Article Text

Abstract
Rationale Strength training and neuromuscular electrical stimulation (NMES) improve lower-limb muscle function in dyspnoeic individuals with chronic obstructive pulmonary disease (COPD). However, high-frequency NMES (HF-NMES) and strength training have never been compared head-to-head; and effects of low-frequency NMES (LF-NMES) have never been studied in COPD. Therefore, the optimal training modality to improve lower-limb muscle function, exercise performance and other patient-related outcomes in individuals with severe COPD remains unknown.
Objectives To study prospectively the efficacy of HF-NMES (75 Hz), LF-NMES (15 Hz) or strength training in severely dyspnoeic individuals with COPD with quadriceps muscle weakness at baseline.
Methods 120 individuals with COPD (FEV1: 33±1% predicted, men: 52%, age: 64.8±0.8 years) were randomised to HF-NMES, LF-NMES or strength training as part of a comprehensive inpatient pulmonary rehabilitation programme. No treadmill walking or stationary cycling was provided.
Measurements and main results Groups were comparable at baseline. Quadriceps muscle strength increased after HF-NMES (+10.8 Newton-metre (Nm)) or strength training (+6.1 Nm; both p<0.01), but not after LF-NMES (+1.4 Nm; p=0.43). Quadriceps muscle endurance, exercise performance, lower-limb fat-free mass, exercise-induced symptoms of dyspnoea and fatigue improved significantly compared with baseline after HF-NMES, LF-NMES or strength training. The increase in quadriceps muscle strength and muscle endurance was greater after HF-NMES than after LF-NMES.
Conclusions HF-NMES is equally effective as strength training in severely dyspnoeic individuals with COPD and muscle weakness in strengthening the quadriceps muscles and thus may be a good alternative in this particular group of patients. HF-NMES, LF-NMES and strength training were effective in improving exercise performance in severely dyspnoeic individuals with COPD and quadriceps weakness.
Trial registration NTR2322
- COPD Pathology
- Exercise
- Pulmonary Rehabilitation
Statistics from Altmetric.com
Introduction
Lower-limb muscle dysfunction is a prominent extrapulmonary feature in individuals with moderate-to-very severe chronic obstructive pulmonary disease (COPD).1 It is related to exercise intolerance, increased healthcare use and mortality.1 Physical inactivity is most probably its main underlying cause.1 Therefore, exercise-based pulmonary rehabilitation should be part of the integrated care of individuals with COPD.2
Lower-limb muscle dysfunction occurs frequently in severely dyspnoeic individuals with COPD.3 Therefore, there is great interest in effective rehabilitative modalities which do not evoke severe dyspnoea, such as strength training or transcutaneous neuromuscular electrical stimulation (NMES).2 Indeed, the metabolic load on the impaired respiratory system is relatively low during strength training or NMES in individuals with COPD.4 ,5
Strength training or high-frequency NMES (HF-NMES; stimulation frequencies ≥50 Hz) increases quadriceps muscle function, exercise capacity and health status as compared with a non-exercise control group or sham NMES in individuals with COPD, respectively.6 ,7 To date, a head-to-head comparison of strength training and HF-NMES has not been done in severely dyspnoeic individuals with COPD. Therefore, it remains unknown whether, and to what extent, these training modalities may have similar effects in individuals with COPD. A priori, no differences were expected between the groups.
Low-frequency NMES (LF-NMES, at 15 Hz) of lower-limb muscles increased exercise capacity in individuals with chronic heart failure.8 To date, the effects of LF-NMES at 15 Hz have not been studied in individuals with COPD. However, it seems reasonable to hypothesise that quadriceps muscle endurance will improve to a greater extent after LF-NMES,8 ,9 while quadriceps muscle strength will improve to a greater extent after HF-NMES.10
The aim of the DICES (Dyspnoeic Individuals with COPD: Electrical stimulation or Strength training) trial was to study the efficacy of HF-NMES, LF-NMES or strength training in severely dyspnoeic individuals with COPD with quadriceps muscle weakness at baseline.
Methods
Please see online supplementary data for all details.
Participants
Individuals with COPD referred for a pulmonary rehabilitation programme at the Centre of Expertise for Chronic Organ Failure (CIRO+) were screened for eligibility.11 Inclusion criteria were primary diagnosis of COPD; baseline modified Medical Research Council (MRC) dyspnoea grade 3 or 4 and quadriceps weakness (peak torque ≤80% predicted).12 Exclusion criteria were neuromuscular diseases; joint disorders in hip, leg and/or knee; metal implants in hip, leg and/or knee; cardiac pacemaker or internal cardiac defibrillator and/or outpatient pulmonary rehabilitation programme.
Design and procedures
A prospective, single-blind, randomised controlled trial was designed which was approved by the medical ethical committee of the Maastricht University Medical Centre+ (MEC 09-3-072). The DICES trial was registered at http://www.trialregister.nl (NTR2322) before enrolment of the first subject. All participants gave written informed consent to participate. Some baseline findings of the DICES trial have been published.13
Interventions
Participants were randomly assigned to HF-NMES, LF-NMES or strength training (8 weeks, twice a day, five times a week). All sessions were supervised by a physiotherapist. Symptom scores for dyspnoea, fatigue and muscle pain were assessed before and directly after each session.14 The DICES trial was part of a regular 8-week inpatient pulmonary rehabilitation programme, including also non-exercising components such as occupational therapy, relaxation therapy, exacerbation management strategies, educational sessions and psychosocial counselling.2 The interdisciplinary treatment was comparable among the groups. None of the participants underwent treadmill walking or stationary ergometry cycling.
NMES protocols
Quadriceps and calf muscles of both legs were stimulated electrically with a portable battery-operated electrical stimulator, using eight carbon-rubber electrodes (Tensmed S84, Enraf-Nonius, Rotterdam, the Netherlands) (see online supplementary figure E1).5 After a continuous 3-min warm-up at 5 Hz, intensity was adjusted to individual toleration during each 18-min session. The frequencies used were 75 Hz (HF-NMES) or 15 Hz (LF-NMES).5
Strength training
Strength training consisted of bilateral leg extension and bilateral leg press exercises (Technogym SpA, Gambettola, Italy).15 Both exercises started at 70% of one-repetition maximum, four sets of eight repetitions for each exercise with at least 2 min of recovery between each set. The training load was set to increase by 5% every 2 weeks.15
Outcomes
Primary outcome
The primary outcome was the change in isokinetic quadriceps muscle function (ie, peak muscle strength and endurance) using a Biodex (Biodex System 4 Pro, Biodex Medical Systems, Inc, New York, USA).16 Participants performed 30 sequential volitional maximal contractions at an angular velocity of 90°/s, while seated upright and with the hip joint in 90° of flexion. Quadriceps muscle strength was defined as the highest peak torque (Newton-metre (Nm)). Quadriceps muscle endurance was defined as the total amount of delivered work (Joules (J)) during the set of 30 repetitions.16 To minimise learning effects, the measurement was performed twice at the initial assessment. Best values were used for analyses.
Secondary outcomes
Functional exercise performance was measured with the 6-min walk test (6MWT), including a practice walk at initial assessment.17 The best value was used for further analyses. The constant work-rate cycling endurance test (CWRT, expressed in seconds) was performed at 75% of the measured peak cycling work rate.18 Dyspnoea and fatigue were assessed before and after exercise tests and at isotime during the postintervention CWRT. Anxiety and depression were assessed using the Hospital Anxiety Depression Scale.19 Disease-specific health status was measured using the St George’s Respiratory Questionnaire (SGRQ).20 The Canadian Occupational Performance Measure (COPM), a semistructured interview performed by an occupational therapist, was used to assess problematic activities of daily life (ADLs),21 and has been shown to be reliable in individuals with COPD.22 Whole-body dual-energy x-ray absorptiometry scan was used to assess body mass index and fat-free mass index (FFMI).23 A modified MRC dyspnoea scale was used to assess dyspnoea.24 In addition, age, sex, height, weight, comorbidities,25 pulmonary function parameters and arterial blood gases were collected at the initial assessment.13
Sample size calculation, randomisation, blinding and statistics
The DICES trial was powered to detect a significant difference in the change in maximal quadriceps strength between HF-NMES and LF-NMES of 9.2 kg on average.26 Each intervention group needed to have 36 individuals with COPD. Adjusting for drop out and withdrawals, we aimed for a minimum of 40 individuals in each intervention group.
A randomisation schedule was generated by the computer for participants with and without the use of long-term oxygen treatment; and with or without hospitalisation for a COPD exacerbation within <3 months of enrolment. The sequence was concealed. Analyses were performed using SPSS for Windows, V.17.0.1 (SPSS, Inc, Chicago, Illinois, USA). Differences within groups were analysed using paired t tests or Wilcoxon signed rank test. Groups were compared using one-way analysis of variance, χ2 test, Fisher's exact test or Kruskal–Wallis one-way analysis of variance, as appropriate. The Bonferroni t test was used as post hoc test. Correlation analyses were done using Pearson's or Spearman's correlations. The level of significance was set at ≤0.05.
Results
Participants’ flow
Between September 2010 and November 2012, 120 individuals with COPD were included in the DICES trial (HF-NMES: n=41; LF-NMES: n=39; strength training: n=40). Ninety-one individuals (75.8%) were followed up at 8 weeks. The main reasons for dropping out were severe health problems, including hospital admission. Dropout rates were similar among intervention groups (figure 1).

Flow diagram DICES trial (Dyspnoeic Individuals with COPD: Electrical stimulation or Strength training). CIRO, Centre of Expertise for Chronic Organ Failure; HF-NMES, high-frequency transcutaneous neuromuscular electrical stimulation; LF-NMES, low-frequency transcutaneous neuromuscular electrical stimulation.
Baseline characteristics
Participants generally had severe to very severe COPD, a poor diffusing capacity, explicit quadriceps muscle weakness, very severe dyspnoea, a poor functional and peak exercise performance and a poor health status (table 1). Participants used 10±1 types of medications (see online supplementary table E1) and had 3.2±0.1 objectified comorbidities (see online supplementary figure E2). The 29 individuals who dropped out and the 91 participants who completed the 8-week intervention had similar baseline characteristics (see online supplementary table E2).
General characteristics
Course of the 8-week NMES or strength training
The 91 participants who completed the programme attended 76±3 HF-NMES sessions, 74±1 LF-NMES sessions, or 68±2 strength training sessions (both NMES interventions vs strength training, p<0.001). Exacerbations requiring antibiotics and/or corticosteroid treatment occurred frequently during all three interventions: 58% of the HF-NMES participants; 41% of the LF-NMES participants and 41% of the strength training participants (p=0.254). During exacerbations of COPD which did not require hospital admission, NMES sessions (HF and LF) were continued. Strength training sessions were not always possible during exacerbations. The mean numbers of training sessions did not differ between the patients with and without one or more exacerbations (p=0.564).
HF/LF-NMES current intensities and strength training loads increased significantly over time (figure 2). All training modalities were safe. No side effects, such as acute dyspnoea or muscle pain, were reported (see online supplementary figure E3 for all details).

Course in NMES pulse amplitude and strength training load. Data are shown as mean±SEM. HF-NMES, high-frequency transcutaneous neuromuscular electrical stimulation; LF-NMES, low-frequency transcutaneous neuromuscular electrical stimulation.
Efficacy
Quadriceps muscle function
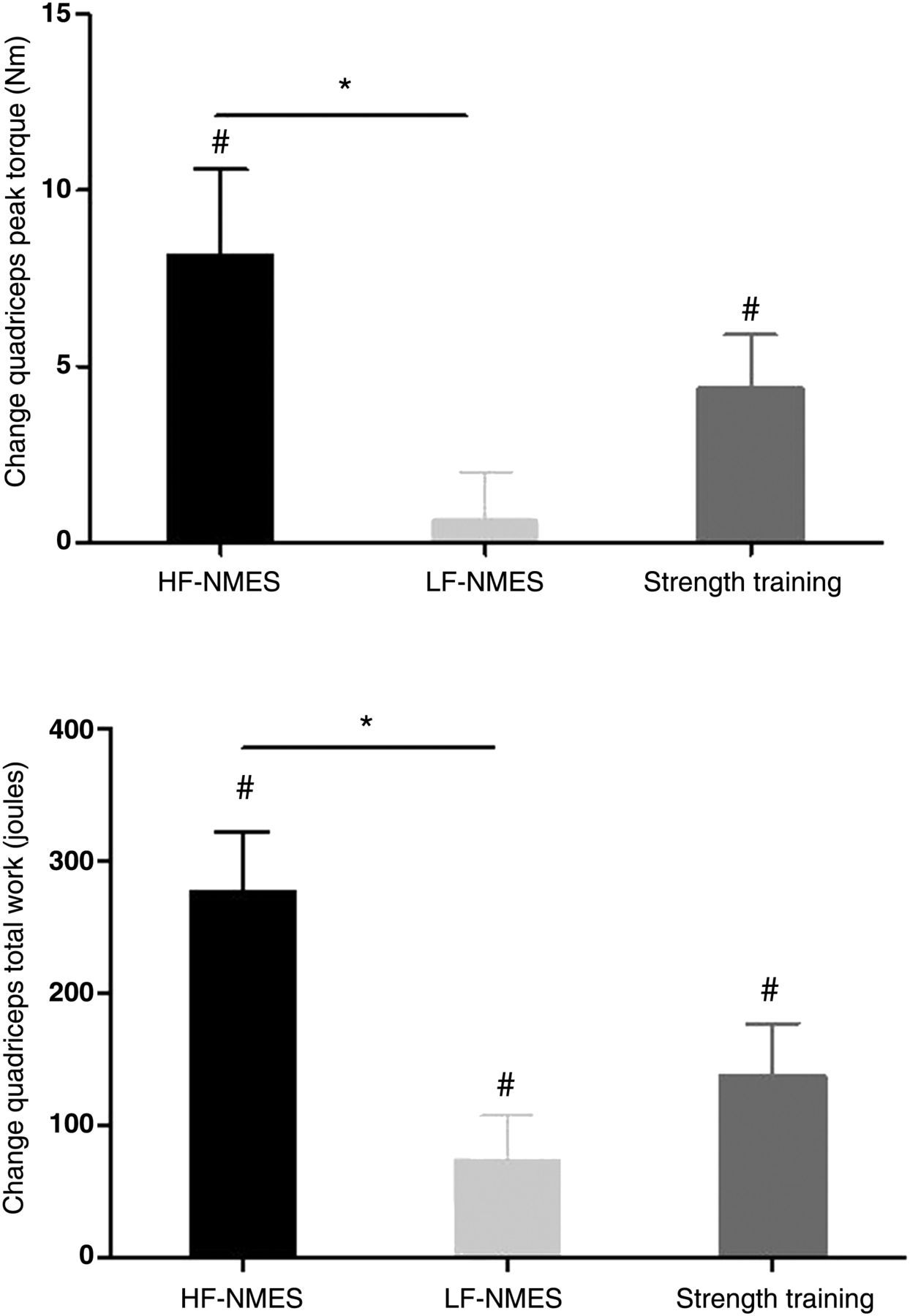
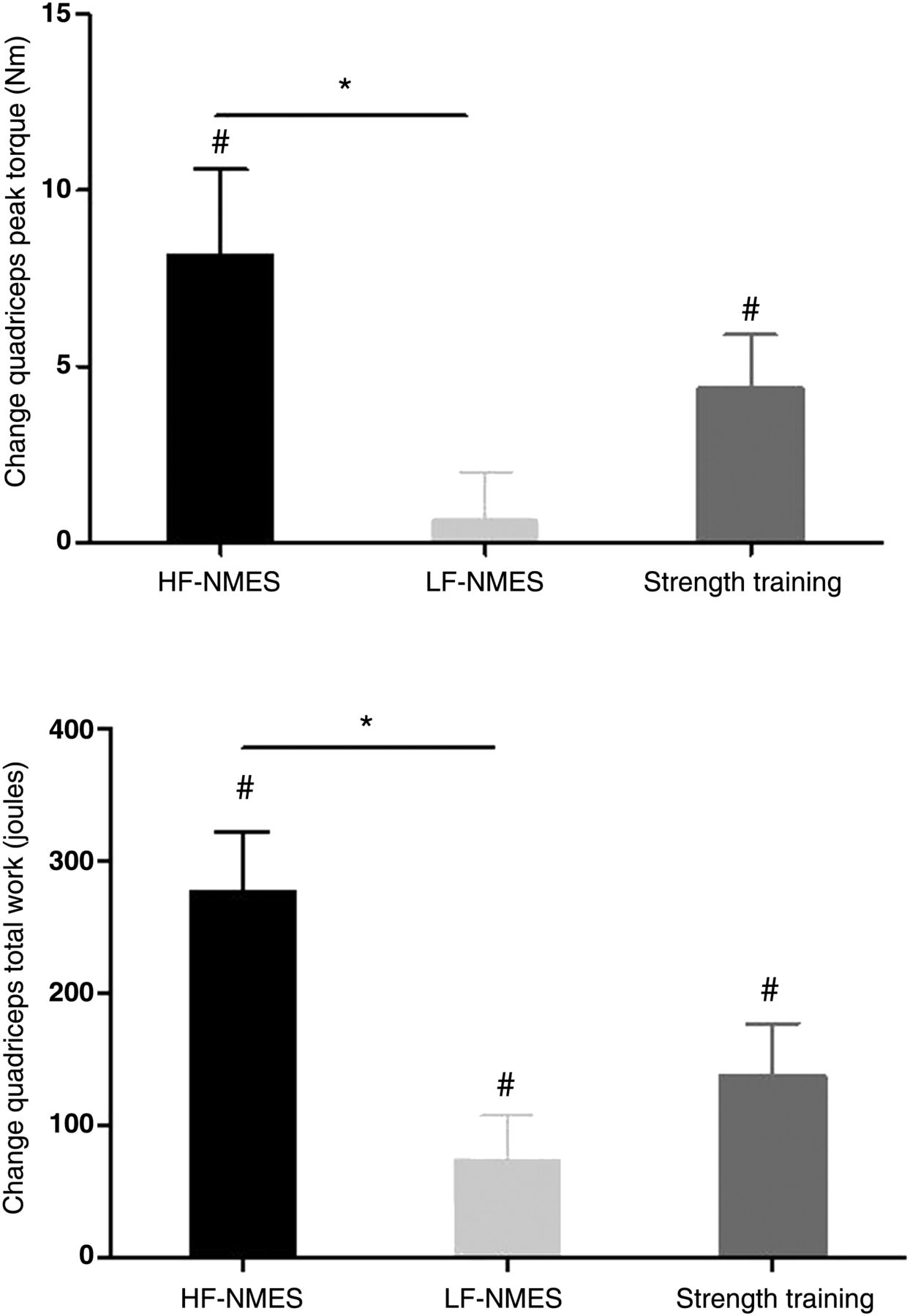
Isokinetic quadriceps peak torque increased significantly after HF-NMES (10.8±2.9 Nm; p<0.01) or strength training (6.1±2.0 Nm; p<0.01), but not after LF-NMES (1.4±1.8 Nm; p=0.43). Improvement in isokinetic quadriceps peak torque was significantly higher after HF-NMES compared with LF-NMES (p=0.01; figure 3A). Isokinetic total work increased significantly in all groups (HF-NMES: 285±51 J; LF-NMES: 101±45 J; strength training: 192±51 J; all p<0.03). Again, the improvement after HF-NMES was significantly higher than with LF-NMES (p=0.03; figure 3B). Gains in peak muscle strength correlated with the increase in muscle endurance (HF-NMES: r=0.689; LF-NMES: r=0.581 and strength training: r=0.689, all p<0.001).
{kind=link}
{kind=link}
{kind=link}
Change in quadriceps muscle strength and endurance. Data are shown as mean±SEM. *p≤0.05; #p≤0.05 compared with baseline. HF-NMES, high-frequency transcutaneous neuromuscular electrical stimulation; LF-NMES, low-frequency transcutaneous neuromuscular electrical stimulation.
Six-minute walk test
Six-minute walk distance improved in all groups (HF-NMES: 66±14 m; LF-NMES: 51±15 m; strength training: 29±12 m; all p<0.03; no differences between groups). Interestingly, symptoms at the end of the 6MWT were significantly lower than baseline after HF-NMES (dyspnoea: 6.9±0.4 vs 5.7±0.4 points; fatigue: 5.2±0.5 vs 3.4±0.4 points; both p<0.014) or LF-NMES (dyspnoea: 6.4±0.4 vs 5.4±0.5 points; fatigue: 4.9±0.5 vs 2.8±0.5 points; both p<0.032). Symptoms at the end of the 6-min walk test remained unchanged after strength training (dyspnoea: 5.6±0.4 vs 5.2±0.4 points; fatigue: 4.1±0.5 vs 3.3±0.5 points; both p>0.11).
Constant work-rate test
Endurance time during the CWRT improved in all groups (HF-NMES: 171±58 s; LF-NMES: 167±46 s; strength training: 69±30 s; all p<0.03; no differences between groups). At isotime, symptoms of dyspnoea were lower after both NMES protocols, and fatigue was lower after all three interventions compared with the initial CWRT (HF-NMES: Δ dyspnoea isotime: −1.8±0.6 points (p=0.005), Δ fatigue isotime: −2.6±0.6 points (p<0.001); LF-NMES: −1.9±0.6 points (p=0.005) and −1.4±0.5 points (p=0.01), respectively; and strength training: 0.4±0.4 points (p=0.361), −1.7±0.5 points, (p=0.003), respectively. Moreover, symptoms of fatigue at the end of the CWRT were significantly lower than at baseline after HF-NMES (6.3±0.5 vs 4.7±0.6 points), LF-NMES (5.8±0.5 vs 5.0±0.6 points) or strength training (6.1±0.5 vs 4.8±0.5 points; all p<0.05). Symptoms of dyspnoea at the end of the cycle endurance test did not change (data not shown).
Body composition
Body mass index and FFMI did not change significantly compared with baseline in any of the groups. Lower-limb FFM increased in all groups (HF-NMES: 0.58±0.18 kg; LF-NMES: 0.44±0.18 kg; strength training: 0.37±0.13 kg; all p<0.03; no differences between groups).
Dyspnoea
Modified MRC dyspnoea scores improved in all groups (HF-NMES: −0.9±0.2 points; LF-NMES:
−0.7±0.2 points; strength training: −0.8±0.2 points; all p<0.005; no differences between groups).
Mood status
Symptoms of depression improved in all groups (HF-NMES: −1.8±0.6 points; LF-NMES: −2.2±0.5 points; strength training: −1.6±0.7 points; all p<0.04), while symptoms of anxiety only improved after LF-NMES (−1.8±0.6 points; p=0.004). Changes in symptoms of anxiety or depression were similar between groups (p>0.46).
Health status
Total SGRQ scores improved in all groups compared with baseline (HF-NMES: −10.2±2.4 points; LF-NMES: −10.5±3.0 points; strength training: −11.4±2.5 points; all p<0.003). Changes in health status scores were similar between groups (p=0.948). See online supplementary table E5 for the significant changes in the SGRQ domain scores.
Problematic activities of daily living (ADL)
COPM total scores for problematic ADL improved in all groups compared with baseline (HF-NMES: performance: 2.7±0.2 points, satisfaction: 3.5±0.2 points; LF-NMES: performance 2.5±0.2 points, satisfaction 2.9±0.3 points; strength training: performance 2.3±0.2 points, satisfaction 2.8±0.3 points; p<0.05), with no significant differences between groups (see online supplementary tables E6 and E7 for details).
Discussion
As far as we know, this is the first trial comparing the effects of HF-NMES, LF-NMES and strength training as the sole supervised muscle training modality during an 8-week pulmonary rehabilitation programme in severely dyspnoeic individuals with COPD and quadriceps weakness at baseline. Lower-limb muscle strength increased in the HF-NMES group and the strength training group compared with baseline. Exercise performance, exercise-induced symptoms of dyspnoea and fatigue improved significantly compared with baseline in all three lower-limb training modalities. Only the increase in isokinetic quadriceps muscle strength and endurance were higher after HF-NMES than after LF-NMES. Moreover, the DICES trial also showed that symptoms of depression, health status and problematic activities of daily living improved after an interdisciplinary pulmonary rehabilitation programme without treadmill walking or stationary cycling.
Lower-limb muscle function
Isokinetic quadriceps muscle strength improved after HF-NMES or strength training. This is in line with previous studies.6 ,7 Interestingly, no significant differences were found between HF-NMES and strength training. Therefore, HF-NMES may be a preferential muscle training modality in patients with COPD with severe dyspnoea and muscle weakness, as the metabolic load on the impaired cardiorespiratory system is significantly lower than with strength training.4 Moreover, HF-NMES recruits motor units in a non-selective, spatially fixed and temporally synchronous pattern,27 contrary to the activation order according to the size principle involving activation of the slower (lower force-producing) motor units before the faster (higher force-producing) units.28 In COPD, atrophy of fast-twitch muscle fibres is consistently reported.29 It can be hypothesised that at least some of these fibres can be trained by HF-NMES, whereas these fibres might otherwise be activated only by high-force voluntary efforts.30
As expected from studies in healthy subjects,31 quadriceps muscle strength did not improve after LF-NMES. Indeed, the change in isokinetic quadriceps muscle strength was significantly higher in the HF-NMES group than in the LF-NMES group. Comparable results were found in a study comparing HF-NMES (50 Hz) with LF-NMES (15 Hz) in healthy volunteers and in individuals with chronic heart failure.10 The above-mentioned results might be obtained because the increase in muscle strength is proportional to the stimulation frequency: higher frequencies produce higher torques, which probably result in a greater increase in muscle strength.32 Besides the peripheral pathway, HF-NMES can also produce muscle contractions by central recruitment through the electrically evoked sensory volley, in contrast to LF-NMES.33 During HF-NMES, the recruitment of motor units through central pathways can augment contractions generated through peripheral pathways, leading to the development of greater torques.34 While HF-NMES and LF-NMES had differential effects on muscle function in this study, the observed increase in lower-limb muscle mass was comparable, indicating that muscle dysfunction in COPD is not only related to the bulk of muscle.
Exercise performance
This trial shows that lower-limb muscle training modalities improve exercise performance significantly, while it is known that the load on the cardiorespiratory system is rather low.4 ,5 Indeed, the mean improvement in 6-min walk distance exceeded the minimal important differences of 25 m in all three intervention groups.35 Even though quadriceps muscle strength and endurance improved to a greater extent after HF-NMES than with LF-NMES, improvements in exercise performance were similar. This might be due to the fact that patients were still limited owing to their dyspnoea at the end of the exercise tests, while fatigue symptom scores were clearly lower at the end of the 6MWT or CWRT compared with baseline tests.
Dyspnoea, mood status, health status and problematic ADL
Both strength training and HF-NMES have a positive impact on health status in individuals with COPD.7 Unfortunately, the design of our study does not allow us to distinguish between the impact of the muscle training modalities and the non-exercising parts of the pulmonary rehabilitation programme. The significant improvements in mood, health and problematic ADLs, however, were very encouraging as clinically relevant thresholds were exceeded, which is also true for walking and/or cycling-based pulmonary rehabilitation programmes.2
Strengths and methodological considerations
The DICES trial has several strengths. This is the largest randomised controlled trial studying the efficacy of HF-NMES, LF-NMES or strength training in severely dyspnoeic individuals with COPD and a considerable number of comorbidities. The number of participants provided sufficient statistical power to detect possible differences in changes in isokinetic quadriceps muscle function between HF-NMES, LF-NMES and strength training. However, the DICES trial is probably underpowered to detect statistically significant differences between HF/LF-NMES and strength training for changes in exercise performance, which did exceed minimal important differences. Isokinetic quadriceps muscle function was assessed twice at the initial assessment to minimise a learning effect. Outcome assessors were blinded for group allocation. They were not (in)directly involved in the delivery of the interventions. This places greater credence on the results.36 Individuals randomly assigned to HF-NMES of LF-NMES were also blinded for the stimulation frequency applied. This is the first trial studying the efficacy of LF-NMES in individuals with COPD. All participants with baseline and outcome assessments were analysed, irrespective of the number of completed sessions or exacerbation treatment with antibiotics and/or corticosteroids during the intervention period.
The DICES trial also had some methodological limitations. The trial design did not include a control group, as strength training or HF-NMES had been proved to be beneficial compared with a non-exercise control group or sham NMES in individuals with COPD, respectively.6 ,7 ,37 Twenty-nine participants (24.2%) did not complete the DICES trial. Dropping out appeared to be random across the DICES study sample as baseline characteristics were similar between participants who did and did not undergo outcome assessment (see online supplementary table E2). We believe that the drop-out rates are acceptable, as the DICES sample consisted of severely dyspnoeic individuals with COPD, who had muscle weakness and multiple coexisting morbidities. Moreover, our drop-out rate is comparable to drop-out rates in peer-reviewed COPD strength training trials (range: 11–38%).6 The generalisability of our findings is limited owing to the strict inclusion and exclusion criteria. This approach, however, is in line with the philosophy of personalised medicine, in which healthcare is tailored to the individual patient or subgroups of patients.38
Conclusions
This study shows that HF-NMES is as effective as strength training in severely dyspnoeic individuals with COPD and quadriceps weakness in partially reversing quadriceps muscle dysfunction. HF-NMES may be a good alternative for strength training in this specific patient group. LF-NMES is not effective in improving muscle strength. HF-NMES, LF-NMES and strength training are effective training modalities, improving exercise performance, lower limb fat-free mass and health status in severely dyspnoeic individuals with COPD and quadriceps weakness.
Acknowledgments
The authors are grateful to the patients who volunteered for the DICES trial. We also thank Martijn Cuijpers and Martyna Renckens for their valuable help.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors Trial concept and design: MJHS, EFMW and MAS; acquisition of data: MJHS, JMLD, AWV; analysis and interpretation of data, drafting the article: MJHS, FMEF and MAS; revising it critically for important intellectual content and final approval of the version to be published: all authors. MJHS had full access to all trial data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
-
Funding Lung Foundation, Leusden, the Netherlands (grant 3.4.09.024); Weijerhorst Foundation, Maastricht, the Netherlands.
-
Competing interests None.
-
Ethics approval Medical ethical committee of the Maastricht University Medical Centre+, Maastricht, the Netherlands.
-
Provenance and peer review Not commissioned; externally peer reviewed.