Article Text

Abstract
Background Pleural infection is common, and has a >30% major morbidity and mortality—particularly when infection is caused by Gram-negative, Staphylococcus aureus or mixed aerobic pathogens. Standard pleural fluid culture is negative in ∼40% of cases. Culturing pleural fluid in blood culture bottles may increase microbial yield, and is cheap and easy to perform.
Objectives To determine whether inoculating pleural fluid into blood culture bottles increases the culture positivity of pleural infection over standard laboratory culture, and to assess the optimum volume of inoculum to introduce.
Methods 62 patients with pleural infection were enrolled. Pairs of aerobic and anaerobic blood culture bottles were inoculated at the bedside with 2, 5 or 10 ml of pleural fluid, and two pleural fluid specimens were sent for standard culture. Pleural fluid from nine control patients was cultured to test for ‘false-positive’ results.
Results The addition of blood culture bottle culture to standard culture increased the proportion of patients with identifiable pathogens by 20.8% (20/53 (37.7%) to 31/53 (58.5%) (difference 20.8%, 95% CI difference 8.9% to 20.8%, p<0.001)). The second standard culture did not similarly improve the culture positivity (19/49 (38.8%) to 22/49 (44.9%) (difference 6.1%, 95% CI difference −2.5% to 6.1%, p=0.08)). The culture inoculum volume did not influence bacterial isolation frequency. The control fluids were culture negative.
Conclusions Blood culture bottle culture of infected pleural fluid increases microbial yield when used in addition to standard culture. This technique should be part of routine care.
- Empyema
- pleural/aetiology
- pleural effusion
- culture media
- microbiological techniques/methods
- blood culture bottles
- bacterial infection
- pleural disease
Statistics from Altmetric.com
- Empyema
- pleural/aetiology
- pleural effusion
- culture media
- microbiological techniques/methods
- blood culture bottles
- bacterial infection
- pleural disease
Key messages
What is the key question?
Does inoculating infected pleural fluid into blood culture bottles at the bedside improve the culture positivity of pleural infection?
What is the bottom line?
Blood culture bottle culture of pleural fluid improves culture positivity of pleural infection when used in addition to standard laboratory culture.
Why read on?
This study demonstrates how the increase in microbiological yield from bottle culture of pleural fluid is not simply the result of repeating the culture process, it is not ‘oversensitive’ and culture positivity is maintained even with smaller inoculum volumes.
Introduction
Pleural infection is a major cause of morbidity or death, and its incidence continues to rise in adults and children.1–4
Identification of the infecting bacteria by culture of pleural fluid is important for clinical care. This is often unsuccessful, as conventional Gram stain and culture are negative in ∼40% of cases.2 These patients are treated with empirical antibiotics that cover the spectrum of likely pathogens, resulting in polypharmacy and its associated disadvantages. Anaerobic antibiotic treatment is frequently given empirically, as anaerobes are often implicated in this syndrome—although their pick-up rates by standard laboratory cultures are poor.5–7 More reliable culture methods for anaerobic bacteria could reduce the frequency with which this empirical treatment is given, if clinical confidence of the absence of anaerobic infection could be guaranteed.
Mortality is increased to ∼40% in cases of Gram negative, Staphylococcus aureus or mixed aerobic infection,8 9 and reliable identification of these groups would allow the targeting of early aggressive therapy (such as video-assisted thoracoscopic surgery (VATS) surgical drainage) to selected patients.
Inoculating pleural fluid into blood culture bottles at the bedside can potentially improve the yield of pleural fluid culture.10 11 Previous studies of this approach are small, not restricted to patients with pleural infection and have not had a control intervention—making it unclear whether this benefit is real and clinically valuable. However, initial results suggest clinically higher bacterial isolate rates.12–16 In other clinical settings, inoculation of peritoneal dialysate,14 17–19 peritoneal fluid20–22 and synovial fluid14 23 24 into culture bottles has been shown to be clinically useful.
This study assesses whether inoculating possibly infected pleural fluid into aerobic and anaerobic blood culture bottles identifies more bacteria than simply repeating standard laboratory culture (the control intervention). It also assesses the optimum volume of pleural fluid inoculum to be used in this approach.
Methods
This prospective study recruited 62 patients with suspected pleural infection and nine control patients from four centres in the UK—Oxford Radcliffe Hospitals Trust, Northampton General Hospital (Northampton), Southmead Hospital (Bristol) and the Royal Berkshire Hospital (Reading).
Patients with pleural infection
Sequential patients with potential pleural infection were identified at each centre and offered entry into the study if they fulfilled the inclusion criteria (box 1) which required written informed consent.
Clinical features of patients with pleural infection
Clinical presentation compatible with pleural infection
Pleural fluid requiring drainage which was either:
purulent
Gram stain or culture positive
pH <7.2 by blood gas machine analysis
Excess pleural fluid available after standard sampling
Following recruitment, patients were managed by the recruiting physicians according to local policy. Pleural fluid obtained at the time of diagnostic sampling was divided at the bedside as follows:
A 10 ml aliquot into a sterile container for standard Gram stain and culture at the recruiting hospital laboratory.
A 10 ml aliquot for repeat standard culture at a second laboratory (Royal Free Hospital, London, UK).
Pairs of aerobic and anaerobic blood culture bottles (BACTEC PLUS, Becton Dickinson, Sparks, Maryland, USA. Soybean-casein digest broth 2.75% w/v) were inoculated with either 2, 5 or 10 ml of pleural fluid for culture at the Royal Free Hospital.
Venous blood cultures were performed at each centre at the time of recruitment.
Sixty-two patients were enrolled in the study, 57 of which were included in the final analysis. Five patients were withdrawn—four had insufficient data and one was subsequently diagnosed with Mycobacterium tuberculosis, where this diagnostic strategy is inappropriate.
Control patients―patients without pleural infection
Control patients with pleural effusions secondary to heart failure or malignancy were offered entry into the study if they fulfilled the inclusion criteria (box 2). All of these patients were recruited at the Oxford Radcliffe Hospitals Trust during investigation and/or management of a pleural effusion of non-infective aetiology.
Clinical features of patients without pleural infection
Heart failure patients
Clinical presentation compatible with heart failure and not infection
Pleural effusion present requiring drainage
Transudative pleural effusion (protein <30 g/dl, or pleural fluid:plasma lactate dehydrogenase (LDH) ratio <2/3), with a pH >7.2
Excess pleural fluid available after standard sampling
Patients with malignant effusions
Proven malignant effusion requiring drainage
Pleural fluid biochemistry supporting a non-infected effusion (pH >7.3, glucose >2.2 mmol/l and LDH <1000 IU/l)
No clinical features of infection or raised temperature >37.5°C and/or venous blood C-reactive protein >20 mg/l
Excess pleural fluid available after standard sampling
Pleural fluid obtained at sampling was divided by the same method as for patients with pleural infection, with the exception that only one pair of blood culture bottles was sent (each with 10 ml inoculum volume).
Sample handling and laboratory methods
Samples were transferred to a central analysis centre (Royal Free Hospital) by urgent courier. The standard sample was centrifuged at 3000 rpm for 10 min, the deposit being used for Gram staining and inoculation onto blood, MacConkey, chocolate and anaerobic media. Blood and MacConkey plates were incubated aerobically, and the chocolate plates in 5% CO2, all at 35°C for 18 h. The anaerobic plates (with metronidazole discs) were incubated anaerobically at 35°C for 48 h.
The blood culture bottles containing pleural fluid were incubated in the BacTec 960 (Becton Dickinson) at 35°C for up to 5 days. A Gram stain was performed on any positive bottles and subculture was performed onto appropriate solid media to identify the organism(s) and perform antibiotic susceptibility testing.
Isolates of a coagulase-negative Staphylococcus were considered to be a contaminant and were not included in the data analysis.
Power calculation
Sixty patients were required to exclude the minimum clinically significant improvement in isolate rate of 25% (from 50% to 75%) with blood culture bottle culture (α=0.05, power 90%, the McNemar test).
Statistical analysis
Comparison of the microbiological sensitivity of tests was undertaken using the McNemar test for paired proportions (STATA version 9.2).
Results
The baseline characteristics are given in table 1, and microbiological results from the two standard cultures and the blood culture bottle culture are given in table 2.
Baseline characteristics of pleural infection and control patients
Pleural fluid culture results for each culture method
Patients with pleural infection
Primary analysis
In 53 patients, a full set of specimens allowed direct comparison between methods.
Addition of blood culture bottle culture to the standard laboratory culture increased the frequency of bacterial isolation from 20/53 (37.7%) cases with standard culture to 31/53 (58.5%) cases with the addition of blood culture bottle culture (difference 20.8%, 95% CI difference 8.9% to 20.8%, McNemar test=11.0, 1 degree of freedom (df), p<0.001).
Of the 31 cases with bacterial isolates combining these techniques, six had the same organisms identified by both, and four had different organisms identified. In nine cases only the standard culture was positive, and in 12 cases only the blood culture bottle culture was positive. Blood culture bottle culture also added microbiological value to standard culture in a further two (3.8%) cases, by identifying additional microbiologically relevant organisms when the standard culture was already positive (one Enterococcus spp, and one Streptococcus spp.—when standard culture was solely anaerobic).
Repeating the standard culture in a second laboratory (control intervention)
Standard culture results from both the recruiting hospital and the second laboratory were available in 49 cases. Addition of the information provided by the second laboratory culture produced a clinically insignificant increase in bacterial yield (6.1%). This tended towards, but did not achieve, statistical significance—19/49 (38.8%) culture-positive cases on standard culture at the recruiting hospital, increased to 22/49 (44.9%) with the addition of a repeat standard culture at a second laboratory (difference 6.1%, 95% CI difference −2.5% to 6.1%, McNemar test=3.0, 1 df, p=0.08).
The second bacterial culture added extra microbiological value in one further case (2.0%)—identifying an Acinetobacter spp. when the home culture was solely anaerobic.
Addition of blood culture bottle culture to the combined results of both standard cultures
The frequency of pathogens identified by both standard laboratory cultures combined was 22/49 (44.9%) cases, which increased to 30/49 (61.2%) cases when blood culture bottle culture was added (difference 16.3%, 95% CI difference 4.3% to 16.3%, McNemar test=8.0, 1 df, p=0.005).
Blood culture bottle culture still provided extra microbiological value when standard cultures were already positive in the two (4.1%) additional cases described earlier.
Figure 1 shows the additional sensitivity of the two standard cultures and blood culture bottle culture for each of the infecting bacterial classes. The pathogen classes match those shown to have prognostic significance.8 9

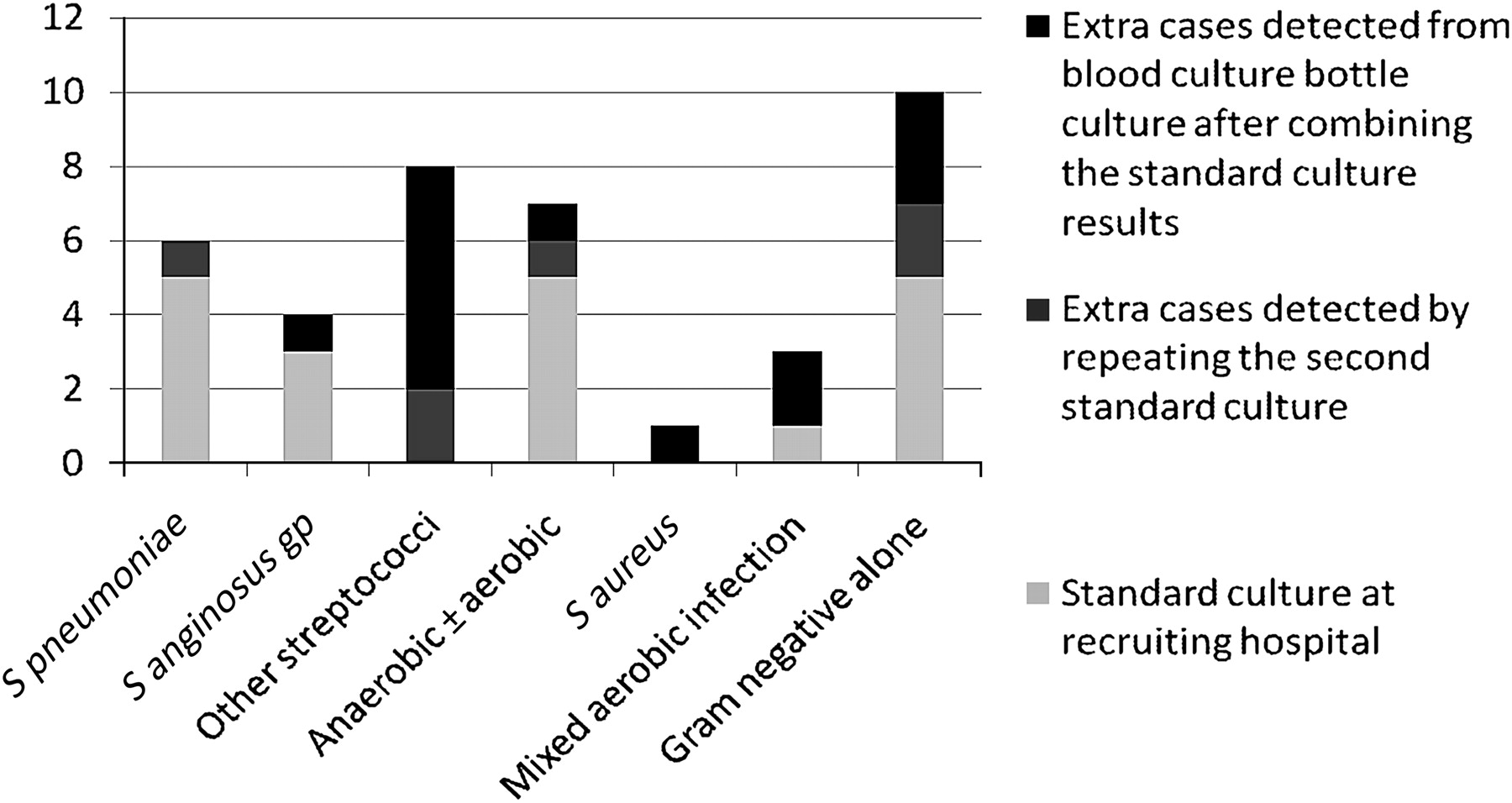{kind=link}
The value of adding different culture methods to standard culture in the additional detection of pathogens.
Venous blood cultures
Venous blood cultures were taken in 51/57 pleural infection cases, and were positive in only 6/51 (11.8%). Of the six positive cultures, three did not add any clinical value as the organism was also isolated from pleural fluid. In two cases they were the only positive culture for the patient (Streptococcus pneumoniae and Enterobacter aerogenes), and one cultured S pneumoniae—when only S aureus was isolated from the pleural fluid cultures (from the blood culture bottle culture).
Pleural fluid inoculum volume for blood culture bottle culture
It was possible to compare the 2, 5 and 10 ml inoculum volume in 11 patients with bacterial isolates from the aerobic culture bottles, and in 20 patients with bacterial isolates from the anaerobic culture bottles. There was no evidence of increased sensitivity with any of the inoculum volumes (table 3).
Comparison of the different pleural fluid inoculum volumes in culture-positive patients
Control patients without pleural infection
In the control patients, both sets of standard cultures and all blood culture bottle cultures were negative, with the exception of one standard culture sample that isolated Streptococcus viridans. Neither follow-up clinical information nor pleural fluid parameters from sampling supported the diagnosis of pleural infection.
Discussion
This is the first adequately powered prospective controlled study of culturing infected pleural fluid in blood culture bottles. Our results suggest that inoculation of pleural fluid into blood culture bottles increases diagnostic yield and the number of multiorganism infections detected. These data support the use of blood culture bottles in routine care for patients with suspected pleural infection.
The addition of blood culture bottle culture to standard culture increased the number of culture-positive cases in pleural infection by 20.8% (from 37.7% to 58.5%). This is consistent with a previous study, in which blood culture bottle culture increased culture positivity from 44% to 64%.12 This study adds to the former by being adequately powered and having a control intervention. Together, these two studies show that blood culture bottle culture is a valuable adjunct to standard laboratory plated culture within the context of pleural infection, and should be part of standard care.
It is interesting that this finding is very similar to the results in other ‘non-blood’ uses of blood culture bottle culture. In bacterial peritonitis, blood culture bottle culture increases the bacterial isolation rate by 29–49%,19–21 from a positivity rate on standard culture of 42–54%. In synovial fluid culture, blood culture bottle culture increases the bacterial isolation rate by up to 20% over the 10–20% culture positivity with standard culture.14 23 24
In addition to increasing the organism identification rate over standard culture at the recruiting hospital, blood culture bottle culture identified additional clinically important co-infecting bacteria in 2/53 (3.8%) cases. In the first case, standard culture isolated methicillin-resistant S aureus (MRSA), Pseudomonas aeruginosa and anaerobes, whereas bottle culture identified an Enterococcus spp.—which was of clinical value given the resistance patterns these organisms exhibit. In the second, standard culture grew only anaerobes, and bottle culture identified an aerobic growth of an organism from the Streptococcus anginosus group.
S pneumoniae isolation rates were higher from standard culture at the recruiting hospital compared with standard culture and blood culture bottle culture at the second laboratory (9.4, 1.9 and 1.8%, respectively). This may be due to the known tendency for delays in sample processing leading to impaired isolation of this fastidious organism.25 26 However, the frequency of isolation of non-pneumococcal streptococci also differed between standard and blood culture bottle culture, with the former identifying more organisms in the S anginosus group and the latter identifying more ‘other streptococci’ (namely other α-haemolytic streptococci). It is unclear why different bacteria culture preferentially in different media, and further studies are required to address this observation. This finding emphasises the importance of employing both standard and blood culture bottle culture strategies in parallel.
This study used repeated standard laboratory culture as a control intervention to test whether the improved yield of organisms using blood culture bottles was simply due to repeating the culture process. We have shown that blood culture bottle culture is superior to simple repetition of culture, with repeat standard culture increasing the rate of organism identification by 6.1% (from 38.8% to 44.9% of cases), and blood culture bottle culture increasing this further to 61.2% (65.3% if the additional clinically important bacterial isolates are considered).
The results from control patients without clinical evidence of pleural infection showed no false-positive cases identified from blood culture bottle culture of pleural fluid. This provides reassurance that the proposed diagnostic approach is robust.
This study demonstrated no evidence of differential rates of bacterial identification between different volumes of pleural fluid inoculum. This may suggest that even small residual volumes of possibly infected pleural fluid should be subjected to blood culture bottle culture.
There are several potential limitations to this study. Firstly, there was extra transportation time involved in transferring samples to the second laboratory, which could have altered the yield of bacteria. In addition, as we showed that different bacteria may have preferential growth in different media, and the spectrum of bacterial infection differs worldwide, this study should be repeated in other regions to ascertain the exact magnitude of benefit with blood culture bottle culture. A larger study may also be needed to address whether bottle culture is particularly beneficial in subgroups of clinical settings, for example taking into consideration antibiotic treatment prior to sampling, the size of the effusion or the likely bacterial load (degree of sepsis).
Conclusions
Inoculating pleural fluid into blood culture bottles at the bedside increases the rate of bacterial pathogen identification in pleural infection, when used in addition to standard laboratory culture. This increased yield appears to be specific to the use of blood culture bottles, is not a result of repeating the culture process and is clinically and statistically significant.
These results suggest that bedside pleural fluid inoculation into blood culture bottles should enter routine care in those with potential pleural infection.
Acknowledgments
We are greatly saddened to report the recent death of Professor Robert Davies. The authors wish to thank Emma Headley, Margaret Chapman, Nicky Crosthwaite, Claire Manners and Magda Laskawiec from the Respiratory Trials Unit, Oxford.
References
Footnotes
See Editorial, p 649
Funding This study was funded by the NIHR Oxford Biomedical Research Centre Programme.
Competing interests None.
Ethics approval This study was conducted with the approval of the Oxfordshire Regional Ethics Committee (reference 05/Q1605/5).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Respiratory infection
- Airwaves