Article Text

Abstract
Background Acute exacerbations of chronic obstructive pulmonary disease have a significant negative impact on both patients and healthcare systems. Currently, there are no physiological biomarkers that effectively monitor clinical change or predict respiratory readmission. Acute exacerbations impose a change in the respiratory muscle load-capacity-drive relationship. It was hypothesised that lack of a fall in neural respiratory drive would identify patients at risk of treatment failure and early hospital readmission.
Methods An observational study was performed at two UK teaching hospitals. Routine clinical physiological parameters and neural respiratory drive index (NRDI), calculated as the product of second intercostal space parasternal electromyography (EMG) activity normalised to the peak EMG activity during a maximum inspiratory sniff manoeuvre and respiratory rate, were recorded daily from admission to discharge.
Results 30 acutely unwell patients of mean (SD) age 72 (10) years, forced expiratory volume in 1 s 0.60 (1.65) l, NRDI 455 (263) AU and median length of stay 6 days were studied. Changes in NRDI correlated with changes in Borg score (r=+0.60; p<0.001), discriminated between patients deemed to have clinically improved rather than deteriorated (mean difference 339 AU; 95% CI 234 to 444; p<0.001) and identified those patients readmitted within 14 days (mean difference 203 AU; 95% CI 39 to 366; p=0.017).
Conclusions NRDI is a feasible clinical physiological parameter in patients with an acute exacerbation of chronic obstructive pulmonary disease and can provide useful information on treatment response and risk of readmission.
- Respiratory physiology
- chronic obstructive pulmonary disease
- hospital readmission
- COPD exacerbations
- respiratory muscles
Statistics from Altmetric.com
- Respiratory physiology
- chronic obstructive pulmonary disease
- hospital readmission
- COPD exacerbations
- respiratory muscles
Key messages
What is the key question?
Can neural respiratory drive act as an advanced physiological biomarker for clinical change during acute exacerbations of COPD?
What is the bottom line?
Neural respiratory drive, as measured non-invasively from parasternal electromyography, can accurately track clinical change during acute exacerbations of COPD and predict readmission to hospital.
Why read on?
This paper reports the clinical usefulness of non-invasive advanced respiratory physiological monitoring in patients during an acute exacerbation of COPD.
Introduction
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are a major economic burden to healthcare systems.1 2 In addition, exacerbations have a significant impact on health-related quality of life (HRQL) with admission avoidance and reduced length of hospital admission becoming national targets.3 Recently, healthcare systems, including the National Health Service, have focused on providing enhanced community care to facilitate early discharge.4–6 Acute care organisations have incorporated early warning scores, integrating basic cardiorespiratory and other physiological variables into a composite score, as predictors of clinical deterioration. However, the clinical usefulness of such scoring systems remains controversial.7–11 All these monitoring systems require accurate characterisation of disease severity and response to treatment to identify patients that are either deteriorating or only slowly improving to allocate patients to higher levels of clinical care. At present there are few physiological biomarkers available that have sufficient sensitivity and specificity to identify patients of AECOPD failing to respond to treatment.12
Neural respiratory drive (NRD) using diaphragm electromyography (EMGdi) reflects the balance between respiratory muscle load and capacity and has been shown to relate to disease severity in stable COPD.13 Despite its potential clinical usefulness, this technique has limited application in the acute setting as it requires the placement of an oesophageal electrode.13 14 Clinical interest has therefore been directed towards measuring the EMG of the parasternal intercostal muscles as these obligatory muscles of inspiration15 can be studied in a non-invasive manner.16 Parasternal EMG (EMGpara) signals, recorded from surface electrodes, have a direct relationship with respiratory muscle load17 and have been shown to respond to acute change.18 19
The use of EMGpara to monitor treatment response in AECOPD has not previously been reported. To be a useful clinical tool in the acute setting, the measurement must be reproducible in a stable setting and therefore one aim of this study was to establish the inter-occasion reproducibility of NRD in both healthy subjects and in patients with stable COPD. Furthermore, we hypothesised that changes in NRD would reflect clinical response to treatment during an AECOPD and a failure of NRD to fall would predict subsequent readmission to hospital.
Methods
Subjects
The study protocol was approved by the local research ethics committees and all participants provided written informed consent. Two studies were performed to (1) validate the reproducibility of EMGpara in (a) healthy subjects and (b) patients with stable COPD and (2) investigate the ability of EMGpara as a physiological biomarker to monitor change in AECOPD. The methods and results of the reproducibility studies are given in the online supplement. The acute study recruited patients admitted with AECOPD via the emergency department. AECOPD was defined based on clinical features and basic investigations.6 Initial patient management was according to standard local guidelines with oral corticosteroids, antibiotics and a combination of metered dose inhalers and nebulised bronchodilators. Patients were identified by the COPD team and subsequently screened and recruited by the research team, with the first EMGpara measurement recorded within 24 hours of hospital arrival. Repeat EMGpara measurements and the clinical dataset were recorded daily until the patient was reported as stable and suitable for hospital discharge.
Baseline data
Demographic and anthropometric data were collected. Borg20 and MRC dyspnoea scores21 22 were used to assess subjective breathlessness. HRQL data were obtained using the Chronic Respiratory Disease Questionnaire.23 Spirometry was performed with a hand-held device (EasyOne Diagnostic Spirometer, ndd Medical Technologies, Switzerland) according to standard guidelines.24 25 Repeat measurements were taken during admission. The patient was seated and rested for at least 5 min; bronchodilator therapy was withheld for the previous 4 h. Heart rate (HR), oxygen saturations (SpO2) and respiratory rate (RR) were measured over 1 min. Clinical data (HR, SpO2, RR, temperature (T), blood pressure (BP) and medical early warning score (MEWS)26) and the supervising senior clinician's summary opinion on clinical course were recorded from the medical notes and observation charts. A patient was defined as a clinical ‘deteriorator’ or ‘improver’ based on the summary opinion of the senior attending respiratory physician (respiratory specialist registrar or consultant) and the requirement for increased treatment. The respiratory clinicians were blinded to the EMGpara measurement, which was analysed offline following patient discharge. EMGpara signals were acquired either in a chair or semirecumbent in bed. Oxygen therapy was only used when the SpO2 was ≤88%.
EMGpara measurement
The second intercostal space (ICS) was identified using surface bony landmarks and the skin was prepared prior to placement of electrodes. EMGpara signal acquisition and processing was analogous to the method described previously for EMGdi.13 Details are provided in the online supplement. The resting signal was normalised to the maximum value obtained from a reproducible maximum sniff manoeuvre to produce the EMGpara%max. To reflect changes in respiratory pattern, the product of EMGpara%max and RR was calculated to produce the neural respiratory drive index (NRDI; arbitrary units (AU)). Nasal cannulae connected to a differential pressure transducer (Validyne DP45, Validyne, Northridge, California, USA) identified inspiratory and expiratory phases of breathing.
Data analysis and statistics
Reproducibility was assessed using coefficient of variability and Bland–Altman analysis.27 Relationships between EMGpara, EMGpara%max and NRDI and lung function parameters and HRQL data were analysed using regression analysis. Data were analysed using independent or paired t test where appropriate. Data that were not normally distributed, as defined by the Kolmogorov–Smirnov test, were transformed and then analysed as parametric data or, if the logarithm of the data remained non-normal, a non-parametric equivalent was used. Data analysis was conducted using SPSS software. All data are presented as mean±SD unless otherwise stated, with p<0.05 considered as statistically significant.
Results
Reproducibility of EMGpara
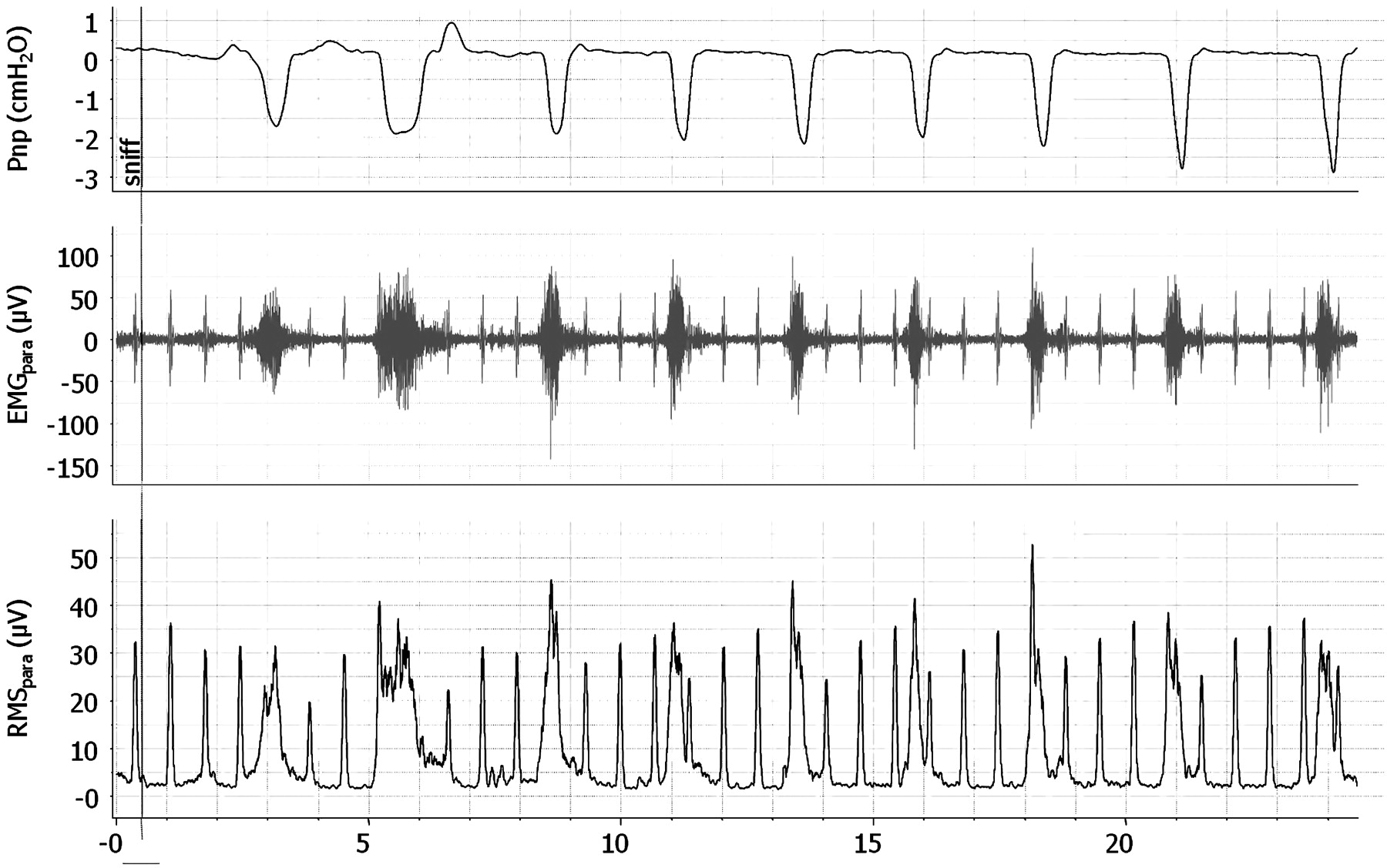
EMGpara data are reported as root mean squared (RMS; μV). A representative trace of a patient with stable COPD during the sniff manoeuvres is shown in figure 1. Reproducibility of EMGpara was confirmed in 10 healthy volunteers and 10 patients with stable COPD. Further details can be found in the online supplement.
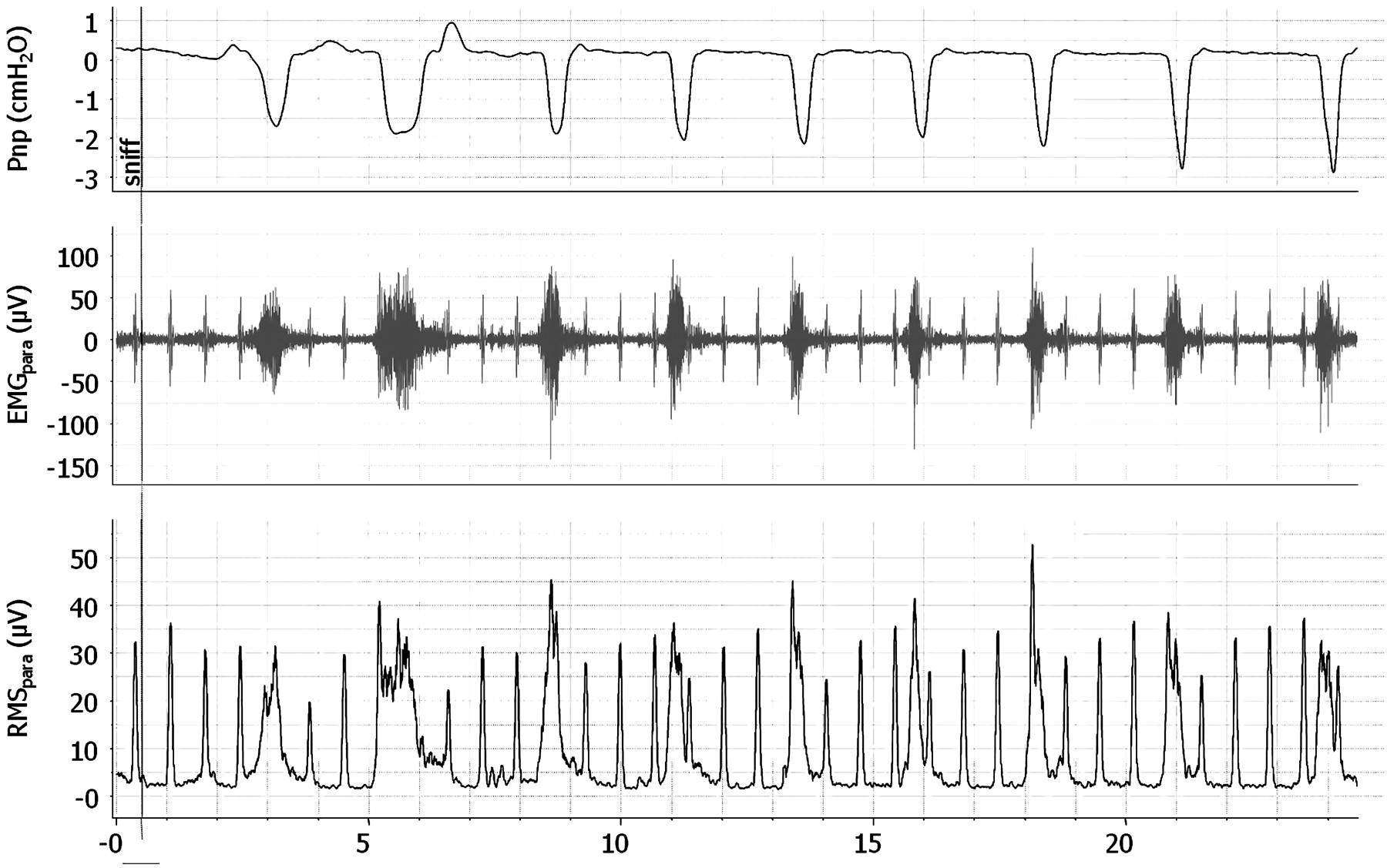
Representative trace of raw data during maximum sniff manoeuvre in a patient with stable chronic obstructive pulmonary disease. Pnp, nasal pressure derived from nasal cannulae; EMGpara, parasternal electromyogram activity; RMSpara, root mean squared analysis of EMGpara.
Change in EMGpara in patients with AECOPD
Thirty patients were recruited with a mean age of 72±10 years (47% male). On admission, the median MRC dyspnoea score was 5 (2–5). The median previous admission frequency and length of stay was 3 (0–13) and 6 days (2–34), respectively. Baseline data are provided in table 1 and full details can be found in the online supplement (table E1). Three patients received non-invasive ventilation with all cases initiated in the first 4 h of admission in the emergency department. Nine patients were discharged with home oxygen, all of whom were previously prescribed long-term oxygen therapy.
Standard clinical parameters and indices of neural respiratory drive on admission
Twenty-four patients had recordings on two occasions, five patients had recordings on three occasions and one patient had recordings on four occasions, producing 37 data pairs. ∆Borg score had a significant relationship with ∆EMGpara (r=+0.50; p=0.001), ∆EMGpara%max (r=+0.57; p<0.001) and ∆NRDI (r=+0.60; p<0.001) as shown in figure 2 and ∆FEV1 (r=−0.58; p=0.002). No relationship was observed with ∆SpO2 (p=0.16) or ∆RR (p=0.08).
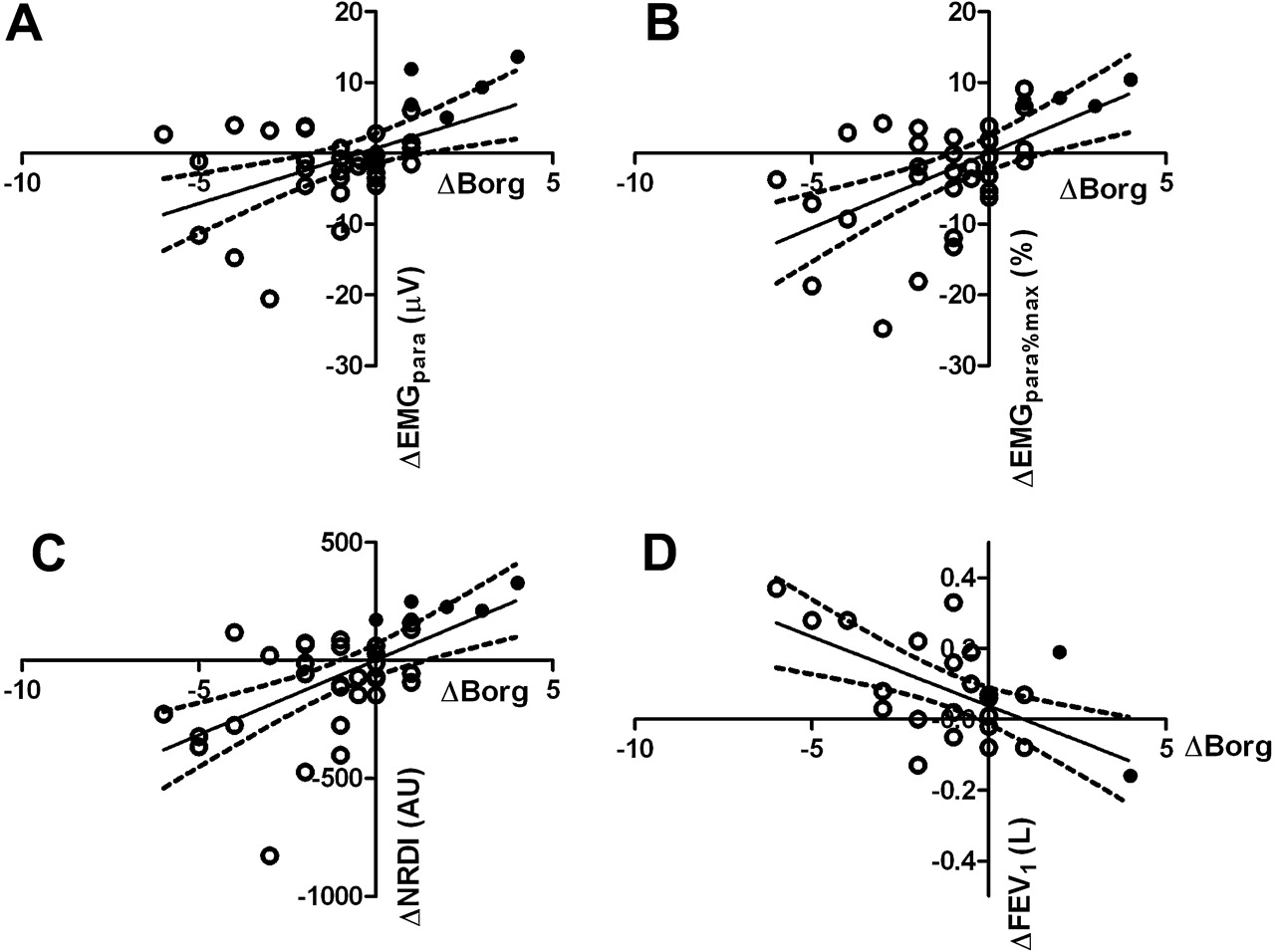
Data from 37 pairs of readings generated from consecutive recordings of physiological variables in 30 patients. Open circles represent ‘improvers’ and closed circles ‘deteriorators’. Comparison of change in Borg score with change in (A) EMGpara (r=0.50; p=0.001), (B) EMGpara%max (r=0.57; p<0.001), (C) NRDI (r=0.60; p<0.001), (D) FEV1* (r=−0.58; p=0.002). EMGpara, parasternal electromyogram activity; EMGpara%max, EMGpara during tidal breathing normalised for maximum EMGpara produced during a sniff manoeuvre; NRDI, neural respiratory drive index (EMGpara%max × RR). *Data from 26 pairs of data.
Significant differences were observed in mean change between ‘improvers’ and ‘deteriorators’ in all three EMGpara indices. However, there were no significant between-group differences in changes in RR, HR, SpO2 or forced expiratory volume in 1 s (FEV1) (table 2). A significant (p=0.02) but clinically small (+0.5) difference was observed in MEWS between ‘improvers’ and ‘deteriorators’. Patients who improved had a statistically significant reduction in dyspnoea (∆Borg −1.5; 95% CI −0.7 to −2.3), RR (∆RR −1.8 bpm; 95% CI −0.2 to −3.3) and an increase in FVC (∆FVC 0.22 l; 95% CI 0.05 to 0.40), with no statistically significant differences demonstrable in physiological variables in the ‘deteriorators’. Further data on daily changes in NRD can be found in the online supplement.
Difference between consecutive recordings of measured physiological variables in 30 patients from day of baseline measurement to repeat reading
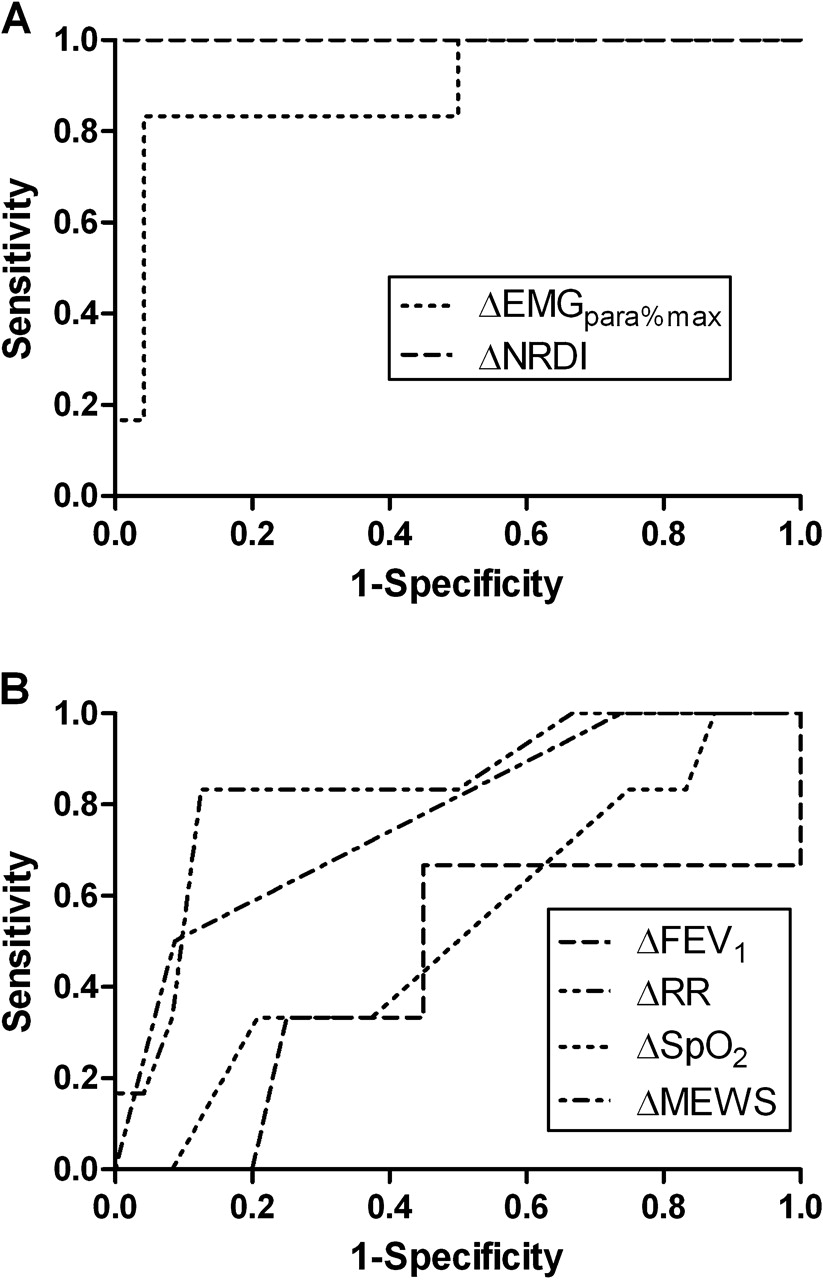
Receiver operating characteristics (ROC) plots (figure 3A) with change cut-offs >+6.6 for EMGpara%max and >+160 AU for NRDI had sensitivities of 83% (95% CI 54% to 100%) and 100% (95% CI 100% to 100%) and specificities of 96% (95% CI 88% to 100%) and 100% (95% CI 100% to 100%) for both EMGpara%max and NRDI, respectively. ROC plots of the standard clinical variables either did not statistically differ from the null hypothesis or could not produce a cut-off providing sensitivity >80% without reducing specificity to <90% (figure 3B).

Receiver operating characteristic (ROC) plot of change in (A) EMGpara%max and NRDI and (B) RR, MEWS, and FEV1 for detection of clinical deterioration. EMGpara%max, EMGpara during tidal breathing normalised for maximum EMGpara produced during a sniff manoeuvre; FEV1, forced expiratory volume in 1 s; NRDI, neural respiratory drive index; RR, respiratory rate; MEWS, medical early warning score.
Change in EMGpara between admission and discharge to predict readmission
A significant difference in ∆EMGpara%max and ∆NRDI between admission (first measurement within 24 h of admission) and discharge (final measurement within 24 h of clinical stability) was demonstrated between patients readmitted within 14 days as a consequence of a respiratory deterioration and those who remained at home. However, ∆MEWS, ∆FEV1 and number of previous admissions did not differ between patients who were and were not readmitted (table 3).
Difference between admission and discharge of measured physiological variables in 30 patients either readmitted (n=9) or not readmitted (n=21) within 14 days of hospital discharge
ROC plots (figure 4A) were calculated with cut-offs of a change in EMGpara%max >0% and NRDI >50 AU during admission, producing sensitivities of 67% (95% CI 36% to 97%) and 67% (95% CI 36% to 97%) and specificities of 62% (95% CI 41% to 83%) and 71% (95% CI 52% to 91%) for EMGpara%max and NRDI, respectively. None of the ROC plots for routine clinical variables differed significantly from the null hypothesis (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) plot of change in (A) EMGpara%max and NRDI and (B) RR, change in MEWS and number of previous admissions for hospital readmission at 14 days. EMGpara%max, EMGpara during tidal breathing normalised for maximum EMGpara produced during a sniff manoeuvre; NRDI, neural respiratory drive index; RR, respiratory rate; MEWS, medical early warning score.
Discussion
This study has shown that second ICS parasternal NRDI, calculated as a product of EMGpara and RR normalised for maximum EMGpara, is a reproducible physiological biomarker in patients with stable COPD and has greater sensitivity and specificity than standard clinical physiological parameters to identify patients with AECOPD failing to respond to treatment. Furthermore, the failure of NRDI to fall during AECOPD requiring hospitalisation identifies patients who are more likely to be readmitted with a further respiratory deterioration.
Critique of the method
Patient selection
The patients with AECOPD recruited were not consecutive admissions and therefore subject to selection bias. Despite this limitation, the demographics and severity of patients were similar to previously reported data.28 Furthermore, the goal of this study was to provide pilot data to demonstrate the feasibility and clinical usefulness of using non-invasive EMG monitoring as a physiological biomarker in the acute setting.
Surface EMGpara measurement
Although the issues of surface EMG recording are well described,29 we acknowledge that contamination from other chest wall muscles cannot be excluded. However, we carefully observed patient and electrode position during data acquisition to maximise the contribution of second ICS parasternal muscle to the inspiratory EMGpara signal and minimising the non-respiratory muscle activity of other muscles. Needle electrode technique could be used to isolate parasternal muscle activity30 31 but, similar to oesophageal measurement of diaphragm electrical activity, this invasive technique is not suitable for the acute setting.
Validity and reproducibility of EMGpara
EMGpara, as a measure of NRD, was shown to have satisfactory inter-occasion reproducibility in both healthy subjects and patients with stable COPD. Although the degree of variability with EMGpara in patients with COPD was greater in this study than that shown previously by our own group using EMGdi13 and EMGpara in patients with cystic fibrosis,32 the inter-occasion correlation for both healthy subjects and stable COPD was >0.80, which is a level that has previously been used to indicate acceptable inter-test agreement for surface electromyography.17
Definition of clinical change
The lack of an objective measure to monitor clinical progress in the acute setting to allow comparative changes with EMGpara is an obvious limitation of this study. All patients met an event-based criterion for a severe exacerbation of COPD requiring hospital admission.33 34 It is acknowledged that there is no ‘gold standard’ to predict or measure acute clinical progress in AECOPD,34 and therefore we compared EMGpara with standard clinical parameters and the summary opinion of the supervising senior physician. While this is a broad definition, it is widely used in both research and clinical practice and is the benchmark by which other novel influential assessment tools have been judged.35 Despite the limitations inherent in this choice of outcome, it allows the data to be easily interpreted. Clinical gestalt is the interpretation and analysis by the physician of the patient's report of their clinical state as well as the findings from the physical examination incorporating standard physiological variables and clinical parameters, which are subsequently processed as part of a learnt complex clinical algorithm to determine the clinical state of the patient and the response to treatment. In order to have measured the performance of this novel technique against a more definable objective marker, the study population may have to be limited to those patients in respiratory failure. However, this would have limited the applicability of the study and would have been difficult to demonstrate that measures of NRD added to already established and widely available techniques to measure clinical progress in this group.
Significance of findings
Parasternal muscle activity
Chest wall respiratory muscles have increased importance in patients with advanced COPD as progressive hyperinflation impacts adversely on diaphragm positioning and efficiency,36 37 which results in a compensatory increase in chest wall and accessory respiratory muscle activity.38 39 In particular, the uppermost parasternal intercostal muscles have been shown to be important inspiratory muscles.40–42 Furthermore, these parasternals have minimal post-inspiratory activity43 with the second ICS parasternal muscle demonstrating similar activity to the diaphragm.30 However, during increasing hyperinflation, as observed during an AECOPD, the resting length of the parasternals is less affected than the diaphragm, such that the parasternals make a greater contribution to inspiratory pressure generation.44 This increase in parasternal activity is also associated with higher levels of dyspnoea.45 These data provide the scientific rationale to develop EMGpara as a physiological biomarker to track changes in clinical state in patients with AECOPD. Patients failing to responding to therapy have persistent hyperinflation with sustained elevation in EMGpara activity compared with those responding to therapy and associated respiratory muscle unloading who have a decline in EMGpara activity as the lung volumes and diaphragm and parasternal activity return to baseline. Finally, NRD was expressed as a product of EMGpara and RR normalised for maximum EMGpara to produce NRDI, which incorporates the peak RMS inspiratory parasternal muscle activity per unit time as a ratio of maximum NRD, similar to pressure time index, which has been extensively used in previous studies as a dynamic measure of respiratory muscle fatigue.46 47
Dyspnoea
Dyspnoea provides a significant symptom burden in COPD. An objective method of assessing the severity of breathlessness has previously been lacking, with clinicians using subjective assessment tools. Physiological indicators of disease severity in COPD, such as FEV1, are acknowledged to be poorly predictive of dyspnoea.48 In contrast, changes in NRD have been shown to explain variance in exercise-induced dyspnoea.49 In the current study we observed a similar relationship between change in Borg score and change in EMGpara. Furthermore, as the initial measurements were recorded following commencement of emergency therapy, in some patients there were relatively small changes in second ICS parasternal muscle electrical activity and breathlessness, indicating that that this technique is sensitive enough to monitor relatively modest changes even after treatment initiation. These data therefore support the use of non-invasive second ICS parasternal EMG as a physiological biomarker of NRD that reflects perception of dyspnoea severity during AECOPD. Furthermore, as FEV1 has a weak relationship with dyspnoea, there is potential for EMGpara to be applied to patients in the stable state to monitor progression of disease and detect exacerbation onset, although more work is required to fully elucidate this relationship.
Monitoring response to treatment
NRD was shown to monitor response to treatment in patients admitted with AECOPD when calculated as EMGpara%max and NRDI. The reproducibility data indicate that the cut-off chosen for maximum sensitivity and specificity of detection for clinical change (EMGpara%max >6.6%) represents a genuine and detectable change in NRD as it is above the 95% upper limit of agreement on the Bland–Altman plot. In this population of patients with AECOPD this would have correctly tracked deterioration in five out of six occasions. This high sensitivity and specificity was further improved with the addition of respiratory rate to produce the NRDI, which correctly identified all episodes of deterioration in this sample set. This demonstrates the potential clinical utility of the test with the integrated physiological signal accurately reflecting the summary opinion of the senior attending respiratory physician in a way unable to be replicated by any of the standard clinical variables assessed.
Readmission
In addition to the ability to track changes in NRD during AECOPD using this technique, we have also shown that failure of NRDI to fall in response to therapy identifies those patients who were likely to be readmitted within 14 days of discharge with further respiratory deterioration. At present there are no clinically useful biomarkers that can predict readmission in these patients.50 Previous data in COPD patients with severe disease, as indicated by an FEV1 <1 l at discharge or more than two previous admissions in the preceding 12 months, reported that these patients were more likely to be readmitted following an exacerbation of COPD.51 The specificity of these particular predictors in the current cohort of patients was poor at <0.5 and therefore these are not clinically useful. Failure of NRDI to fall in response to treatment provides an easy to apply novel physiological biomarker to predict readmission in high-risk patients. Data from the ECLIPSE study have suggested that the ‘frequent exacerbator’ is a distinct phenotype in COPD.52 The measurement of NRDI in this context is not simply acting as a measure of disease severity or to identify the frequent exacerbator phenotype because, if our analysis was limited to those patients with two or more previous admissions (n=22), the sensitivity and specificity to predict readmission at 14 days remained similar to the whole cohort at 63% and 64%, respectively. The ability of this physiological tool to maintain its sensitivity and specificity in the higher risk group of patients increases the clinical utility, with the ability to further risk stratify the most high-risk patients. With the increasing role of early discharge and COPD outreach schemes to support patients in the community,3 4 this technique could facilitate clinical selection to identify patients who require greater community support or further hospital treatment prior to discharge. This approach has increasing importance as the rising incidence of failed hospital discharge has been highlighted by the UK government as an area for improved performance with potential financial penalties for hospitals.3 Although these observational data have shown that measures of NRDI can identify treatment failure and readmission in patients with AECOPD, further validation of the technique is required with prospective interventional trials. These could focus on the ability to identify treatment failure to allow patients to be discharged with standard or supportive care packages with the aim of reducing readmissions and the serious sequelae of repeated exacerbations.
Conclusion
NRD, measured from second ICS parasternal EMG, is an objective physiological biomarker which is both reliable and reproducible in healthy subjects and patients with stable COPD. The technique is well tolerated and feasible in the acute care setting. NRDI, in contrast to other standard clinical parameters, is able to provide an objective marker of dyspnoea, track the clinical state of a patient during an AECOPD and predict readmission at 14 days.
References
Supplementary materials
Web Only Data thx.2010.151332
Files in this Data Supplement:
{kind=link}
{kind=link}
Footnotes
Funding The work included within this manuscript was supported with grants from Guy's and St Thomas' Innovation Fund for Technology Transfer and NHS Innovations London. The authors acknowledge support from the Department of Health via the National Institute of Health Research (NIHR) Comprehensive Biomedical Research Centre award to Guy's and St Thomas' NHS Foundation Trust in partnership with King's College London and King's College Hospital NHS Foundation Trust. MIP's salary is part funded by the NIHR Respiratory Biomedical Research Unit of the Royal Brompton Hospital and Imperial College.
Competing interests None.
Ethics approval This study was conducted with the approval of the King's College Hospital REC.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves