Article Text

Abstract
Background: The load imposed on ventilation by increased body mass contributes to the respiratory symptoms caused by obesity. A study was conducted to quantify ventilatory load and respiratory drive in obesity in both the upright and supine postures.
Methods: Resting breathing when seated and supine was studied in 30 obese subjects (mean (SD) body mass index (BMI) 42.8 (8.6) kg/m2) and 30 normal subjects (mean (SD) BMI 23.6 (3.7) kg/m2), recording the electromyogram of the diaphragm (EMGdi, transoesophageal multipair electrode), gastric and oesophageal pressures.
Results: Ventilatory load and neural drive were higher in the obese group as judged by the EMGdi (21.9 (9.0) vs 8.4 (4.0)%max, p<0.001) and oesophageal pressure swings (9.6 (2.9) vs 5.3 (2.2) cm H2O, p<0.001). The supine posture caused an increase in oesophageal pressure swings to 16.0 (5.0) cm H2O in obese subjects (p<0.001) and to 6.9 (2.0) cm H2O in non-obese subjects (p<0.001). The EMGdi increased in the obese group to 24.7 (8.2)%max (p<0.001) but remained the same in non-obese subjects (7.0 (3.4)%max, p = NS). Obese subjects developed intrinsic positive end-expiratory pressure (PEEPi) of 5.3 (3.6) cm H2O when supine. Applying continuous positive airway pressure (CPAP) in a subgroup of obese subjects when supine reduced the EMGdi by 40%, inspiratory pressure swings by 25% and largely abolished PEEPi (4.1 (2.7) vs 0.8 (0.4) cm H2O, p = 0.009).
Conclusion: Obese patients have substantially increased neural drive related to BMI and develop PEEPi when supine. CPAP abolishes PEEPi and reduces neural respiratory drive in these patients. These findings highlight the adverse respiratory consequences of obesity and have implications for the clinical management of patients, particularly where the supine posture is required.
Statistics from Altmetric.com
Obesity is a rapidly increasing public health problem.1 2 Ventilatory impairment due to increased body mass occurs, causing complications during hospital admissions, contributing to increased morbidity and mortality.3 Mechanical indices of ventilatory load have been studied, and increase in the supine posture.4–9 There is evidence that obese subjects develop intrinsic positive end-expiratory pressure (PEEPi) when supine and have expiratory flow limitation,5 probably due to the low lung volumes at which obese subjects breathe.8 However, accurate measurement of inspiratory pressures is difficult because of measurement artefacts of oesophageal and gastric pressure in the supine position.6 8 10 Respiratory muscle electromyography (EMG), which provides an index of global respiratory motor drive, can add valuable information to that from mechanical indices. Although not a new concept, hitherto the measurement of respiratory muscle EMG has been limited to documenting relative changes in muscle recruitment with changes in posture or responses to carbon dioxide-stimulated breathing.7 11–13 Absolute levels of neural respiratory drive in response to the load imposed on the respiratory muscles in obesity have not been described.14
This study was undertaken to determine the increased respiratory load and neural drive of obese subjects when seated and supine. Besides an increase in body mass, multiple other confounders of metabolic, hormonal, chemoreflex and behavioural origin may contribute to increased motor drive, all of them reflected in an increased central respiratory motor drive, as measured by the diaphragm EMG. For this purpose, we measured neural respiratory drive to the diaphragm and to the extradiaphragmatic respiratory muscles, inspiratory pressures and ventilation. We hypothesised that neural respiratory drive is progressively higher with increasing obesity and that drive further increases when supine.
METHODS
Obese subjects were recruited from the metabolic outpatient clinic at King’s College Hospital and healthy normal subjects followed an announcement of the study on the hospital intranet.
Age, sex, height, weight, body mass index (BMI), waist and hip circumference, waist-to-hip ratio and neck circumference as well as smoking history were recorded. The patients filled in the Medical Research Council (MRC) Dyspnoea Scale,15 the Epworth Sleepiness Scale (ESS)16 and the Hospital Anxiety and Depression Score (HADS).17 All subjects underwent standardised spirometry.18 19 Vital capacity was measured in the sitting and supine positions. Arterialised earlobe blood was analysed for blood gases (Bayer Rapidlab 248, Diamond Diagnostics, Massachusetts, USA).
Respiratory pressures and EMG of the diaphragm and extradiaphragmatic respiratory muscles
Two balloon catheters (Cooper Surgical, Connecticut, USA) for the measurement of oesophageal (Poes) and gastric (Pgas) pressures lubricated with lidocaine (2%) gel were introduced via one nostril into the oesophagus (filled with 0.5 ml air) and the stomach (filled with 2 ml air) in the standard manner14 and the positioning checked as described by Baydur et al.20 In addition, a custom-made multipair electrode catheter (Yinghui Medical, Guangzhou, China) was inserted via one nostril to record the transoesophageal EMG of the diaphragm (EMGdi), as previously described.21–24 The EMG signals of the neck muscles (sternocleidomastoid), parasternal intercostals and abdominal (external oblique) muscles were recorded using surface electrodes (Kendall Arbo, Tyco Healthcare, Neustadt, Germany) from standard positions.25–27
The following manoeuvres were performed and EMG and pressures recorded:14
Maximum inspiratory pressure (Pimax)
Maximum expiratory pressure (Pemax)
Sniff pressures (nasal (Pnasal), oesophageal (Poes) and transdiaphragmatic (Pdi))
Cough gastric pressure (cough Pgas)
Total lung capacity manoeuvre (TLC)
“Sprint” (15 s) maximal voluntary ventilation (MVV)
Pimax, sniff, TLC and MVV manoeuvres have been shown to produce maximal or near maximal diaphragm activation, and the highest value achieved by these manoeuvres was taken to define maxima for the inspiratory muscles.21 24 28 Pemax and cough Pgas manoeuvres were chosen to determine the reference for the maximum abdominal muscle EMG.
Recording of spontaneous breathing
Resting breathing was recorded for 5 min while relaxed, seated in an armchair, and for 5 min lying supine on a bed, the head resting on a pillow, wearing a noseclip, breathing through a flanged mouthpiece connected to a pneumotachograph. Mean (SD) EMG and pressure data for all comparable breaths during this period were analysed. Electromechanical coupling of the diaphragm sitting and supine was described in terms of ΔPdi/EMGdi.14 Dynamic compliance was derived from the change in oesophageal pressure and volume during inspiration,14 measured for 5–10 comparable breaths. Volume was derived from the flow signal. PEEPi was defined as the change of oesophageal pressure from end-expiratory baseline pressure prior to the beginning of inspiratory flow;5 at least 10 breaths were analysed and the mean reported (fig 1; additional information on PEEPi is described in fig E1 in the online supplement).
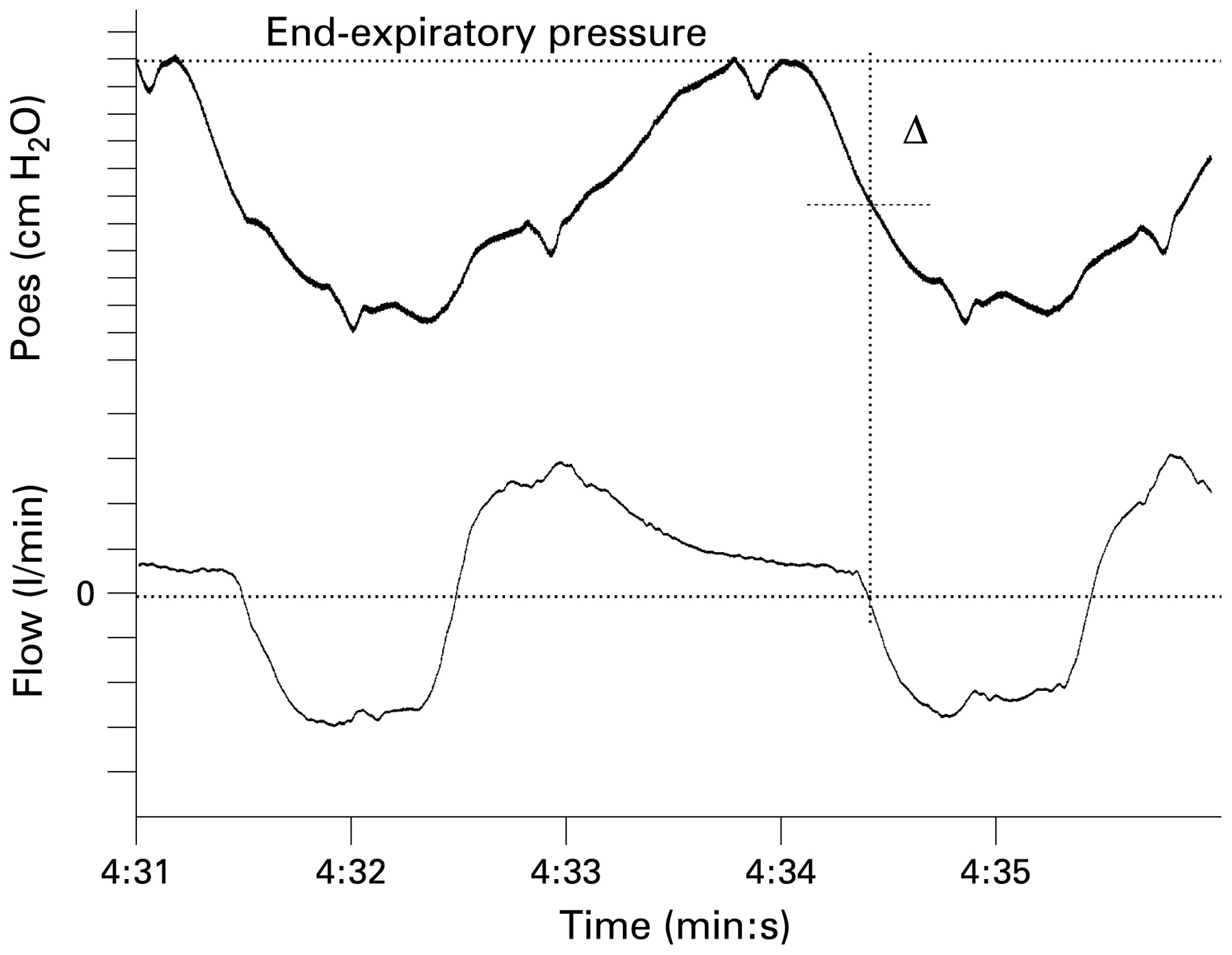
Intrinsic positive end-expiratory pressure (PEEPi) as defined by change of oesophageal pressure (ΔPoes) from end-expiratory baseline prior to inspiratory flow (vertical dashed line) in the supine posture in a morbidly obese subject.
In addition, a subgroup of seven obese patients was studied when receiving continuous positive airway pressure (CPAP; Resmed S8 Elite II, San Diego, California, USA) delivered through a full facemask (Respironics Performa Trak, Murrysville, Pennsylvania, USA) and titrated against PEEPi.
Data analysis and statistics
EMG and pressure data were saved and analysed with Chart Version 5.4 (ADInstruments, Colorado Springs, Colorado, USA) on a Mac Powerbook Pro Computer (Apple Computers, Cupertino, California, USA). The results were further analysed using SPSS Version 16 (SPSS, Chicago, Illinois, USA) for Mac OS X, figures were plotted using SPSS and Microsoft Powerpoint 2004 (Microsoft, Seattle, Washington, USA). Following testing for normality, results are given as mean (SD). A p value of <0.05 was considered significant. The correlation between EMGdi and BMI was plotted in a scattergraph and R2 reported for seated and supine measurements. A repeated measures one-way ANOVA was performed including post hoc analysis using Bonferroni’s correction for multiple comparisons. Questionnaire data were expressed as median (interquartile range). Other parametric data were compared using paired and unpaired t tests, non-parametric data using the Mann-Whitney rank sum test and categorical data using the Fisher exact test. Multiple linear regression analysis was performed to establish independent predictors of PEEPi. The variables age, sex, neck circumference, waist-to-hip ratio and BMI were entered into a forward model.29
RESULTS
Sixty subjects were measured, 30 obese (BMI ⩾30 kg/m2) and 30 non-obese (BMI <30 kg/m2). The obese group had the same height and sex distribution as the non-obese group, but were heavier and slightly older (table 1). Smoking status was similar in both groups.
On the questionnaires, obese subjects scored higher for daytime fatigue, dyspnoea and anxiety and depression (table 1). Both groups had normal inspiratory and expiratory muscle strength; expiratory muscle strength was higher in the obese group. Dynamic compliance was lower in the obese group; both groups had a decrease in dynamic compliance when changing posture from sitting to supine (table 1).
Obese subjects had lower FEV1 and vital capacity (VC), while the FEV1/VC ratio and the fall in VC with posture was not significantly different between the groups. Earlobe blood gas results showed slight but statistically significant differences so that arterial oxygen tension (Pao2) was lower and arterial carbon dioxide tension (Paco2) and bicarbonate were higher in the obese subjects (table 1).
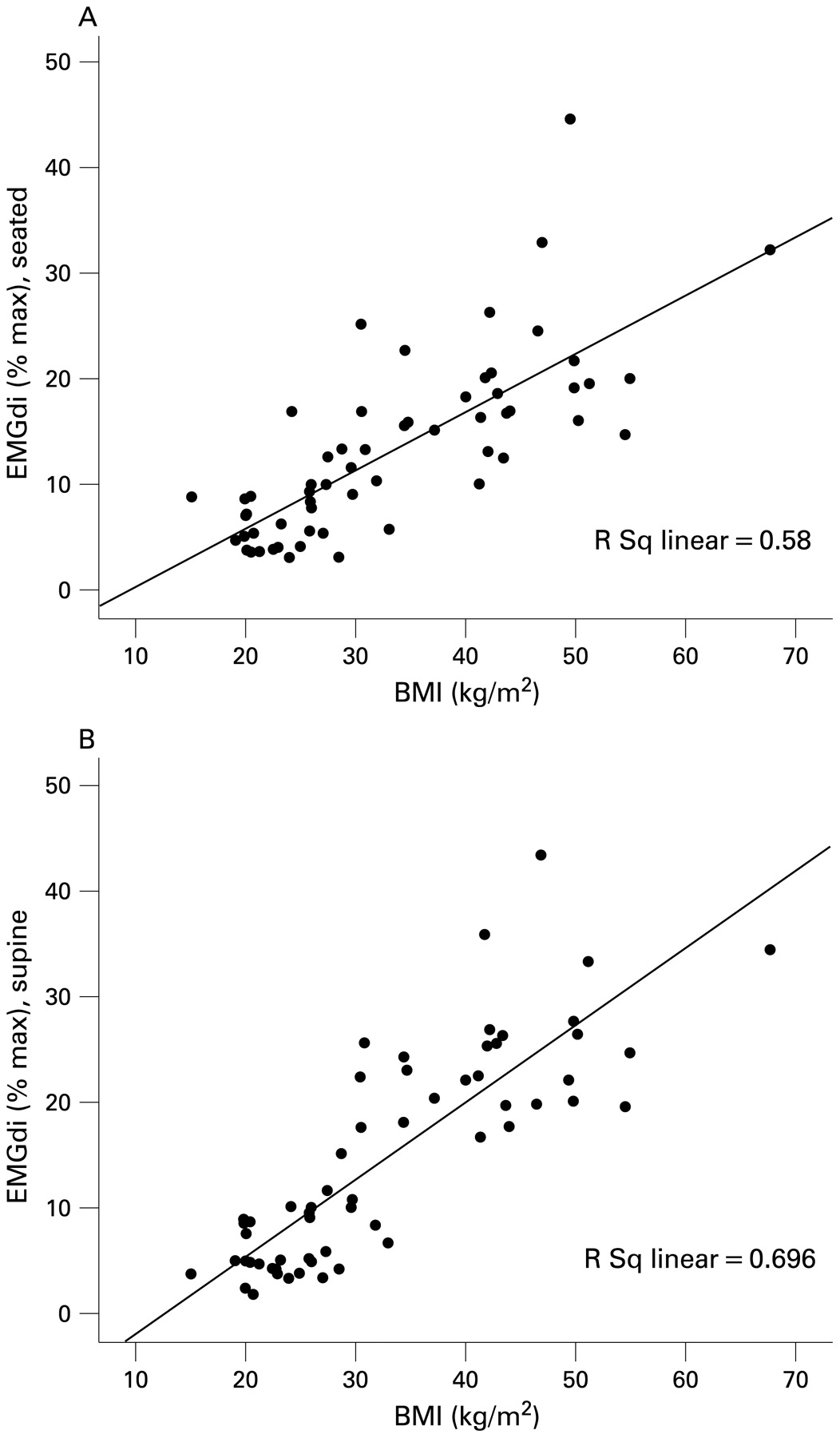
When seated, both groups had a similar breathing pattern with no differences in respiratory rate, tidal volume or minute ventilation. Obese subjects had larger oesophageal and transdiaphragmatic pressure swings. Correlation between EMGdi and BMI was R2 = 0.58 (p<0.001, fig 2). Average end-expiratory gastric and oesophageal pressures were higher in obese subjects, as was inspiratory EMG activity in all muscles studied (table 2, fig 2).

Neural respiratory drive as measured by electromyography of the diaphragm (EMGdi) versus body mass index (BMI) when (A) seated and (B) supine. A high correlation is observed when sitting (R2 = 0.58, p<0.001) and supine (R2 = 0.696, p<0.001). Interestingly, the slope increases with posture. While the lines for both the seated and supine postures are almost identical in non-obese subjects, neural respiratory drive in obese subjects is increased more in the supine posture (eg, for a subject with a BMI of 50 kg/m2, neural respiratory drive increases from approximately 20% to 25% when supine).
In the supine position, the diaphragm, neck, parasternal intercostal and abdominal muscles were activated more in the obese subjects (table 2, fig 2). The correlation between EMGdi and BMI increased to R2 = 0.696 (p<0.001, fig 2). Oesophageal and transdiaphragmatic pressure swings increased while gastric pressure swings decreased slightly in both groups. Average end-expiratory baseline pressures (Poes, Pgas) were higher in obese subjects. The breathing pattern was similar in both groups. A PEEPi of 5.3 (3.6) cm H2O developed in the obese subjects in the supine posture (table 2, fig 3).

{kind=link}
{kind=link}
{kind=link}
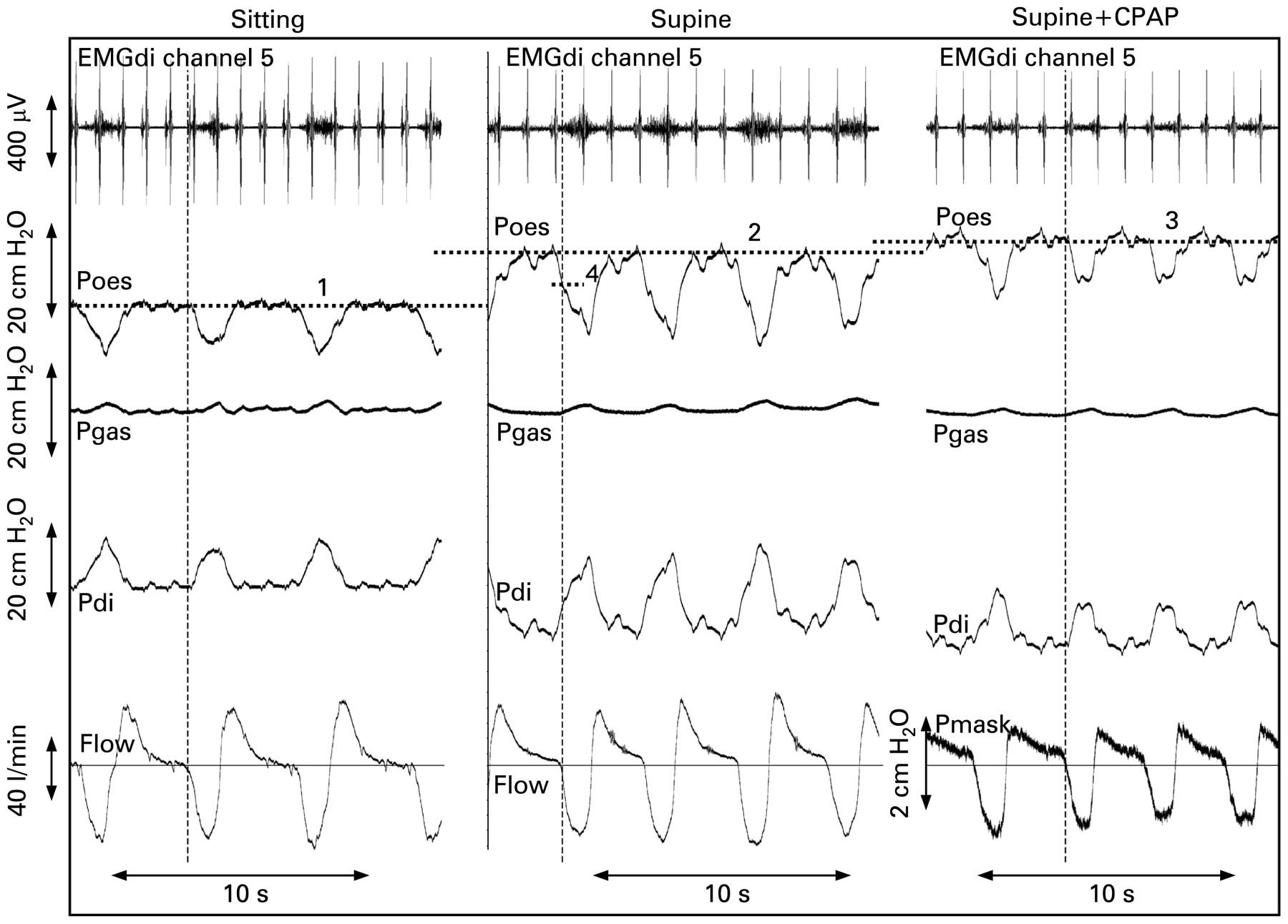
Resting breathing in an obese subject (body mass index 42 kg/m2, neck circumference 43 cm) when seated (left), supine without CPAP (middle) and with CPAP (right). The change in end-expiratory oesophageal baseline pressure is reflected by the horizontal dotted lines (nos 1–3). There is PEEPi of approximately 6 cm H2O (vertical lines indicate the start of inspiratory flow, difference between horizontal dotted lines 2 and 4 = PEEPi). Zero flow is indicated by the horizontal line. The right panel shows the same patient supine breathing with CPAP of 6 cm H2O (full facemask). Neural respiratory drive to the diaphragm increases when changing posture from sitting to supine and decreases with CPAP; PEEPi is offset with CPAP and pressure swings of Poes and Pdi are smaller. Note that on the lower right trace we do not measure flow but mask pressure because flow is predominantly inspiratory when receiving CPAP. The inspiratory deflection in mask pressure was chosen instead of flow to mark the beginning of inspiration (vertical line). CPAP, continuous positive airway pressure; EMGdi, electromyogram of the diagram (channel 5 records the biggest EMG signal, as described in the Methods section); Poes, oesophageal pressure; Pgas, gastric pressure; Pdi, transdiaphragmatic pressure (Pdi = Pgas – Poes); PEEPi, intrinsic positive end-expiratory pressure; EMGdi in μV, all pressures in cm H2O, flow in l/min.
The change from sitting to supine caused a significant increase in EMGdi, oesophageal and transdiaphragmatic pressure swings, and the development of PEEPi in obese subjects (table 2). The shift of end-expiratory oesophageal and gastric baseline pressures related to posture was not significantly different between the two groups. Extradiaphragmatic respiratory muscles were more activated in the obese group, both seated and when supine (additional information on the recruitment of extradiaphragmatic muscles is given in fig E2 in the online supplement). While oesophageal pressure swings became larger when supine, gastric pressure swings decreased with change in posture (table 2, fig 3). Neck circumference correlated with EMGdi%max when sitting (r = 0.545) and when supine (r = 0.660, both p<0.01), but was not an independent predictor of neural respiratory drive.
The quotient of ΔPdi/EMGdi was 0.67 (0.32) cm H2O/%maxEMGdi for the obese group when seated and 0.81 (0.35) cm H2O/%maxEMGdi when supine (p<0.001). The non-obese group had a ΔPdi/EMGdi quotient of 1.27 (0.61) cm H2O/%maxEMGdi when seated and 1.73 (0.88) cm H2O/%maxEMGdi when supine (p = 0.005). The difference between the obese and non-obese groups was significant in both the sitting and supine positions (both p<0.001).
The application of 7.3 (1.8) cm H2O CPAP to a subgroup of seven obese patients (all men, age 51.9 (15.6) years, BMI 37.8 (4.9) kg/m2) when supine led to a reduction of 40.1% (95% confidence interval (CI) 16.5% to 63.8%) in EMGdi, 26.4% (95% CI 13.0% to 39.5%) in oesophageal pressure swing and 25.3% (95% CI 14.3% to 39.0%) in transdiaphragmatic pressure swing. PEEPi in these subjects was reduced from 4.1 (2.7) cm H2O to 0.8 (0.4) cm H2O (p = 0.009) with CPAP (fig 3), similar to the level of PEEPi in non-obese subjects (table 2).
Regression analysis to establish independent predictors of PEEPi revealed an R2 of 0.480 (adjusted R2 = 0.471, standard error of estimate = 2.51); age, sex, neck circumference and waist-to-hip ratio were excluded (p = 0.443, p = 0.858, p = 0.641 and p = 0.327, respectively). The only significant parameter included in the analysis model was BMI (p<0.001) with an unstandardised coefficient of B = 0.205, SE = 0.028 (95% CI 0.149 to 0.262).
DISCUSSION
This study is the first to quantify neural respiratory drive in obesity. Obese subjects have markedly increased neural respiratory drive, 2–3 times that of non-obese subjects. The levels of neural drive in the obese subjects were similar to those reported in patients with moderate to severe respiratory disease.21 24 Similarly, oesophageal and transdiaphragmatic pressure swings were almost doubled. Increased neural drive is related to BMI and neck circumference. A change of posture from the sitting to the supine position leads to further increases in neural respiratory drive and transdiaphragmatic pressure swings in obese subjects. There is reduced efficacy of the diaphragm in obesity, as described by the quotient of transdiaphragmatic pressure per unit of diaphragm activation, which was half that of the non-obese group. Important for the increased work of breathing in obesity is the development of increasing PEEPi, on average 5 cm H2O when supine. The single independent predictor for the development of PEEPi was BMI; on average, PEEPi increased by 0.2 cm H2O per unit of BMI when supine. For the same ventilation, the obese group developed higher neural respiratory drive and larger pressures in the supine position, demonstrating reduced efficiency which confirms the observations of an earlier study.7
Interestingly, both groups generated larger oesophageal pressure swings for a given level of drive, contributing to the higher transdiaphragmatic pressure when lying supine, expressed by an increase in the quotient ΔPdi/EMGdi. There are several possible explanations for this observation. One is that the contribution of the non-diaphragmatic muscles is proportionately greater. In addition, the diaphragm may generate more tension when supine, acting through the zone of apposition because the contraction is relatively more isometric, although this is not supported by the tidal volume data which showed no significant change with posture. Lastly, because the supine posture induces a fall in lung volume, this results in increased pressure generation because of the length-tension relationship of the diaphragm. Available data show that functional residual capacity does fall in the supine posture,8 30–32 and this is a plausible explanation.7
Clinical significance of findings
Sinderby and colleagues used a similar electrode for the measurement of EMGdi.21 They found values for neural respiratory drive of 8.4 (2.5)%maxEMGdi in normal subjects, 43.4 (22.1)%maxEMGdi in patients with severe COPD (mean (SD) FEV1 0.69 (0.19) l, mean FEV1 28% predicted) and 45.1 (22.8)%maxEMGdi in patients with severe restrictive lung disease after prior poliomyelitis infection. Our group found that EMGdi was 27.9 (9.9)%max in a group of 30 COPD patients (mean (SD) FEV1 34.8 (13.9)% predicted).24 In the 30 non-obese subjects, neural respiratory drive was 8.4 (4.0)%maxEMGdi when seated and 7.0 (3.4)%maxEMGdi when supine. The level of neural respiratory drive in obesity (21.9 (9.0)%maxEMGdi when seated and 24.7 (8.2)%maxEMGdi when supine) reflects the high load on the ventilatory system and its increase when supine. These observations emphasise the severity of the impact of obesity on the ventilatory system, which is comparable to that in patients with moderately severe lung disease.
The high levels of neural respiratory drive in obesity result in a reduction in ventilatory reserve. Lourenço11 investigated hypercapnic and normocapnic obese subjects when seated and measured the increase in EMGdi during carbon dioxide breathing. Interestingly, the hypercapnic patients had a significant lower increase in EMG activity than the normocapnic patients. Lourenço concluded that an inability to increase the activity of the respiratory muscles, reflecting reduced reserve, could play a major role in the genesis of ventilatory failure.
CPAP applied to obese subjects when supine can offset PEEPi. With appropriate CPAP levels, inspiratory flow starts with the onset of the intrathoracic pressure swing. We found that CPAP reduced inspiratory pressure swings by 25% and neural respiratory drive by 40%. The efficacy of CPAP is likely to be due to its known volume-inflating effect, causing obese subjects to breathe at higher functional residual capacity. The observation that obese subjects recruit inspiratory capacity and dynamically increase end-expiratory lung volume during exercise to optimise pulmonary mechanics, reduce expiratory flow limitation and accommodate increased load without increased breathlessness33 supports this hypothesis. In addition, the finding of Pelosi and colleagues4 that CPAP is helpful to support ventilation in obese patients during anaesthesia, while normal subjects do not benefit, is consistent with our observations. However, despite offsetting PEEPi with CPAP, obese subjects still had markedly raised levels of EMGdi and oesophageal and transdiaphragmatic pressure swings compared with normal subjects. Besides the increased abdominal load anxiety, an increase in Paco2 and low maximum oxygen uptake are factors that may have contributed to increased neural respiratory drive.
Interestingly, Yamane et al34 recently reported in 30 Asian patients that the levels of Pao2 and Paco2 in the inferior pulmonary veins are related to BMI in the supine posture, suggesting that tidal breathing in more obese subjects is close to the “closing volume”.30 35 36 They concluded that the inverse relationship between BMI and Pao2 in the inferior pulmonary veins was a subclinical manifestation of obesity-related respiratory insufficiency. This observation is consistent with our finding that the supine posture imposes an additional load on the ventilatory system in obesity. BMI was the only parameter associated with low Pao2 in the study by Yamane and colleagues,34 and it was closely related to PEEPi and increased neural respiratory drive in our study.
Limitations of the study
There are several factors which make the measurement of true intrathoracic pressure with an oesophageal balloon difficult, and there is a well recognised artefact in the supine posture. Inspiratory flow can only start when intrathoracic pressures are subatmospheric, but measuring the oesophageal pressure at the onset of flow shows it to be positive when supine. The increase in end-expiratory oesophageal baseline pressures when supine was about 7–9 cm H2O in our study, similar to the results of earlier studies.6 37 Importantly, this artefact was the same in the obese and non-obese groups. The shift in baseline pressures is partly due to a displacement on the pressure-volume curve and, in part, it is likely that the mediastinum compresses the oesophageal balloons in the supine posture.6 8 37–39 Interestingly, the difference in end-expiratory gastric pressure between the obese and non-obese groups (around 5.0 cm H2O) was similar to the results of Sampson and Grassino.12 The finding that changes in the end-expiratory pressure were the same in both groups while EMGdi and oesophageal pressure swing increased much more in the obese subjects make it highly likely that these observations are documenting a true increase in the ventilatory load. However, lung volume may directly affect efficiency, as measured by the quotient of ΔPdi/EMGdi, and it is possible that the differences between obese and non-obese subjects could be smaller than observed if corrected for lung volumes.
The obese group in this study was matched to the non-obese group for sex, height and smoking status. However, the obese subjects were slightly older than the non-obese subjects, which could potentially contribute to differences in neural respiratory drive. The physiological impact of ageing—including stiffening of the rib cage and development of mild emphysema—may cause a slightly higher respiratory drive.40 Lung compliance worsens with age and, because they were somewhat older, would be expected to be slightly reduced in the obese group. However, as described by Jolley et al,24 neural respiratory drive in normal subjects increases only slightly with age—on average to 11.3 (3.4)%maxEMGdi in those aged >50 years—and therefore a small difference in age (12 years) as reported in our study would have little effect.
CONCLUSION
Obese subjects have increased neural respiratory drive which is 2–3 times that of non-obese subjects and comparable to that of patients with moderately severe lung disease. The increased neural respiratory drive is strongly related to BMI. Neural respiratory drive in obese subjects increases when changing from the sitting to supine position, while in normal subjects the same level of drive is sustained. In obese subjects PEEPi develops when supine, and this can be offset with CPAP which substantially reduces respiratory drive. CPAP therapy may therefore have a role in the clinical management of severely obese patients when supine. Obesity causes breathlessness and eventually ventilatory failure. Future studies could address the interaction of levels of neural respiratory drive, breathlessness and ventilatory failure, as well as the impact of weight loss.
Acknowledgments
The authors thank Professor Neil Pride for his help with the manuscript and Dr Gerrard Rafferty for his statistical advice.
REFERENCES
Supplementary materials
Web only appendix 64:8;719
Files in this Data Supplement:
Footnotes
Competing interests: Professor Yuanming Luo, a close collaborator from the State Key National Laboratory of Respiratory Disease, Guangzhou Medical College, China, has developed the multipair catheter used for the measurement of the diaphragm electromyogram. No patent is pending.
Funding: JS is the recipient of a long-term Research Fellowship of the European Respiratory Society (No 18).
Ethics approval: The study was approved by the King’s College Hospital local research ethics committee and informed consent was obtained from each patient.
▸ Additional data are published online only at http://thorax.bmj.com/content/vol64/issue8