Article Text

Abstract
Background: Studies examining the physiological interactions of oxygen (O2) and bronchodilators (BD) during exercise in chronic obstructive pulmonary disease (COPD) should provide new insights into mechanisms of exercise intolerance. We examined the effects of O2 and BD, alone and in combination, on dyspnoea, ventilation (V̇e), breathing pattern, operating lung volumes, and exercise endurance.
Methods: In a randomised, double blind, crossover study, 16 patients with COPD (mean (SE) FEV1 43(3)% predicted) performed pulmonary function tests and an incremental exercise test, then completed four visits in which they received either nebulised BD (ipratropium 0.5 mg + salbutamol 2.5 mg) or placebo (PL) with either 50% O2 or room air (RA). After 90–105 minutes the patients performed pulmonary function tests, then breathed RA or O2 during symptom limited constant load exercise at 75% peak work rate.
Results: With BD the mean (SE) increase in inspiratory capacity (IC) was 0.3 (0.1) l (p<0.05) at rest and during exercise, permitting greater tidal volume (Vt) expansion during exercise and a greater peak V̇e. With O2, V̇e decreased during exercise as a result of decreased breathing frequency (F), with no significant change in IC. During exercise with BD+O2, IC and Vt increased, F decreased, and V̇e did not change. Dyspnoea decreased with all interventions at a standardised time during exercise compared with PL+RA (p<0.05). Endurance time was significantly (p<0.05) greater with BD+O2 (10.4 (1.6) min) than with O2 (8.5 (1.4) min), BD (7.1 (1.3) min) and PL+RA (5.4 (0.9) min).
Conclusion: By combining the benefits of BD (reduced hyperinflation) and O2 (reduced ventilatory drive), additive effects on exercise endurance were observed in patients with normoxic COPD.
- BD, bronchodilator
- COPD, chronic obstructive pulmonary disease
- EELV, end expiratory lung volume
- EILV, end inspiratory lung volume
- F, breathing frequency
- FEV1, forced expired volume in 1 second
- FRC, functional residual capacity
- FVC, forced vital capacity
- IC, inspiratory capacity
- IRV, inspiratory reserve volume
- O2, oxygen
- Paco2, arterial carbon dioxide tension
- Pimax, maximal inspiratory pressure
- PEFR, peak expiratory flow rate
- PL, placebo
- RA, room air
- RV, residual volume
- Sao2, oxygen saturation
- Ti, Te, inspiratory and expiratory time
- TLC, total lung capacity
- Tlco, lung carbon monoxide transfer factor
- V̇co2, carbon dioxide output
- V̇e, minute ventilation
- V̇o2, oxygen consumption
- Vt, total volume
- chronic obstructive pulmonary disease
- bronchodilators
- oxygen
- exercise
- dyspnoea
- lung hyperinflation
Statistics from Altmetric.com
- BD, bronchodilator
- COPD, chronic obstructive pulmonary disease
- EELV, end expiratory lung volume
- EILV, end inspiratory lung volume
- F, breathing frequency
- FEV1, forced expired volume in 1 second
- FRC, functional residual capacity
- FVC, forced vital capacity
- IC, inspiratory capacity
- IRV, inspiratory reserve volume
- O2, oxygen
- Paco2, arterial carbon dioxide tension
- Pimax, maximal inspiratory pressure
- PEFR, peak expiratory flow rate
- PL, placebo
- RA, room air
- RV, residual volume
- Sao2, oxygen saturation
- Ti, Te, inspiratory and expiratory time
- TLC, total lung capacity
- Tlco, lung carbon monoxide transfer factor
- V̇co2, carbon dioxide output
- V̇e, minute ventilation
- V̇o2, oxygen consumption
- Vt, total volume
In patients with more advanced chronic obstructive pulmonary disease (COPD), ventilatory constraints and the associated respiratory discomfort (dyspnoea) contribute importantly to poor exercise performance. Recent consensus guidelines have correctly highlighted the importance of reducing dyspnoea and activity limitation as an effective means of improving perceived health status in these patients.1,2 An individualised integrated management plan that combines pharmacological and non-pharmacological interventions is most likely to be successful in achieving these goals.
Our understanding of the mechanisms of dyspnoea relief following bronchodilator therapy continues to grow. All classes of bronchodilators have been shown to improve airway conductance and to facilitate lung emptying. In patients with moderate to severe disease, the consequent reduction in end expiratory (EELV) and end inspiratory (EILV) lung volumes allows greater tidal volume expansion and ventilation during exercise with less exertional dyspnoea.3–6 However, the impact of different bronchodilators on these operating volume components during exercise appears to vary, and this inter-patient variability has not been studied. Moreover, the relative importance of increases in inspiratory capacity (IC) and inspiratory reserve volume (IRV) (reflecting decreases in EELV and EILV, respectively) in contributing to improvement in dyspnoea and activity limitation remains unknown and is also explored further in this study.
Several controlled studies have shown positive effects of hyperoxia on dyspnoea and exercise performance, even in patients with insignificant arterial oxygen desaturation.7,8,9,10,11,12 Exertional dyspnoea relief during hyperoxia is multifactorial but appears to be linked to the attendant reduction in ventilation during exercise.7,13 However, it remains uncertain whether hyperoxia induced reduction in ventilation is associated with a reduced rate of dynamic hyperinflation during exercise in normoxic patients with COPD. In this regard, different studies have yielded conflicting results, suggesting that there is considerable inter-patient variability in this response.7,8,13 This study was therefore undertaken to examine further the relative contribution of reduced ventilation and reduced lung volumes to dyspnoea relief during hyperoxia.
In the past, dyspnoea relieving interventions such as bronchodilator therapy and supplemental oxygen (O2) have been studied only in isolation, and no information is available on their combined physiological interactions and resultant clinical consequences. In this study we therefore compared the acute effects of bronchodilators and hyperoxia (50% O2), both singly and in combination, in order to gain new insights into the mechanisms of improved dyspnoea and exercise performance. We reasoned that the combination of treatments that both improves dynamic ventilatory mechanics and reduces ventilatory demand would have additive or possibly even synergistic effects on dyspnoea and exercise endurance in patients with moderate to severe COPD who were not significantly hypoxaemic during activity.
METHODS
Subjects
Sixteen clinically stable patients with COPD (forced expiratory volume in 1 second (FEV1) ⩽60% predicted, FEV1/forced vital capacity (FVC) <70%) who were not hypoxic (resting arterial oxygen tension (Pao2) >65 mm Hg (8.7 kPa), exercise oxygen saturation (Sao2) ⩾88%) and had significant activity related breathlessness (modified Baseline Dyspnoea Index score ⩽6)14 were studied. Patients with significant cardiovascular disease, other pulmonary disease, or other disorders that could contribute to dyspnoea or exercise limitation were excluded.
Study design
This randomised, double blind, placebo controlled, crossover study was approved by the local university/hospital research ethics committee. Subjects were recruited from a list of patients who had participated in previous exercise studies. After giving informed consent and screening of medical history, patients were familiarised with all procedures and completed pulmonary function tests and a symptom limited incremental cycle exercise test. During four subsequent visits conducted 2–7 days apart, subjects received one of four treatment combinations in random order: bronchodilator (BD)+room air (RA), placebo (PL)+RA, BD+O2, or PL+O2. At these visits subjects were given either PL or BD, they waited 105 (15) minutes before performing pulmonary function tests, then completed a constant load cycle endurance test at 75% of their maximal incremental work rate while breathing either RA or 50% O2. Subjects adhered to the standard withdrawal of bronchodilators before testing: short acting β2 agonists (4 hours), short acting anticholinergics (6 hours), long acting β2 agonists (12 hours), long acting anticholinergics (48 hours), theophyllines (48 hours), and antileukotrienes (48 hours). Subjects avoided caffeine, alcohol, and heavy meals for 4 hours before testing and avoided major physical exertion entirely on visit days.
Interventions
PL and BD were administered by nebuliser (Parimaster compressor with Pari LC Jet+ nebuliser; PARI Respiratory Equipment Inc, Richmond, VA, USA) in a double blind fashion. The BD used was Combivent (0.5 mg ipratropium bromide + 2.5 mg salbutamol) and PL was sterile 0.9% saline solution. Subjects breathed either RA (21% O2) or 50% O2 on demand from a 200 l Douglas bag reservoir for at least 10 minutes at rest before starting exercise and throughout exercise; they were blinded to the gas mixture being breathed at each test.
Procedures
Pulmonary function measurements were collected using automated equipment (Vmax229d with Autobox 6200 DL; SensorMedics, Yorba Linda, CA, USA) and expressed as percentages of predicted normal values;15–20 predicted IC was calculated as predicted total lung capacity (TLC) minus predicted functional residual capacity (FRC). Symptom limited exercise tests were conducted on an electrically braked cycle ergometer (Ergometrics 800S; SensorMedics) using a cardiopulmonary exercise testing system (Vmax229d; SensorMedics). Incremental testing was performed at the first visit. Subsequent constant load tests were conducted at 75% of the maximal incremental work rate. Exercise test measurements included intensity of dyspnoea (breathing discomfort) and leg discomfort using the 10-point modified Borg scale;21 operating lung volumes derived from IC manoeuvres;22,23 arterialised capillary blood samples taken from the earlobe; and reason for stopping exercise. Endurance time was defined as the duration of loaded pedalling (see the online supplement at http://www.thoraxjnl.com/supplemental for a more detailed description of the procedures).
Statistical analysis
The sample size of 16 provides the power (80%) to detect a difference in IC measured at a standardised exercise time based on a relevant difference of 0.3 l, standard deviation (SD) of 0.3 l for IC changes found at our laboratory, α = 0.05, and a two tailed test of significance. Results are reported as mean (SE). A p value of <0.05 was considered significant in all analyses. Comparisons were made using ANOVA for repeated measures for linear exercise response slopes and for measurements at rest (pre-exercise steady state), at isotime during exercise (the highest common exercise time achieved during all tests performed by a given subject), and at peak exercise (mean of last 30 seconds of loaded pedalling). Paired t tests were used for post hoc analyses. Reasons for stopping exercise were analysed using Fisher’s exact test. Pearson correlations were used to establish associations between standardised dyspnoea ratings (and exercise endurance time) and relevant independent variables; forward stepwise multiple regression analysis was carried out with significant variables and relevant covariates.
RESULTS
Sixteen subjects with moderate to severe airflow obstruction and lung hyperinflation and significantly reduced exercise capacity completed the study (table 1). One additional subject was enrolled in the study but was withdrawn after the first treatment visit due to an adverse reaction (dizziness, nausea) to acute administration of the bronchodilator.
Subject characteristics
Resting pulmonary function
Pulmonary function parameters are shown in table 2. These parameters were measured before exercising with either RA or O2 and reflect responses to nebulised BD or PL only. Measurements on the two PL days were similar (and similar to those at visit 1), demonstrating good repeatability of measurements. Improvements in pulmonary function on the two BD days were also comparable.
Resting pulmonary function measured after placebo (PL) or bronchodilator (BD) but before breathing oxygen (O2) or room air (RA)
Exercise response to bronchodilators
Endurance time increased by 1.7 (0.9) min (41 (16)%) after BD (+RA) compared with PL (+RA) (p = 0.067, table 3). After BD compared with PL, dyspnoea intensity decreased at isotime during exercise (p = 0.008, table 4) and the slope of Borg dyspnoea ratings over time also fell significantly (p = 0.039, fig 1). The main reasons for stopping exercise did not change significantly in response to BD (fig 2). Dyspnoea/V̇e slopes shifted rightwards after BD compared with PL, such that dyspnoea fell by 1.2 (0.3) Borg units (p = 0.001) at a standardised V̇e of 33.4 (2.5) l/min (fig 3).
Symptom limited peak of constant load cycle exercise at 75% Wmax (57 (6) W, 39 (2)% of predicted maximum)
Measurements at isotime (4.1 (0.8) minutes) during constant load cycle exercise

Mean Borg ratings of (A) dyspnoea and (B) leg discomfort over time during constant load cycle exercise at 75% peak work rate. Dyspnoea/time slopes decreased significantly (p<0.05) with bronchodilators (BD) and 50% oxygen (O2), alone and in combination; the combination of O2+BD resulted in greater (p<0.05) dyspnoea relief than either BD or O2 alone. Slopes of leg discomfort over time fell significantly (p<0.05) with O2, either alone or in combination with BD. PL, placebo; RA, room air.

Selection frequency of reasons for stopping symptom limited cycle endurance tests. The percentage of patients stopping exercise mainly because of dyspnoea decreased with oxygen (O2) and bronchodilator (BD), alone or in combination, while other reasons or leg discomfort (combined with dyspnoea) became more predominant. The distribution of reasons for stopping was significantly (p<0.01) different with the treatment combination (O2+BD) compared with room air and placebo (RA+PL).
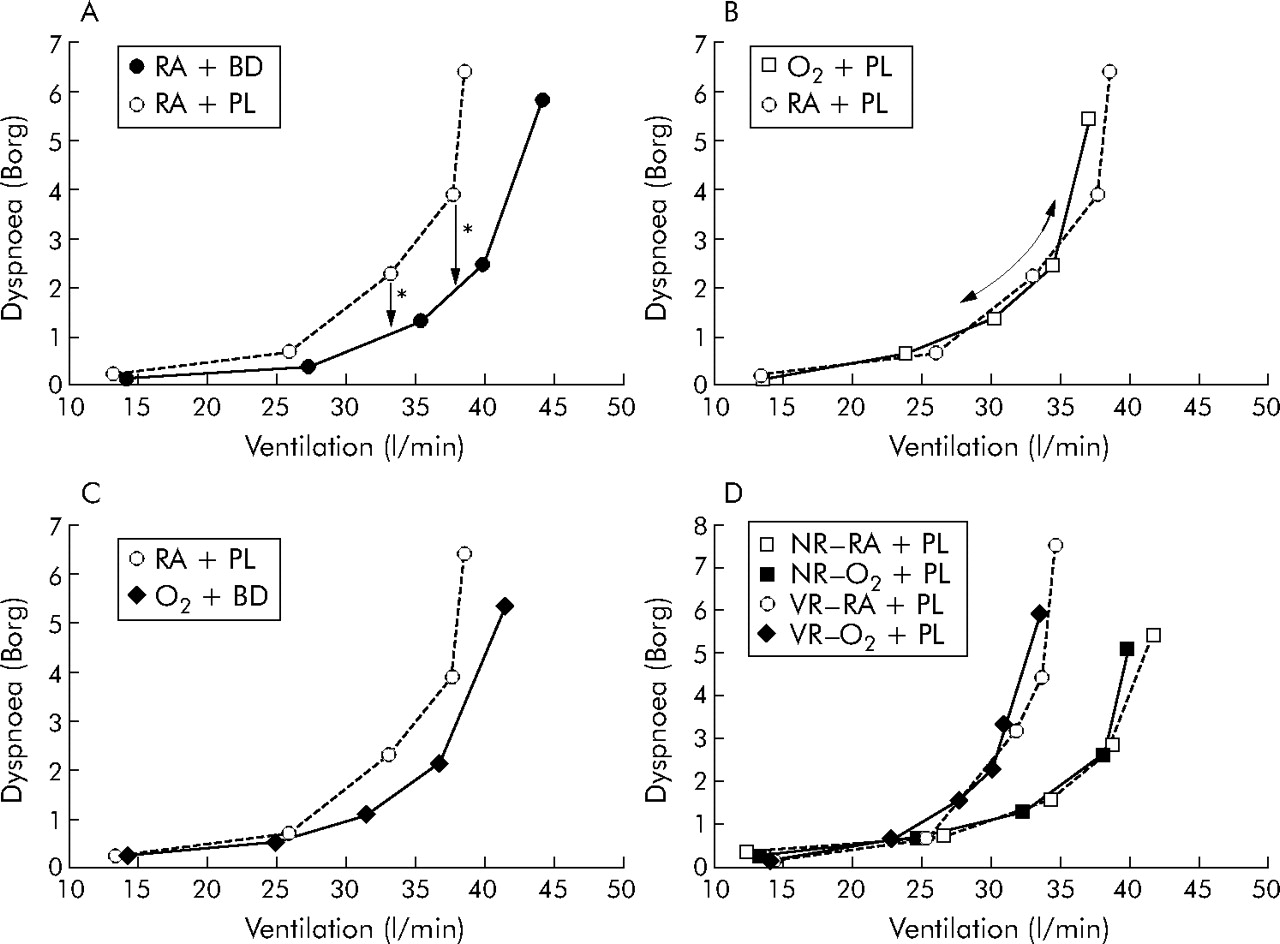
Dyspnoea/ventilation (V̇e) plots for bronchodilators (BD) and 50% oxygen (O2), alone and in combination, compared with placebo (PL) and room air (RA). (A) Dyspnoea/V̇e slopes shift downwards and to the right with BD such that dyspnoea is significantly (*p<0.05) reduced for a given V̇e during exercise. (B) With O2, dyspnoea/V̇e relationships remain unchanged so that dyspnoea falls in conjunction with a fall in V̇e. (C) With O2+BD combined, the dyspnoea/V̇e response falls between those of BD and O2 alone. (D) Responses to O2 are shown for O2 induced “volume responders” (VR: those in whom exercise inspiratory capacity (IC) increased) and “non-responders” (NR: those with no change in exercise IC). Despite differences in slopes on room air and placebo (RA+PL) across subgroups, the dyspnoea/V̇e relationships did not change with O2 in either group.
Bronchodilator induced increases in peak V̇co2, V̇e, Vt, and IC are shown in table 3. Compared with PL at isotime (4.1 (0.8) minutes) during exercise, BD increased IC and Vt (p<0.005), decreased F as a result of increased Ti and Te (p<0.05), with a resultant increase in V̇e (p = 0.06, table 4, fig 4). At a standardised V̇e, the only difference between BD and PL was a reduction in lung hyperinflation (all p⩽0.01): decreases in EELV (−0.35 (0.09) l) and EILV (−0.31 (0.10) l) with reciprocal increases in IC (0.25 (0.07) l) and IRV (0.21 (0.07) l).

Ventilatory responses to constant load cycle exercise for 50% oxygen (O2) and bronchodilators (BD), alone and in combination, compared with room air (RA) and placebo (PL). *See table 4 for significant differences between tests at a standardised time (isotime) during exercise.
All but three subjects had reduced lung hyperinflation at rest with BD compared with PL. In 10 subjects the reduction in resting lung hyperinflation continued during exercise—that is, IC at isotime increased. In these 10 subjects dyspnoea was reduced at isotime by −1.7 (0.7) Borg units (p = 0.031) and exercise endurance improved by 2.7 (1.3) min or 64 (23)% (p = 0.023), whereas there was no change in dyspnoea at isotime (−0.9 (0.6) Borg units) or endurance time (0.1 (0.5) min) in the six subjects with no volume response.
Correlates of improvement
Reductions in dyspnoea/time slopes were greatest in subjects with the steepest non-intervention (RA+PL) dyspnoea/time slopes (r = −0.59, p = 0.016). Dyspnoea/time slopes decreased most in those who experienced the greatest expansion of Vt standardised as % predicted vital capacity measured at isotime (r = −0.54, p = 0.027) or at peak exercise (r = −0.69, p = 0.003), and in those with the largest increases in Te at isotime (r = −0.60, p = 0.014) or at peak exercise (r = −0.56, p = 0.024). Reductions in dyspnoea at isotime correlated best with reductions in concurrent measurements of F (r = 0.64, p = 0.007) and with increases in isotime Ti (r = −0.62, p = 0.010) and Te (r = −0.57, p = 0.020); the combination of change in F and change in EELV (% predicted TLC) explained 50% of the variance in change in dyspnoea at isotime. Reductions in dyspnoea at iso- V̇e correlated best with the concurrent increase in IC (r = −0.46, p = 0.074). Reductions in dyspnoea did not correlate with improvements in FEV1 (p>0.5).
Exercise response to oxygen
Endurance time increased by 3.1 (1.1) minutes (76 (28)%) with O2 + PL compared with RA + PL (p = 0.011). The main reasons for stopping exercise did not change significantly in response to O2 (fig 2). Slopes of Borg ratings of both dyspnoea and leg discomfort over time fell significantly (p<0.05) in response to O2 (fig 1). Dyspnoea/V̇e slopes were similar on O2 and RA (fig 3).
Figure 4 shows exercise responses to O2. Isotime V̇e fell as a result of a concurrent decrease in F (r = 0.65, p<0.01) which, in turn, correlated with increases in Ti (r = −0.87, p<0.0005) and Te (r = −0.64, p<0.01). Changes in V̇e also correlated with concurrent changes in V̇co2 (r = 0.80, p<0.0005), pH (r = −0.65, p<0.05), and base excess (r = −0.58, p<0.05). Paco2 and HCO3− increased during exercise with O2 compared with RA, but not at rest.
On average, operating lung volumes at rest and during exercise did not change significantly with hyperoxia. Compared with RA, seven of the 16 subjects reduced lung hyperinflation during exercise (that is, increased IC at isotime) on oxygen. These subjects had worse maximal expiratory flows than the nine subjects with no volume response to O2 (FEV1/FVC ratios 39 (2)% and 48 (2)% respectively; p = 0.009). Volume responders had significantly steeper dyspnoea/time slopes (p = 0.012) and poorer exercise endurance (p = 0.045) on RA, with greater improvements with O2. Dyspnoea/V̇e relationships were also steeper in volume responders than in non-responders on RA and did not change on O2 (fig 3). O2 induced changes in the ventilatory responses to exercise were generally similar across subgroups, but volume responders had more significant associated decreases in V̇e and Vt/Te (due to increased Te).
Correlates of improvement
Decreases in dyspnoea/time slopes were largest in subjects with the steepest slopes on RA+PL (r = −0.70, p = 0.002). Since dyspnoea/V̇e relationships did not change in response to O2, decreases in dyspnoea were directly related to decreases in V̇e. After accounting for differences in isotime V̇e, increases in isotime IC % predicted explained an additional 45% (p<0.005) of the variance in improvement in dyspnoea/time slopes.
Exercise response to O2+BD
With O2+BD combined, endurance time increased by 5.0 (1.5) minutes (127 (40)%) compared with RA+PL (p = 0.004). This increase was greater (p = 0.01) than with either intervention alone and equalled the sum of increases with BD and O2 singly (p = 0.86; agreement measured by r = 0.86, p<0.0005). By combining interventions, dyspnoea was displaced as the predominant exercise limiting symptom such that more subjects now stopped due to combined breathing and leg discomfort and for other reasons such as being too hot, too tired, or too uncomfortable sitting on the bicycle seat (fig 2). Dyspnoea/time slopes fell significantly in response to O2+BD compared with RA+PL (p = 0.001) and were also different from those with BD (p = 0.010) and O2 (p = 0.045) alone (fig 1). Slopes of Borg ratings of perceived leg discomfort over time fell significantly in response to O2+BD compared with RA+PL (p = 0.002) and compared with BD alone (p = 0.021, fig 1).
For all interventions the relationship between dyspnoea and IRV remained constant (fig 5). Once IRV reached its “minimal” level of 0.4 l, on average, dyspnoea increased steeply until it reached its peak level. The plateau in IRV at this point (fig 5) corresponded with the plateau in the Vt response to exercise (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationships between dyspnoea and inspiratory reserve volume (IRV) during exercise were superimposable for each test. Once a minimal IRV was reached, dyspnoea intensity increased steeply to reach its peak level while no further change occurred in IRV.
By combining O2 and BD, the opposing changes in exercise V̇e resulting from each intervention alone were negated—that is, an increase in Vt (similar to that with BD alone) and a decrease in F (similar to that with O2 alone) resulted in no change in V̇e (fig 4). Adding BD to O2 also reduced the magnitude of increase in Paco2 and HCO3− shown with O2 alone (p<0.05, table 3).
Correlates of improvement
Baseline percentage predicted carbon monoxide transfer factor (Tlco) correlated with improvements in the dyspnoea/time slope with O2+BD (r = 0.62, p = 0.010) and with RA+PL (r = −0.64, p = 0.007). Decreases in dyspnoea at isotime correlated best with reductions in isotime F (r = 0.81, p<0.0005), but also with decreases in V̇e (r = 0.58, p = 0.019) and increases in Te (r = −0.52, p = 0.041); stepwise regression selected the combination of changes in F and EILV/TLC to best predict the relief of dyspnoea at isotime (r2 = 0.74, p<0.0005). Reductions in dyspnoea did not correlate with improvements in FEV1 (p>0.2).
Additional results are presented in the online supplement available at http://www.thoraxjnl.com/supplemental.
DISCUSSION
This is the first study to demonstrate additive effects of BD and O2 therapy on dyspnoea and exercise endurance in normoxic COPD, reflecting the combined salutary influences of improved dynamic mechanics and reduced ventilatory drive. The other novel aspect of this study is that it helps us to understand how these treatments interact.
The effects of hyperoxia on breathing pattern and operating lung volumes were distinctly different from those of BD in the same patients. Consistent with the results of previous studies,4–6,25 BD treatment was associated with a 17% increase in resting IC, thus allowing greater Vt expansion “from below” throughout exercise, within the constraints of the existing diminished IRV. In contrast to previous studies,4–6 mean IRV at a standardised time during exercise was not increased after BD compared with placebo, and dyspnoea/IRV relationships remained superimposed. It follows that IRV recruitment during exercise is not a prerequisite for dyspnoea alleviation during BD treatment provided greater Vt expansion is achieved as a result of an increased IC. Reductions in breathing frequency (increased Ti and Te) in conjunction with increased Vt during exercise probably reflect BD induced improvements in the operating limits for volume expansion. While bronchodilators increased IC, Vt, and V̇e, hyperoxia was associated with reduced V̇e as a result of reduced breathing frequency, with minimal change in Vt or IC. Reduced frequency reflected prolongation of both Ti and Te, but correlated more closely with the increase in Ti (r = −0.87, p<0.0005); there was no change in the inspiratory duty cycle (Ti/Ttot). This consistent effect on respiratory timing must ultimately reflect altered peripheral chemoreceptor input.
The mechanisms of reduced ventilation have been the subject of debate. Most short term studies in health show either no change9,26–29 or a reduction in V̇e during exercise as a result of a fall in breathing frequency, especially at higher submaximal exercise levels.30–32 In studies in non-hypoxic patients with COPD, the range of reduction in exercise V̇e varied between 6% and 15% (that is, approximately 2–6 l/min), again due to a decrease in breathing frequency.30–32
Previous studies on the effect of hyperoxia on oxygen uptake and ventilatory kinetics and blood lactate levels in normoxic COPD patients have shown conflicting results, with the majority of studies showing an improvement in oxidative capacity.7,9,33 We previously reported a reduction in lactate in conjunction with a reduced V̇e during hyperoxia in both hypoxic and non-hypoxic COPD patients.7,13 In the current study the relationship between V̇e and base excess (which is inversely related to blood lactate) was superimposable on O2 and RA, suggesting that the reduction in V̇e during hyperoxia was linked to reduced metabolic acidosis. However, in the present study there was a significant decrease in the V̇e/V̇co2 ratio at a standardised exercise time during O2 with no change during BD. This suggests that the decrease in V̇e and the increase in arterial CO2 during hyperoxia are independent of metabolic factors, and that direct effects of hyperoxia (independent of reduced acidosis) on carotid receptor input cannot be ruled out.
In accordance with the results of our previous study on the effects of hyperoxia in normoxic COPD patients,7 only seven of the 16 patients in the current study had reduced operating lung volumes in response to 50% O2 compared with RA. This small subset of patients had significantly greater baseline airway obstruction, greater ventilatory constraints during exercise, and poorer exercise performance with steeper dyspnoea/V̇e slopes. Moreover, these volume responders had greater depression of V̇e and prolongation of Te, and experienced greater dyspnoea relief with supplemental O2 than the remaining patients.
Combined bronchodilators and hyperoxia
The physiological interactions of the combined interventions resulted in additive effects on exertional dyspnoea and exercise endurance time. The magnitude of this effect (a decrease of 1.75 units in standardised dyspnoea ratings and nearly a twofold increase in endurance time) was impressive and probably clinically important. The dominant physiological effects evident when interventions were considered in isolation were still discernible when they were given in combination. However, the net effect of the combination on exercise V̇e was neutral: the decrease in V̇e as a result of decreased breathing frequency during hyperoxia was counterbalanced by the increased V̇e as a result of increased Vt secondary to BD. Timing component changes during the combination mimicked those seen during hyperoxia alone. The increase in IC at rest and exercise in the BD arm of the study was also preserved during combined treatment. Finally, in spite of an increased cumulative V̇e over an extended exercise duration with the combined treatments, dyspnoea intensity was significantly diminished.
Mechanisms of symptom relief
As previously reported during exercise in COPD,5 this study showed a discernible inflection point in the dyspnoea/IRV relationship such that dyspnoea rose steeply after reaching a “minimal” IRV where further Vt expansion was not possible (fig 5). After this inflection, dyspnoea at this minimal IRV probably rises with the increasing disparity between neural drive (and inspired effort) and the Vt response which is essentially fixed—that is, neuromechanical dissociation.34 It is noteworthy that BD, O2, or a combination of the two had no significant effect on the time course of change of IRV with exercise or on the dyspnoea/IRV relationship, suggesting that factors other than change in IRV are instrumental in both the cause and relief of dyspnoea. Thus, when a minimal IRV is reached during exercise, dyspnoea relief is possible if the intervention releases Vt constriction by increasing IC (for example, in response to BD), reduces neural drive (for example, in response to O2), or accomplishes both of these together. Of note, the 10 patients who had increased exercise IC with BD showed important improvements in dyspnoea and endurance, whereas those with no change in IC did not. It is also of interest that, despite impressive increases in FEV1 (by an average of 28%) following high dose BD treatment, there was no correlation between this variable and improvements in either dyspnoea or exercise endurance. The finding that dyspnoea relief correlated with increased Vt, reduced breathing frequency, and reduced EELV supports the idea that reduced elastic loading is importantly linked to dyspnoea relief with BD.
A comparison of the effects of BD and O2, singly and in combination, on dyspnoea/V̇e slopes allowed us to identify different underlying mechanisms of dyspnoea relief. Dyspnoea intensity fell for a given V̇e after BD compared with placebo, probably reflecting the improvement in ventilatory mechanics outlined above. By contrast, mean dyspnoea/V̇e slopes during O2 and RA were exactly superimposed, suggesting that the reduction in dyspnoea at a standardised time during O2 mainly reflected the concomitant reduction of V̇e. Interestingly, dyspnoea/V̇e slopes remained superimposed on O2 and RA even in the subgroup of patients (n = 7) in whom operating lung volumes were reduced. However, after accounting for the reduction in V̇e, reductions in lung hyperinflation further contributed to dyspnoea relief during O2. Although improved ventilatory mechanics and reduced neural drive have been identified as possible contributory factors in dyspnoea relief in this study, we recognise that other oxygen induced factors (not evaluated in this study) such as reduced pulmonary hypertension, improved left ventricular function, central effects of hyperoxia on the perception of dyspneogenic stimuli, and reduced anxiety may all affect the intensity and quality of exertional dyspnoea on an individual basis.
Combined O2 and BD had additive effects on dyspnoea/time slopes; dyspnoea also fell at a given ventilation during exercise; 74% of the variance in change in dyspnoea ratings at a standardised exercise time was explained by the combination of reduced breathing frequency and EILV. Patients with the lowest Tlco, the most severe exertional dyspnoea, and worst impairment of exercise endurance derived the greatest subjective benefit from the combined interventions. O2 with BD resulted in a dramatic shift in the locus of sensory limitation to exercise such that dyspnoea was now rarely selected by patients as the primary exercise limiting symptom.
During the O2 applications (alone and in combination with BD), perceived leg discomfort fell significantly whereas no such effect was seen with BD alone. The mechanism of benefit is unknown but may indicate an improved metabolic milieu in the active peripheral skeletal muscles with increased intracellular O2 tension. Recent studies by Hogan et al have shown that an oxygen rich environment in the exercising muscles of healthy individuals attenuated muscle fatigue.35 A similar effect has been suggested during 30% O2 in mildly hypoxaemic patients with COPD.36 Improved oxygenation may alter sensory afferent inputs from muscle mechanoreceptors and metaboreceptors or enhance neuromuscular coupling. Reduced fatigue would result in reduced central motor command output and, possibly, attendant reductions in ventilation.37 This may translate into a concomitant reduction of perceived effort required for a given force generation by these muscles. It is intriguing to speculate that similar salutary effects may occur in the ventilatory and peripheral muscles in response to O2, with favourable consequences for the perception of both leg discomfort and exertional dyspnoea.
This study has extended the results of previous mechanistic studies on pharmacotherapy in COPD by showing that effective dyspnoea relief is possible with BD in the absence of increased IRV during exercise, provided there is also an increase in Vt expansion. This study also showed that alleviation of exertional dyspnoea during O2 breathing is possible in normoxic COPD patients in the absence of any consistent reductions in the rate of dynamic hyperinflation. As our analysis of dyspnoea/V̇e slopes suggests, dyspnoea relief during O2 is mainly linked to reduced ventilatory demand. The benefits following O2 and combined O2 and BD were most pronounced in those with the most severe disease, and these individuals showed greater reductions in operating lung volumes during exercise than patients with less severe COPD. The physiological interactions of combining BD and O2 culminated in impressive improvements in exertional symptoms and exercise endurance, thus underscoring the incremental benefits of reducing neural drive and improving dynamic ventilatory mechanics. Finally, this study provides a physiological rationale for the recommendation of O2 therapy as an adjunct to exercise reconditioning for patients with more advanced normoxic COPD who remain incapacitated by dyspnoea despite optimisation of bronchodilators.
REFERENCES
Supplementary materials
Files in this Data Supplement:
- view PDF - Figure 1. Differences in measurements at isotime during constant-load cycle exercise for O2-induced "volume responders" and "non-responders".
- view PDF - Combined effects of bronchodilators and hyperoxia on dyspnoea and exercise endurance in normoxic COPD. M M Peters, K A Webb, D E O�Donnell: Methods, Results and References.
Footnotes
-
Published Online First 7 February 2006
-
This study was supported by the Ontario Ministry of Health, Ontario Thoracic Society, and the William M Spear Endowment Fund, Queen’s University.
-
Competing interests: none.
-
Presented in part at the ALA/ATS International Conference, San Diego, May 2005 (
Linked Articles
- Airwaves