Article Text

Abstract
Background Postoperative pulmonary complications (PPC) are the most frequently observed complications following lung resection, of which pneumonia and atelectasis are the most common. PPCs have a significant clinical and economic impact associated with increased observed number of deaths, morbidity, length of stay and associated cost. The aim of this study was to assess the incidence and impact of PPCs and to identify potentially modifiable independent risk factors.
Methods A prospective observational study was carried out on all patients following lung resection via thoracotomy in a regional thoracic centre over 13 months. PPC was assessed using a scoring system based on chest x-ray, raised white cell count, fever, microbiology, purulent sputum and oxygen saturations.
Results Thirty-four of 234 subjects (14.5%) had clinical evidence of PPC. The PPC patient group had a significantly longer length of stay (LOS) in hospital, high dependency unit (HDU) LOS, higher frequency of intensive care unit (ITU) admission and a higher number of hospital deaths. Older patients, body mass index (BMI) ≥30 kg/m2, preoperative activity <400 m, American Society of Anesthesiologists (ASA) score ≥3, smoking history, chronic obstructive pulmonary disease (COPD), lower preoperative forced expiratory volume in 1 s (FEV1) and predicted postoperative (PPO) FEV1 were all significantly (p<0.05) associated with PPC on univariate analysis. Multivariate analysis confirmed that age >75 years, BMI ≥30 kg/m2, ASA ≥3, smoking history and COPD were significant independent risk factors in the development of PPC (p<0.05).
Conclusion The clinical impact of PPCs is marked. Significant independent preoperative risk factors have been identified in current clinical practice. Potentially modifiable risk factors include BMI, smoking status and COPD. The impact of targeted therapy requires further evaluation.
- Bronchoscopy
- COPD mechanisms
- lung cancer
- pneumonia
Statistics from Altmetric.com
Background
Thoracic surgery impairs postoperative respiratory function resulting in a relatively high risk of developing postoperative pulmonary complications (PPCs). The incidence (19–59%) is much higher than following upper (16–17%) or lower abdominal surgery (0–5%).1 The overall in-hospital frequency of deaths is 5% for pneumonectomy, 2% for lobectomy and 5% for oesophagectomy (UK thoracic registry data, 2008). PPCs are the major cause or a contributing factor to the number of deaths following lung resection, accounting for up to 84% of all deaths. Other major significant clinical and economic impacts of PPCs include prolonged hospital stay and need for admission to the intensive therapy unit (ITU).2
Risk factors for PPCs following pulmonary resection have been identified from numerous clinical studies using a variety of research designs and definitions. The most frequent risk factors include age, preoperative pulmonary function tests, cardiovascular comorbidity, smoking status and chronic obstructive pulmonary disease (COPD).2–5
Existing studies of PPCs are difficult to compare for several reasons. First, the definition and criteria for PPCs vary widely between studies. A broad definition such as ‘any pulmonary abnormality occurring in the postoperative period that produces identifiable disease or dysfunction which is clinically significant and adversely affects the clinical course’ incorporates a wide spectrum of processes such as pneumonia, atelectasis, respiratory failure, pulmonary embolus, pleural effusion, pneumothorax and pulmonary oedema. In part this explains the large variation in the recorded frequency of PPC.2–5 Second, many of the identified risk factors for PPCs are interrelated, but this has been difficult to define because small sample size precludes multivariate logistic regression to identify independent factors. Finally, many studies are retrospective in design and so there are valid concerns as to the sensitivity and specificity of data scoring: missing out on minor complications and overscoring in patients perceived as presenting an increased risk (eg, patients planned to be admitted to the ITU).
Lung cancer kills over 30 000 people each year in the UK, accounting for 5.6% of all UK deaths.6 Patients with lung cancer in the UK present at a later stage and have a higher comorbidity than patients in comparable European cities.7 As a result, surgical resection rates (a marker of outcome) are lower in the UK (11%) than in the rest of Europe (17%) and North America (21%).8 Consequently, survival rates for lung cancer in the UK are very poor and have not improved in the last 30 years; for patients diagnosed between 1993 and 1995 and followed up to 2000, only 5.5% were alive after 5 years. This compares with a 5-year survival rate of 13% reported in the USA and similar proportions for several other European Community countries.9
One approach to dealing with the poor surgical resection rate and overall survival is to identify and optimise modifiable factors which may increase the risk of surgery or preclude it altogether. The aims of this study were to assess the incidence of PPCs and to identify potentially modifiable risk factors.
Methods
A prospective observational study was performed in a regional thoracic centre on all consecutive patients undergoing thoracotomy and lung resection between October 2007 and October 2008. Decisions regarding patient operability and resectability were informed by the British Thoracic Society guidelines for lung cancer resection. All pulmonary resections were performed by open thoracotomy. Emergency procedures were excluded from the analysis.
All surgical procedures were performed under general anaesthesia with single lung ventilation. Patients were scheduled for extubation in the recovery room at the end of the operation. Postoperatively, patients were managed in a dedicated thoracic HDU (level 2) and ward unless complications required their admission to the ITU. Postoperative pain control was achieved by continuous thoracic epidural analgesia or intrathecal morphine and/or intercostal blocks or systemic opioids (parenteral administration or intravenous patient-controlled administration). The choice of analgesic technique was made by the anaesthetist. All patients had a daily physiotherapy programme from the first postoperative day comprising deep breathing exercises, incentive spirometry (Coach 2, Medimark, Grenoble, France), supported coughing and mobilisation.
A PPC score, the Melbourne Group Scale (MGS), was used around the same time each day by senior physiotherapists who were performing their routine respiratory assessments.10 Using this score, PPC is defined in those patients presenting with four or more of the following eight dichotomous factors: chest x-ray findings of atelectasis or consolidation; raised white cell count (>11.2×109/l) or administration of respiratory antibiotics postoperatively (in addition to prophylactic antibiotics); temperature >38°C; signs of infection on sputum microbiology; purulent sputum differing from preoperative status; oxygen saturations <90% on room air; physician diagnosis of pneumonia; and prolonged HDU stay or readmission to HDU or ITU for respiratory complications (table 1). The reliability of the score was established by its use in 20 patients by two independent physiotherapists: score results were identical (data not shown). The clinicians were blinded to the daily score result so it did not alter patient management.
Melbourne Group Scale (MGS)
Preoperative and postoperative data collected included age, body mass index (BMI), forced expiratory volume in 1 s (FEV1), predicted postoperative (PPO) FEV1, American Society of Anesthesiologists (ASA) score, COPD, smoking status, subjective preoperative activity level, comorbid conditions (specifically significant cardiac, neurological, pulmonary and orthopaedic (affecting mobility) conditions), operative procedure, postoperative analgesia, postoperative mobility, length of stay (LOS) in hospital, HDU LOS, ITU admission and number of deaths.
Statistical analysis
Unless otherwise stated, results are expressed as mean±SD or median (95% CI) for continuous variables and as a percentage for categorical variables. Statistical support was provided by an independent statistician. Analysis of the outcomes of the number of deaths and ITU admission were performed with the Fisher exact test as numbers were small, and LOS was analysed with the Mann–Whitney U test as data were skewed. For univariate analysis of risk factors, dichotomous variables were analysed with the χ2 test, the independent sample t test was used to analyse continuous variables and the Mann–Whitney U test for the ordinal scale used for preoperative activity level. The risk of PPCs associated with these variables was evaluated using stepwise logistic regression analysis to estimate ORs and their 95% CIs. Continuous and ordinal variables were dichotomised. A p value ≤0.1 by univariate analysis was chosen as the criterion for submitting variables to the model. Goodness-of-fit was assessed by the Hosmer and Lemeshow χ2 test. The sensitivity and specificity of the model were calculated from the percentage accuracy in classification after application of the model.
Results
Two hundred and thirty-four patients underwent pulmonary resections during the study period, 137 of whom were male (59%). The mean±SD age of the group was 63±14 years, mean predicted FEV1 was 81±20%, mean BMI 26.2±4.6 kg/m2, 131 patients (56%) had an ASA score ≥3, 37 patients (15.8%) had COPD, 36 (15.4%) were current smokers, 206 (88%) had primary lung cancer, 20 (8.5%) had secondary metastatic cancer and 8 (3.5%) had chronic infection.
The most frequent procedure was lobectomy (n=124, 53%) followed by wedge or segmentectomy (n=76, 32.5%) and pneumonectomy (n=24, 10.3%). The least frequent procedures were sleeve resections and exploratory thoracotomy (n=6, 2.6% and n=4, 1.7%, respectively).
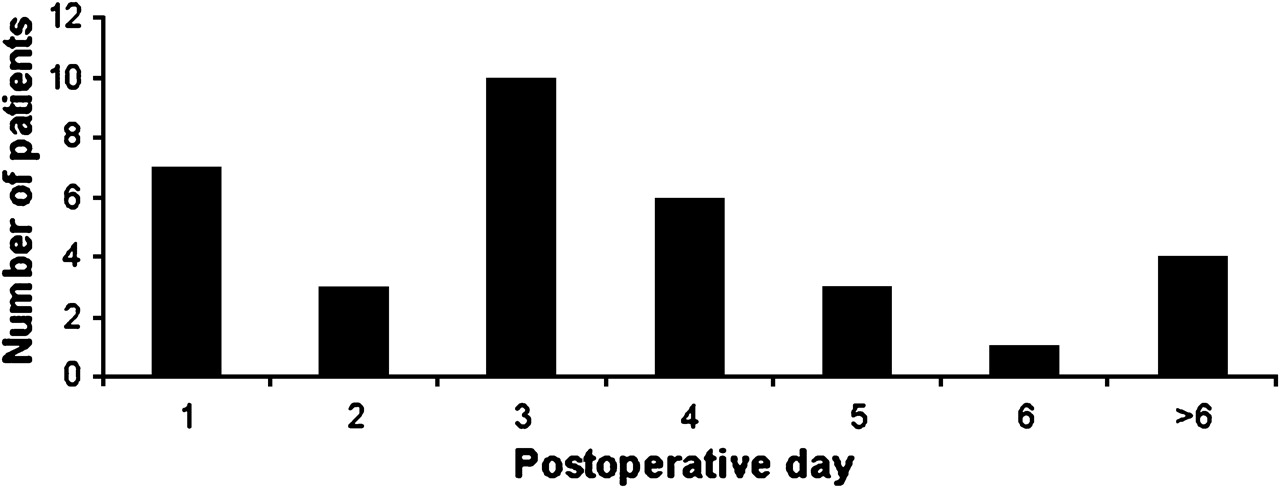
Thirty-four patients (14.5%) had clinical evidence of PPC using the MGS. The four most common positive factors to trigger a score of 4 were chest x-ray showing atelectasis /infiltration, temperature >38°C, physician diagnosis of pneumonia/chest infection and purulent sputum (table 1). The distribution of the postoperative day of patients' first scores of ≥4 is shown in figure 1.
{kind=link}
Timing of patients′ first Melbourne Group Scale score of ≥4.
Patients in the PPC group had a significantly (p<0.001) longer hospital LOS, HDU LOS and higher frequency of ITU admission and number of deaths (table 2). Four (11.8%) of the 34 patients in the PPC group died from complications of pneumonia and one patient (0.5%) of the 200 in the non-PPC group died from postoperative myocardial infarction.
Outcomes following PPC
Age, BMI and ASA were all significantly higher (p<0.05) in the PPC group. Subjective preoperative activity level, FEV1 and PPO FEV1 were all significantly lower (p<0.05) and there were significantly more current smokers and patients with COPD in the PPC group (p<0.05, table 3). Types of analgesia, operative procedure or primary pathology were not significant risk factors in this study.
Statistically significant risk factors for developing PPC
Stepwise logistic regression analysis was then used to identify perioperative variables independently associated with PPCs. Five independent risk factors were associated with the development of PPCs: age ≥75 years, BMI ≥30 kg/m2, ASA ≥3, current smoking history and COPD (table 4). The goodness-of-fit χ2 of this model remained non-significant during the five steps. The resulting logistic model had a sensitivity of 81% and specificity of 69%. The sensitivity of the model is the percentage of the group accurately identified by the model as having a PPC and the specificity is the percentage correctly identified as not having one.
ORs and CIs for independent risk factors
Discussion
This study demonstrates five significant independent preoperative risk factors for PPC identified by the MGS: age ≥75 years, BMI ≥30 kg/m2, ASA ≥3, current smoking history and COPD. The frequency of PPC during this prospective study at a regional thoracic surgery unit was 14.5%, which is comparable with international results.2–5 The clinical and potential economic impact of PPC is marked, with significantly longer hospital and HDU LOS, frequency of ITU admission and number of deaths.
The overall incidence of PPCs following thoracic surgery varies from 15% to 37.5%, primarily due to the type of pulmonary complications studied, the clinical criteria used in the definition and the type of surgery included.
Our study may be limited by its purposeful exclusion of less common but serious respiratory complications such as pulmonary embolus and bronchopleural fistula. The risk factors for these complications are likely to differ from the studied PPCs, hence including them may have diluted the associations stated. Preoperative assessment of pulmonary function has been the most extensively studied factor for predicting morbidity and the number of deaths after pulmonary resection. In our study there were significant differences between the PPC and non-PPC groups on univariate analysis for both PPO FEV1 and FEV1. However, they were not significant independent factors on multivariate analysis, which is in agreement with other studies.2 3 11 There are several potential explanations for this. The use of guidelines to aid selection of patients may have resulted in fewer patients with poor lung function undergoing surgery, so that FEV1 is no longer a factor. Also, advances in perioperative care and the resultant reduction in the number of deaths may now mean that absolute values in lung volumes are less critical. There is a growing body of evidence that gas transfer factor as a marker of lung function is better at predicting outcome after surgery.12 In our study gas transfer factor was performed only in patients with limited exercise tolerance or lung volumes so data are limited. Similarly, the use of any kind of ‘lateral test’ or lung perfusion scans to correct PPO FEV1 was limited to patients with borderline predicted lung function. This is of special relevance in patients with COPD who may have a lung volume reduction type effect with a less than expected fall in FEV1 and, in some instances, an improvement in PPO FEV1.13 In our study the presence of COPD was in itself a risk factor for PPC and, once COPD is taken into account, PPO FEV1 and FEV1 are no longer independent factors.
Higher ASA physical status has been shown to be associated with postoperative respiratory complications following both thoracic and non-thoracic surgery.2 However, in our study we found that the ASA assessment performed by consultant anaesthetists prior to surgery proved to be an important risk factor for PPC, probably because it takes into account both pulmonary and non-pulmonary comorbidity.
Although advanced age is likely to lead to a higher incidence of coexisting comorbid conditions, in itself it was independently a powerful predictive risk factor. The contribution of age to PPC may differ according to the methodology used to assess its impact.2 3 We chose ≥75 years to reflect the ageing population, and we found a significantly higher frequency of PPC in this age group.
Smoking has been shown to pose an increased risk for PPC.2 14 The reduction in the frequency of perioperative complications after smoking cessation may not be seen until a period of abstinence of up to 2 months; several studies have reported that recent quitters may even have a higher frequency of complications postoperatively than current smokers.15 This may be explained by sputum retention, delayed improvement in inflammatory functions and possible reduction in irritant-induced coughing.16 However, patients with lung cancer who continue to smoke may have a reduced survival, poorer quality of life and a higher risk for subsequent cancers.17 18
This is the first prospective study to show that obesity (BMI ≥30 kg/m2) is an independent risk factor for PPC. Several retrospective studies have shown no relationship.19 20 The contribution of BMI may be masked by rapid weight loss which in itself is a risk factor in the development of PPC, but its contribution to the variability in the number of deaths is relatively low.14 21 Patients with a higher BMI may also be party to a selection bias owing to increased perceived risk. However, a BMI ≥30 kg/m2 need not result in a higher incidence of PPC if an aggressive preventive strategy of management is adopted including the use of video-assisted techniques.20 22
Studies of risk factors can improve the information given to patients and contribute to developing models to predict complications. Although these models may identify high-risk patients, they cannot predict in which single individual a complication may develop and therefore should not be used to exclude patients from surgery. Risk stratification can enable forward planning of the management of those considered to be most at risk postoperatively and even preoperatively. Prognostic variables may be modifiable but even a strong statistical association does not necessarily indicate a cause and effect relationship. For example, optimising COPD may not actually decrease the incidence of PPCs. It has been suggested that high-risk patients can be optimised with preoperative and postoperative cardiopulmonary rehabilitation to reduce their operative risk, frequency of PPC and hospital stay and improve postoperative outcomes including postoperative lung function.23 24 In addition, preoperative pulmonary rehabilitation may improve preoperative exercise capacity and so operability.25 26
Added attention to postoperative strategies shown to improve outcomes is warranted in high-risk groups. Postoperative physiotherapy, incentive spirometry with inspiratory muscle training and prophylactic mini-tracheostomy have all been shown to reduce the frequency of PPC.24 27 28 Positive pressure therapy may improve ventilation and secretion clearance. Early use of non-invasive ventilation improves physiological measures and may reduce the need for endotracheal mechanical ventilation and the number of deaths.29
Conclusion
The clinical and potential economic impact of PPC is marked. Five significant independent preoperative risk factors have been identified, with smoking status modifiable while others factors such as COPD and BMI could be optimised. The impact of such targeted therapy will require further evaluation. An ASA score ≥3 indicated an increased risk of PPC in this study. Consistent with a growing body of evidence, preoperative spirometry did not help to identify patients at increased risk of PPCs. Pulmonary complications are responsible for significant numbers of deaths and morbidity of patients undergoing thoracotomy; the future development and adoption of innovative strategies is required to reduce their impact in an ageing comorbid population.
Acknowledgments
The authors would like to acknowledge all of the members of the ‘Melbourne Group’ for the development of their PPC diagnostic tool referred to in this paper as the Melbourne Group Scale (MGS). Special thanks go to Julie Reeve, School of Physiotherapy, Faculty of Health and Environmental Studies, Auckland University of Technology, Auckland, New Zealand and Linda Denehy, School of Physiotherapy, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, Melbourne, Australia for advice regarding the use of the tool ahead of its publication in July 2008.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the East Birmingham local regional ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.