it is recommended that ⩾3 h of urine output be assessed. Given that there are six other SEWS criteria, and that oliguria would be an unusual isolated finding in severe CAP, it is unlikely that the omission of this would have resulted in poorer SEWS performance. Also, oliguria was not included in the validation study by Subbe et al.20 Nevertheless, it is possible that the omission of these criteria, in particular for SIRS, may have changed performance characteristics.
In summary, CURB65 and CRB65 were better at stratifying mortality and outperformed SIRS and SEWS in predicting 30-day mortality in CAP. For the time being, other prognostic tools should not supplant CURB65 in the initial assessment of patients with CAP. There is clearly a need for corroboration of our results and the development of better generic predictive tools for use in acute medicine and sepsis.
CONTRIBUTORS
GB had the initial study idea, collected and analysed the data and wrote the initial draft of the paper. PD and DN were involved in developing the initial idea and edited the initial and subsequent drafts of the paper. PD is the guarantor.
REFERENCES
Footnotes
Published Online First 23 August 2006
Funding: The original quality improvement project was funded by NHS Education Scotland and The Chief Scientist Office, Scotland.
Competing interests: None.
Ethical approval: Collection of data was approved by both Tayside University Hospitals NHS Trust’s medical ethics committee and Caldicot guardian.