Article Text

Abstract
Background: Intravenous aminophylline is commonly used in the treatment of exacerbations of chronic obstructive pulmonary disease (COPD), despite limited evidence for its efficacy and known risks of toxicity. We hypothesised that adding intravenous aminophylline to conventional treatment would not produce clinically important changes in the speed of spirometric or symptomatic recovery or shorten hospital stay in patients with exacerbations of COPD.
Methods: Eighty patients admitted to hospital with non-acidotic exacerbations of COPD were recruited at admission to a randomised, double blind, placebo controlled study comparing intravenous aminophylline 0.5 mg/kg/hour after an appropriate loading dose with an equivalent volume of 0.9% saline. The primary outcome was the change in post-bronchodilator forced expiratory volume in 1 second (FEV1) over the first 5 days of the admission. Secondary end points were changes in self-reported breathlessness, arterial blood gas tensions, forced vital capacity (FVC), and length of hospital stay.
Results: There was no difference in the post-bronchodilator FEV1 over the first 5 days between the aminophylline and placebo groups. In the aminophylline group, 2 hours of treatment produced a small but significant rise in arterial pH (p = 0.001) and a fall in arterial carbon dioxide tension (p = 0.01) compared with placebo treatment. There were no differences in the severity of breathlessness, post-bronchodilator FVC, or length of hospital stay between the groups. Nausea was a more frequent side effect in the aminophylline group (46% v 22%; p<0.05), but palpitations and headache were noted equally in both groups.
Conclusions: Although intravenous aminophylline produced small improvements in acid-base balance, these did not influence the subsequent clinical course. No evidence was found for any clinically important additional effect of aminophylline treatment when used with high dose nebulised bronchodilators and oral corticosteroids. Given its known toxicity, we cannot therefore recommend the use of intravenous aminophylline in the treatment of non-acidotic COPD exacerbations.
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- chronic obstructive pulmonary disease
- exacerbations
- aminophylline
- theophylline
Statistics from Altmetric.com
Hospitalisation due to an exacerbation of chronic obstructive pulmonary disease (COPD) is a major cause of morbidity and mortality worldwide.1 Treatment of these episodes is relatively standardised, comprising controlled oxygen therapy, high dose nebulised β agonist and/or anticholinergic drugs, oral corticosteroids,2,3 and ventilatory support as needed.4 Several guidelines recommend that intravenous aminophylline be considered as an option when response to the above treatment is not adequate,5,6 since theophylline shows some additivity with the effects of other treatment in stable disease.7 It has been difficult to show that this occurs in acute exacerbations, and although a recent meta-analysis could not exclude a positive beneficial effect, it did confirm that significant adverse effects were present when theophylline was used.8
Of only four trials considered suitable for the meta-analysis, two examined treatment effects over 2 hours in the emergency room, one over 3 days in hospital and one, published only as an abstract, gave oral theophylline and evaluated its effect on patients still hospitalised after 48 hours.9–12 All trials were relatively small, with the best designed underpowered to exclude a treatment effect.9 Two of the studies suggested additional benefits of treatment, either in preventing hospitalisation or reducing subsequent relapse rate, but these findings were inconsistent.10,11
Given the limited data available, we hypothesised that intravenous aminophylline would not change post-bronchodilator lung function or the rate of symptom recovery in patients admitted to hospital with COPD exacerbations, and would not reduce the time to discharge or the subsequent relapse rate. To test these hypotheses we conducted a prospective, double blind, randomised, parallel group trial comparing intravenous aminophylline and placebo given from the time of hospital presentation and followed throughout the admission and, where possible, until 6 weeks after discharge.
METHODS
Patients
Patients with a clinical diagnosis of COPD5 presenting to the emergency department of University Hospital Aintree were considered eligible if they complained of increased breathlessness and two or more of the following symptoms for at least 24 hours: increased cough frequency or severity, increased sputum volume or purulence, increased wheeze. Patients were aged 40–80 years with a smoking history of at least 20 pack years, an initial forced expiratory volume in 1 second (FEV1) of <70% predicted, and FEV1/forced vital capacity (FVC) ratio of <70% predicted for age.
Patients with a clinical history of asthma or atopy, uncontrolled cardiac disease, advanced malignancy, clinical or radiological evidence of pneumonia, pneumothorax, or chest wall deformity were excluded. In addition, those with an arterial blood pH below 7.32 were excluded to ensure that the use of non-invasive ventilation was not a confounding factor when analysing the data. Patients with a contraindication to aminophylline, corticosteroids, β agonists, or anticholinergics were also excluded.
The study protocol was approved by the South Sefton research ethics committee and informed consent was obtained from all patients before study entry.
Study design
One investigator (ND) took a detailed medical history and examined patients within 4 hours of hospitalisation. On admission, blood was taken for a full blood count, including absolute eosinophil count. An arterial blood sample was taken, with patients breathing room air whenever possible, for blood gas analysis; this was repeated after 2 hours of treatment. The serum theophylline level was measured if the patient was receiving an oral theophylline preparation (Olympus turbidometric assay; lower limit <5 μmol/l, the curve is linear to 160 µmol/l; normal range 55–110 µmol/l). Sputum was collected, if produced, for microscopy, culture, and sensitivity. A breathlessness severity score at the time of admission was recorded using both the modified Borg category scale and a 100 mm visual analogue scale on which patients were asked to score their condition between 0 (no shortness of breath) and 100 (shortness of breath as bad as can be). Post-bronchodilator spirometric parameters were recorded using a dry bellows spirometer (Vitalograph Model 2150, Buckingham, UK) to American Thoracic Society standards.13 At least three forced expiratory manoeuvres were obtained on each occasion until two were within 5%. Data are expressed relative to the European Steel and Coal Company predicted values. All patients were treated with both a nebulised β agonist (salbutamol 5 mg) and an anticholinergic (ipratropium 500 μg) every 6 hours, controlled oxygen therapy, intravenous or oral antibiotics at the physician’s discretion, and oral prednisolone 30 mg daily for 14 days.
Patients were randomly assigned to treatment with intravenous aminophylline or saline; the study drug (which was identically packaged) was diluted in saline to a concentration of 1 mg/ml and a loading dose of 5 mg/kg body weight was given over 30 minutes. Subsequently, infusion at a rate of 0.5 mg/kg body weight/hour was continued until the physician in charge of the patient (who was not a study investigator) felt it appropriate to discontinue treatment because of clinical improvement or adverse effect. The placebo was given in the same manner so that a similar volume of fluid was infused. If the patient was taking an oral theophylline preparation before admission, the loading dose was omitted and the oral preparation was discontinued. Randomisation was performed using a computer generated random number table. Packages of treatment were numbered in advance and used sequentially.
Blood was taken on day 1 of the study for measurement of serum theophylline levels. The result was sent to another team member (not an investigator) who issued dummy results where appropriate to maintain the blinding. The rate of infusion was adjusted as appropriate and serum theophylline levels were rechecked as needed. All patients, investigators, and other hospital staff were masked to treatment status throughout the study.
Further assessments were carried out at 12 hours and then daily for 5 days (unless discharged from hospital before this time) and again on the day the patient was thought fit for discharge. At each assessment, made 30 minutes after the bronchodilator was given, spirometric tests were repeated; a daily symptom score was recorded by assessing whether patients felt the same, better, or worse overall compared with the previous day; and a Borg score for breathlessness, measurements of respiratory rate, and percentage oxygen saturation were recorded. In addition, we asked about possible side effects of aminophylline (headache, nausea, and palpitations).
Patients could be withdrawn at any time if they or their physician (not an investigator) felt clinical improvement was unsatisfactory, and patients were automatically withdrawn if the arterial pH fell below 7.32. The patients’ physicians decided when they were medically fit for discharge, and this date was used in the study analysis. At discharge, spirometric tests and the visual analogue breathlessness score were repeated, a St George’s Respiratory Questionnaire was completed to assess the patients’ health status,14 and an assessment was made by the investigator as to whether the study treatment had been helpful.
Patients were reviewed 6 weeks after discharge with repeated spirometric testing after 5 mg nebulised salbutamol and the St George’s Respiratory Questionnaire. Data were collected about any treatment changes since discharge and whether there had been any further exacerbations. The 6 week visit was postponed if the patient had had a further exacerbation. Patients not returning were contacted by telephone and their vital status and exacerbation history confirmed.
The study funders had no part in the design, the running of the study, or the data analysis.
Statistical analysis
The primary end point was the change in post-bronchodilator FEV1 over the first 5 days following admission; secondary end points were changes in breathlessness as measured by the Borg and visual analogue scales, changes in arterial blood gases from baseline to 2 hours after treatment, changes in FVC, and length of hospital stay.
Given the hazards of theophylline treatment, we decided that it could only be justified if it was accompanied by a clinically important improvement in FEV1, equivalent to an improvement of 200 ml within the study period. We calculated that a sample size of 37 in each group would give 80% power to detect a difference of 200 ml in FEV1 between aminophylline and placebo, assuming that the common standard deviation is 300 ml using a two group t test with a 5% two sided significance level. Hence, we aimed to recruit 40 patients per group. All data were analysed using SPSS Version 11. Student’s t tests, ANCOVA, and ANOVA were used to compare normally distributed data. Data are expressed as mean and 95% confidence intervals (CI). The assumptions of the model were checked by inspection of the residuals.
RESULTS
Of 320 patients screened for the study, 132 met the inclusion criteria (fig 1). The most common reason for exclusion was breathlessness for reasons other than COPD. Thirty nine patients received active treatment and 41 placebo. Of the 65 sputum specimens at admission, 43 were sterile, 10 grew Haemophilus influenzae, eight Streptococcus pneumoniae, and the remainder a range of other organisms. The presence of a positive sputum culture was unrelated to the subsequent progress. There were two deaths during hospital admission in the placebo group, both occurring after study medication was stopped due to clinical improvement. In one case the patient subsequently deteriorated and received aminophylline out of the clinical trial setting and also non-invasive ventilation. The other subject died suddenly on day 3 from a myocardial infarction. In addition, two further subjects in the aminophylline group were given unblinded aminophylline due to clinical deterioration the day after the study drug was discontinued.

CONSORT diagram indicating progress of patients through the clinical trial.
The baseline characteristics of the two groups are shown in table 1. There were no significant differences between the groups.
Baseline characteristics of the two groups on admission
In the aminophylline group the mean theophylline level of the eight patients taking oral theophylline was 88 µmol/l (95% CI 72 to 104) compared with 61 µmol/l (95% CI 47 to 75) in the 11 patients taking theophylline in the placebo group.
The mean number of days the study drug was given was 1.7 (95% CI 1.3 to 2.1) in the aminophylline group and 2.3 (95% CI 1.0 to 2.0) in the placebo group (p = 0.058). The mean theophylline level on the day following admission in the aminophylline group was 73.4 µmol/l (95% CI 62.9 to 83.9) while in the placebo group it was 2.5 µmol/l (95% CI 0.5 to 4.5); in the 11 subjects receiving placebo who used oral theophylline the mean level was 9.0 µmol/l (95% CI 3.3 to 14.7).
From admission to discharge the FEV1 increased more with placebo than with aminophylline treatment (p = 0.048). When analysed over the first 5 days after admission with FEV1 or FVC on admission (as appropriate) as a covariate, there was no significant difference in the change in FEV1 or FVC between the two groups (p = 0.49); this was also true for the first 24 hours (p = 0.46) when all but two subjects (both in the aminophylline group) remained on study medication (fig 2). Prior use of theophylline did not affect these results.
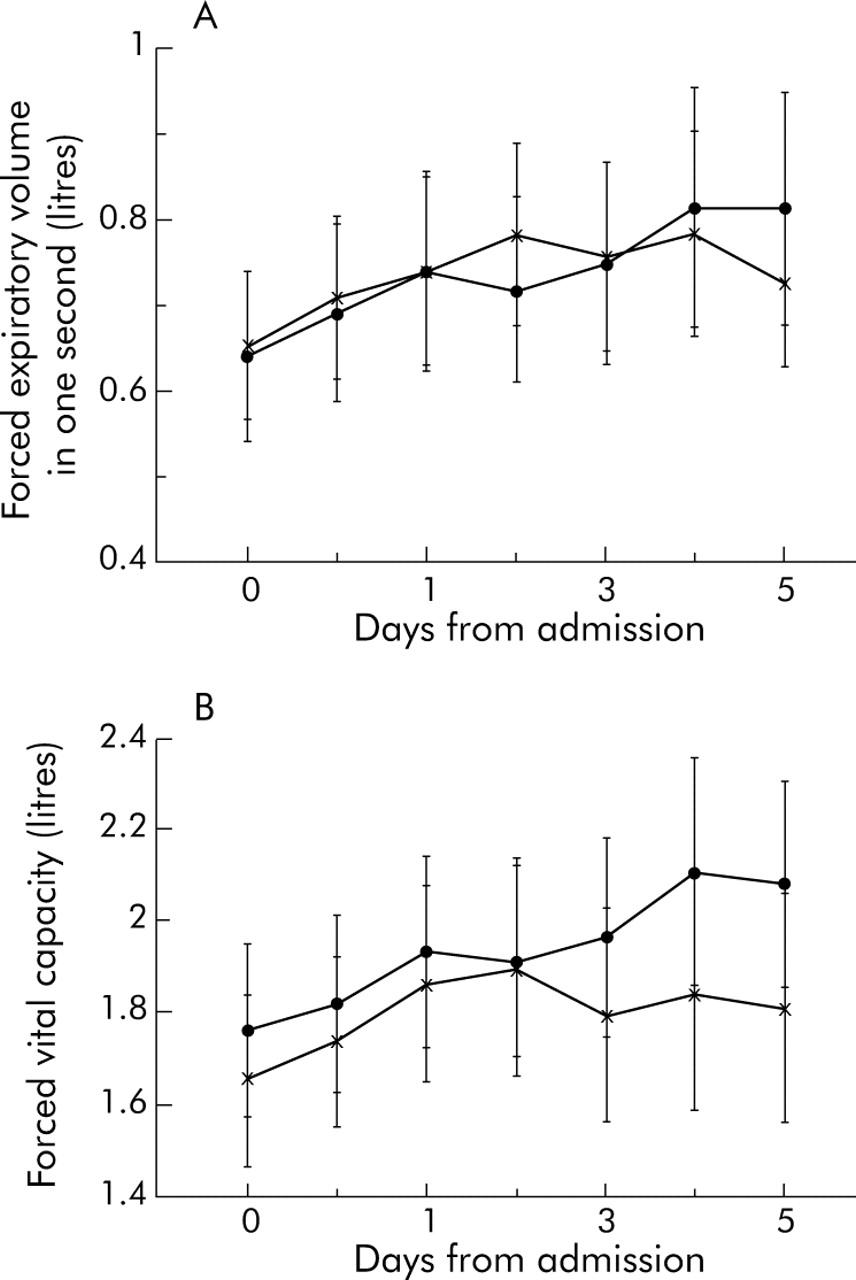
Mean and 95% confidence intervals of post-bronchodilator (A) forced expiratory volume in 1 second and (B) forced vital capacity during the trial. Aminophylline treatment indicated by crosses and placebo by closed circles.
Arterial blood gas data were available in all subjects on admission and 2 hours later. In 70 patients both the admission and 2 hour samples were taken breathing room air (table 2). There was a significant difference in the change in arterial pH and Paco2 over the first 2 hours of treatment between the groups, with the aminophylline group showing a larger increase in pH (p = 0.001) and a larger fall in Paco2 (p = 0.01) which was not influenced by prior theophylline use. The change in respiratory rate did not differ from admission to discharge between groups (from 23.9 (95% CI 22.0 to 25.8) to 22.2 (95% CI 20.4 to 24.0) in the placebo group and from 24.8 (95% CI 23.1 to 26.5) to 23.6 (95% CI 22.2 to 25.0) in the aminophylline group), nor was there a difference in the change in symptom score (table 3). Blinded evaluation of treatment efficacy could not distinguish between placebo (helpful in 42%) and the active drug (helpful in 49%; p = 0.56).
Arterial blood gas tensions breathing air before and 2 hours after treatment
Changes in patient and physician reported symptoms during the course of hospital admission
The mean length of hospital stay analysed on an intention to treat basis for all 78 patients who survived was 7.7 days (95% CI 6.8 to 8.6). In the aminophylline group the mean length of stay in hospital was 7.1 days (95% CI 5.9 to 8.3) compared with 8.2 days (95% CI 7.0 to 9.4) for the placebo group (p = 0.19, fig 3).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier plot of the proportion of patients remaining in hospital in the two treatment groups.
More patients in the aminophylline group complained of nausea than in the placebo group (46% v 22%; χ2 <0.05). In the aminophylline group 10 patients complained of palpitations and 14 of headache compared with seven and 13 patients respectively in the placebo group (not significant). The study drug was stopped in 10 subjects because of possible side effects, six of whom were in the aminophylline group. Four patients reported severe nausea (all on day 1) but in only one case of nausea was the serum theophylline level supratherapeutic. One patient had symptomatic sinus tachycardia (after 1 hour). In one additional patient the drug was stopped after a seizure at 1.5 hours. The drug level was in the therapeutic range at the time of the seizure (53 µmol/l) and the fit was later attributed on clinical grounds to alcohol withdrawal. In the placebo group three patients had severe nausea causing the drug to be discontinued (two on day 1 and one on day 4 who also complained of diarrhoea). The drug was stopped on day 8 in the remaining patient following a seizure; this subject also had epilepsy. Data were included for analysis in all these patients on an intention to treat basis.
At 6 weeks after discharge 28 patients had experienced a further exacerbation requiring treatment or hospitalisation, nine of whom died. Neither mortality nor further exacerbations were related to the initial treatment allocation, nor did spirometric parameters or health status differ between treatments in those assessed at 6 weeks.
DISCUSSION
This is the first adequately powered trial to study whether adding intravenous aminophylline to conventional treatment benefits patients with COPD exacerbations, either acutely or following discharge from hospital. We found no evidence of any clinical or physiological benefit during the hospital stay, nor did the use of intravenous aminophylline shorten hospitalisation significantly or influence subsequent progress.
Our patient groups were well matched at admission. All received identical medical treatment and trial treatment was blinded to the investigator by the use of dummy theophylline levels in those receiving placebo. The magnitude of change in lung function was similar to that reported previously by us during the recovery from an exacerbation.2 The lack of any statistical or clinically significant difference in FEV1 between treatment arms, either early or late in the course of the illness, is in keeping with the data from Rice et al9 who studied similar patients, and it suggests that aminophylline is not providing additional bronchodilatation beyond that achieved with high dose nebulised treatments. Although it has been proposed that theophylline has an effect on more peripheral airways in stable disease,15 we saw no difference in FVC between our treatment groups and the post-bronchodilator FVC showed smaller changes with aminophylline than with placebo.
Prior theophylline use might have confounded these effects, but this was equally distributed between the treatment limbs and the theophylline level was almost undetectable 24 hours after admission in those receiving placebo. Restriction of the analysis to the 61 patients who had not received prior treatment with theophylline did not change the spirometric outcomes. However, a different picture was seen with the early changes in arterial blood gas tensions; aminophylline treated patients breathing air had a lower paco2 and a slightly higher pH at 12 hours than those receiving placebo, a change that was more obvious in those who had not received prior treatment with theophylline. This is in keeping with the known effect of aminophylline as a ventilatory stimulant, probably due to increases in central nervous system hypoxaemia.16,17 However, these changes were clinically unimportant in our patients who were selected as having non-acidotic exacerbations. Whether this effect would benefit patients with hypercapnic respiratory failure remains to be tested, although current evidence would suggest that the use of aminophylline would best be seen as an adjunct to non-invasive ventilatory support.18
The change in breathlessness (whether assessed by the Borg or visual analogue scale) and the rate of resolution of symptoms were not influenced by aminophylline treatment. Treatment was continued for approximately 30–50 hours with no sign of a clinical or physiological difference in favour of aminophylline as treatment progressed. The decision to stop treatment, which was made by clinicians unaware of the treatment allocation, was similar in the two groups and the clinical evaluation of the success of the treatment was likewise randomly distributed. This latter helps to explain the individual clinician’s belief in the value of this treatment, as it is possible to attribute benefit to treatment when improvement has been spontaneous. Similar concerns also affect the perception of side effects with withdrawal due to potential theophylline related toxicity being as common in placebo treated patients as in those who received the active drug.
The theophylline concentration achieved during active treatment was below the mid point of the therapeutic range, although in no case was it subtherapeutic. It is possible that a higher concentration might have improved lung function, but only at the risk of greater toxicity. The relatively “low” toxicity in our study may reflect our careful monitoring of theophylline use but, despite this, several patients developed nausea and the risk of uncontrolled aminophylline treatment has been well documented elsewhere.8
In conclusion, our data indicate that the addition of intravenous aminophylline to nebulised bronchodilators and oral corticosteroids in the management of non-acidotic COPD patients cannot be recommended as it confers no clear benefit and potentially increases both the risk of side effects and the complexity of management.
Acknowledgments
The authors thank all patients, consultants, and staff who participated in the study. Theophylline levels were measured by the Biochemistry Department at University Hospital Aintree. Dummy theophylline levels were supplied by Deirdre Frost (research nurse).
REFERENCES
Footnotes
-
Published Online First 6 June 2005
-
The study was supported by the EU CARED project (ND) and an ERS training fellowship (FD).
-
All authors declare no conflict of interest.
-
ND, PW and FD assessed the patients and collected the data, ND conducting all the final reviews. ND undertook the data analysis and wrote the manuscript together with PMAC and LD who originally developed the study protocol.
Linked Articles
- Airwaves