Article Text

Abstract
Background: Non-invasive ventilation is first-line treatment for patients with acutely decompensated chronic obstructive pulmonary disease (COPD), but endotracheal intubation, involving admission to an intensive care unit, may sometimes be required. Decisions to admit to an intensive care unit are commonly based on predicted survival and quality of life, but the information base for these decisions is limited and there is some evidence that clinicians tend to be pessimistic. This study examined the outcomes in patients with COPD admitted to the intensive care unit for decompensated type II respiratory failure.
Methods: A prospective cohort study was carried out in 92 intensive care units and 3 respiratory high dependency units in the UK. Patients aged 45 years and older with breathlessness, respiratory failure or change in mental status due to an exacerbation of COPD, asthma or a combination of the two were recruited. Outcomes included survival and quality of life at 180 days.
Results: Of the 832 patients recruited, 517 (62%) survived to 180 days. Of the survivors, 421 (81%) responded to a questionnaire. Of the respondents, 73% considered their quality of life to be the same as or better than it had been in the stable period before they were admitted, and 96% would choose similar treatment again. Function during the stable pre-admission period was a reasonable indicator of function reported by those who survived 180 days.
Conclusions: Most patients with COPD who survive to 180 days after treatment in an intensive care unit have a heavy burden of symptoms, but almost all of them—including those who have been intubated—would want similar intensive care again under similar circumstances.
Statistics from Altmetric.com
An acute exacerbation of chronic obstructive pulmonary disease (COPD) is a common reason for hospital admission, and although non-invasive ventilation is the recommended first-line treatment for decompensated type II respiratory failure, on occasions endotracheal intubation may be required.1 Decision making about intubation should involve some understanding of the likely probability of survival, and also of the quality of life that survivors can expect. This information will be most useful if it comes from systematic studies of survivors, who provide both assessments of their own quality of life and their views about the acceptability of their treatment. There are some data from the USA2 but very few from the UK, which has historically had fewer intensive care unit (ICU) beds per unit population and may have different admission policies and practices. A simulation study carried out in one Critical Care Network in the UK suggested that, for patients with COPD with a given set of characteristics and preferences and subject to identical resource constraints, there was variation in decision making about whether intubation was appropriate, partly because of widely differing estimates of the probability of survival.3 Moreover, an analysis of actual decision making in the UK suggested that clinicians tended to be pessimistic about survival.4 In order to provide both clinicians and patients with better information about outcomes for COPD after critical care, this study reports the survival, quality of life and future treatment preferences of patients in the COPD and Asthma Outcome Study (CAOS) study.
METHODS
Intensive care units and subjects
All ICUs participating in the UK Case Mix Programme (CMP)5 and three respiratory high dependency units (HDUs) in hospitals with ICUs were invited to take part in the study. Patients were eligible if they were admitted to a participating unit with breathlessness, respiratory failure or change in mental status due to an exacerbation of obstructive lung disease. They were recruited on admission to the unit. Clinicians were asked to classify the patient as having either COPD, asthma or a mixture of the two, because the precise classification of obstructive airways disease can be difficult at the time decisions about admission to ICU have to be made, but even an imprecise diagnosis may have prognostic value. Clinicians found this classification easy to use in the clinical setting.
Patients under the age of 45 years were excluded as it was expected that they would be admitted irrespective of prognosis. Patients were also excluded if they had had surgery within the past 10 days or had been transferred from another hospital. Data were collected for admissions between March 2002 and September 2003 with follow-up for 180 days after ICU admission.
Collection of data
Data were sought about each patient’s function during the period of stability 2 weeks before admission using a 4-point scale,6 and standard questions were asked about activities of daily living.7 Clinicians were asked to use the EuroQol visual analogue score (VAS)8 to predict the patients’ self-rated quality of life at 180 days if they were to survive.
When a patient was discharged from a unit or died while in it without having been intubated, clinicians were asked whether intubation had been ruled out as a treatment option if medical treatment and non-invasive ventilation were to fail or had failed. This information was used to divide the patients into three “intubation status” groups: (1) intubation not needed; (2) intubated; and (3) not to be intubated. This last group included those for whom clinicians felt intubation to be futile and patients who declind treatment escalation.
Actual survival to 180 days was determined initially from the general practitioner and confirmed by the Office of National Statistics. A follow-up questionnaire was sent to patients who survived 180 days which included the 4-point functional score used on admission, the Euroqol profile and VAS, the AQ-20,9 and how their current state of health compared with their health during the period of stability before hospitalisation. In addition, to understand how patients felt about their experience of the ICU and intubation, they were asked: “Under the same circumstances, would you be willing to undergo similar intensive care treatment again?”
Data for the participating ICUs and others were also obtained from the CMP database.
Analysis of data
Data from the study were compared with extracts from the CMP database to assess how representative of the UK were the ICU/HDUs and patients recruited. Data from the CMP were also used to indicate the variation between units in admission policies.
Survival rates and quality of life on follow-up were examined overall and for the three “intubation status” groups. Clinicians’ predictions of quality of life among 180-day survivors were compared with the survivors’ assessments, and functional status in the 2 weeks before admission was compared with survivors’ reports.
Analyses were carried out using Stata Version 9 (Stata Corp, College Station, Texas, USA).
RESULTS
Units and patients recruited
Of the 239 ICUs in the UK in January 2002, the 177 contributing to the CMP database at the time were invited to take part. Three were ineligible because they were specialist units that never admitted patients with COPD, 73 refused, 3 did not complete the ethics process and 6 recruited no patients. Thus, 92 ICUs actively participated in the study, 38.5% of the units in the UK and 52.0% of those invited. Three respiratory ICUs also participated.
For 89 of the 92 ICUs, data were available from the CMP database to allow comparison with non-participating units. The units actively participating were similar to others in terms of type, size and affiliation, and the mean percentages of admissions potentially eligible for the study (table 1). The CMP database also allowed comparisons of the patients recruited with those eligible but not recruited in the participating units (table 2). A total of 832 patients were recruited, 724 to ICUs and 108 to respiratory HDUs. At the time of these analyses there were data in the CMP dataset for 648 of the 724 (94.5%). These 648 were compared with the 996 patients in the dataset admitted to participating ICUs and satisfying the inclusion criteria but not recruited. There were no differences in terms of age (Z-test, p = 0.49), COPD acute physiology score10 (Z-test, p = 0.96) or ICU survival (χ2 0.77, p = 0.38).
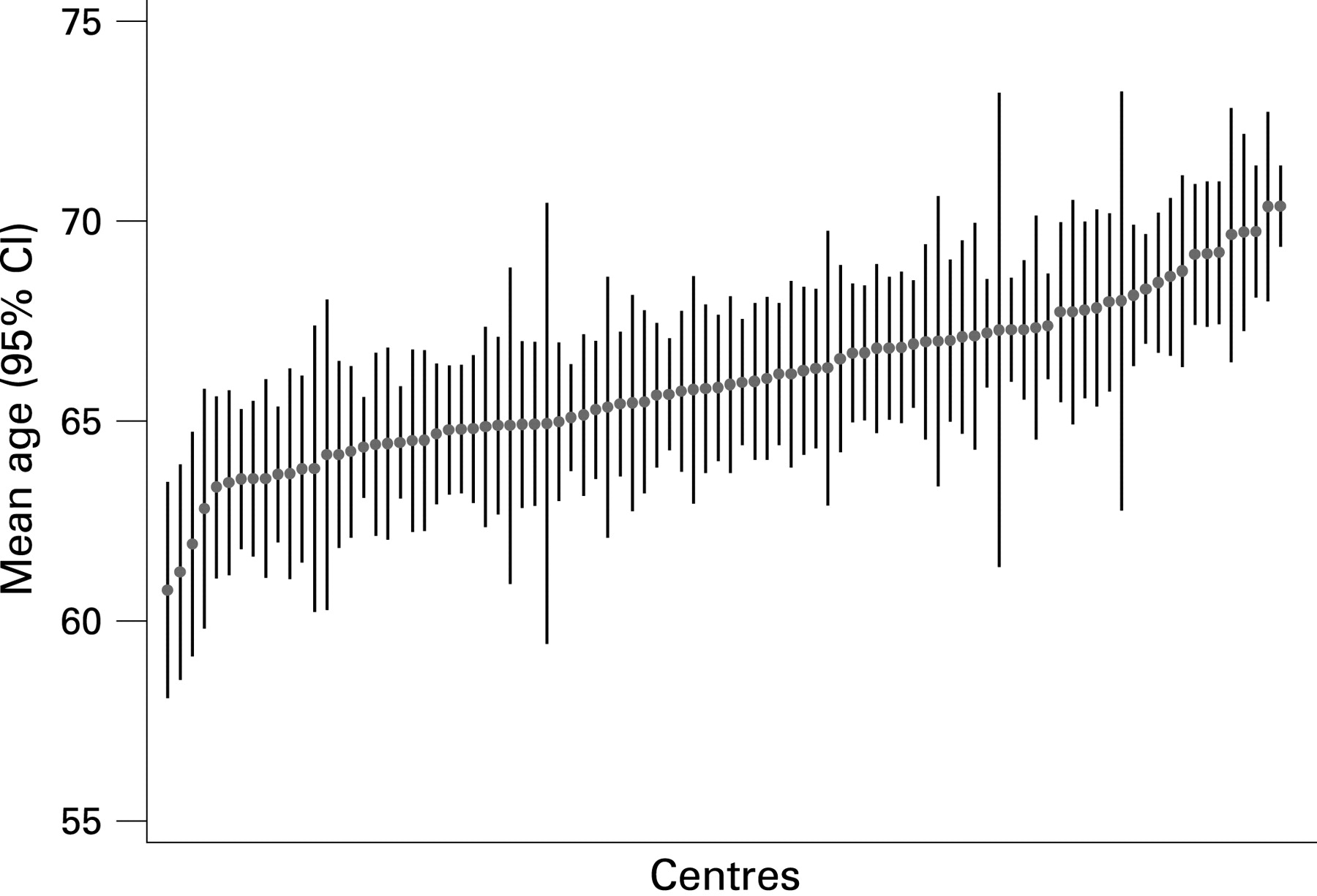
The CMP database had data on 8717 patients who met the CAOS study inclusion criteria and were admitted during the period 2000–6 to the ICUs in the CAOS study. The participating centres are plotted from left to right by increasing mean age in fig 1 and by increasing percentage of admitted patients in the most limited classification of baseline respiratory impairment in APACHE II in fig 2. These diagrams suggest between-unit variation in the age and fitness of patients admitted. This may be partly due to variation between catchment populations, but it also suggests that some units are more selective than others about which patients with COPD/asthma they admit.


{kind=link}
{kind=link}
Ventilation and length of stay
Of the 832 patients recruited, 81.3% were admitted only to the ICU. 54.1% were intubated before or during ICU admission, 36.5% were not intubated but had non-invasive ventilation, and 8.1% had medical treatment only. For 201 (53%) of the non-intubated patients, medical treatment and non-invasive ventilation were sufficient to manage the exacerbation (“intubation not needed”), but in the other 47% the patients were designated “not to be intubated”.
Baseline differences between intubation status groups are given in table 3. In the intubated and intubation not needed groups the patients have been subdivided into those with COPD or a mixture of COPD and asthma (labelled “COPD±”) and those diagnosed on admission as “pure asthma”. (In the “not to be intubated” group there were only two patients with pure asthma, and only one who responded to the 180-day questionnaire, so this group was not subdivided.) In table 3, as elsewhere, the numbers in the intubation not needed/pure asthma subgroup were small and so the parameter estimates will be very imprecise. Of the patients designated “not to be intubated”, 57% had been admitted directly to the ICU. They tended to be older than the others (mean age 70.3 vs 66.1 years, t test, p<0.001) and had slightly lower mean COPD acute physiology scores (26.4 vs 28.4, t test, p = 0.03). They had much lower functional scores (housebound or worse 68.0% vs 30.0%, χ2 test, p<0.001), and 75.1% were either housebound or on long-term oxygen or both compared with 32.7% in the intubated group.
The intubated patients had longer stays than the others, both in the COPD± and the pure asthma subgroups.
Survival
Survival rates at discharge from the ICU and from hospital and at 180 days after ICU admission are given in table 3. Overall, 517 (62.1%) survived to 180 days. Survival rates were highest in patients who did not need intubation and lowest in those designated “not to be intubated”, but the differences in survival between the intubated COPD± and the “not to be intubated” groups were quite small, with overlapping confidence intervals. The intraclass correlation for actual survival rates between participating units was 0.017 (95% CI 0.000 to 0.057), so no adjustment was made to the confidence intervals for unit-level effects.
Quality of life at 180 days
Of the 517 subjects who survived to 180 days, 420 (81.4%) returned the follow-up questionnaire. The median (IQR) time from admission to the ICU to return of the questionnaire was 231 days (200–399). There was no evidence for a difference in the percentage of survivors returning the questionnaire between the five groups examined (see table 4 available online). Overall, 73% of respondents stated that their current state of health was the same as or better than before hospitalisation; the figures for the 184 prompt responders (<220 days after admission), 179 delayed responders (221–365 days) and 57 very delayed responders were 71%, 75% and 70%, respectively, giving no indication that non-responders might have responded markedly differently (p = 0.81, χ2 test).11
Table 4 (online) also gives results from the EuroQol schedule. For example, 62% of the respondents experienced moderate or extreme discomfort and 56% had some anxiety/depression, 7% rating this as extreme. Generally, the quality of life in the not-to-be-intubated group was poorer than for the rest. On the EuroQol VAS (0 = “worst possible health state”, 100 = “the best imaginable health state”) the overall mean (SD) rating was 54.9 (19.5); 75% rated their health state as at least 40 and 50% rated it as at least 50.
The AQ-20 questionnaire gives more detail about the symptoms associated with airways disease and table 5 (available online) summarises the data from the 420 respondents. The question on doing things at work was only answered by 59 people so the results are unreliable and are only included for completeness. The p values are for χ2 tests of the hypothesis of no difference in the percentages between intubation status groups. 42.7% of the respondents reported feeling breathless when trying to get to sleep. Only 16% of those who considered the question applicable could get upstairs without breathlessness, 74% had difficulty getting around the house because of their chest trouble, and 83% felt that the fullness of their lives was limited by their chest troubles. For the AQ-20 score, which has a range of 0–20, the mean (SD) and median (IQR) scores were 11.2 (4.7) and 12 (8–15), respectively.
Willingness to undergo similar treatment in the future
In spite of this burden of symptoms and disabilities, 96% of the 415 who answered the question about whether they would be willing to undergo similar treatment again under the same circumstances said that they would. In the 212 intubated patients the percentage was the same. Even under the worst-case assumption that all non-responders would not want ICU admission again, 204 of the 263 who survived to 180 days (78%) would have wanted it. There was no significant difference in this respect between patients with COPD± and those in the “pure asthma” category.
Predictors of quality of life on follow-up
Patient-reported function in the follow-up questionnaire was slightly worse at 180 days than pre-admission function collected from either the patients themselves (45%) or other witnesses (55%) at admission to the ICU. Overall, about one-half scored the same, about one-third were worse and about one-sixth were better. More detail on the changes in reported function for each pre-admission functional category is given in table 6. The actual agreement between function before admission to the ICU and on follow-up was quite low (kappa = 0.21, p<0.001), but the correlation between the two (and therefore the discriminatory power of pre-admission function) was reasonably good (Spearman rank coefficient = 0.485, p<0.001), so pre-admission functional status gives clinicians useful information about likely status on follow-up. As a rule of thumb, those who were housebound before admission will probably be the same at follow-up, but the most common (and equally likely) outcome for those who were fully mobile or independent is that they will stay the same or fall one category.
Doctors’ predictions of quality of life at 180 days made on admission using the EuroQol VAS were slightly pessimistic compared with the patients’ reported scores in the follow-up questionnaire (mean predicted score 50% vs 55%). In spite of using 100 scale points rather than the 4 on the function scale, discrimination was relatively poor (Spearman rank coefficient = 0.221, p = 0.0004). Agreement after converting both VAS scores into quartiles was also poor (kappa = 0.052, p = 0.032).
DISCUSSION
Limitations of study
This study recruited patients with COPD, asthma or a mixture of asthma and COPD who were admitted to ICUs or HDUs in the UK with an episode of respiratory failure. The participating units and patients recruited appear to be representative of UK practice, and the rate of follow-up was good. In these respects the results should be generalisable and valid within the UK at least.
Importantly, however, all the patients in this study were selected for either ICU or HDU admission. Of the whole “population” of patients admitted to hospital with severe acute exacerbations of COPD, we would expect to have recruited relatively few on long-term oxygen and/or with low functional scores. (In one centre 48.9% of all hospitalised patients with COPD were housebound or worse compared with 38.2% in this study.12) Our overall results may therefore be least applicable to such patients. However, fig 1 suggests that the units taking part in the study had highly variable admission thresholds. The spectrum of those recruited—if not representative overall—was broad, with substantial numbers of patients with low functional scores, especially in the “not to be intubated” group. The results for subgroups are therefore of interest.
Assignment of the patients to diagnostic groups was based on clinical judgement at the time of admission. We cannot be certain that those classified as “pure asthma” really did have asthma or whether some of the younger patients, for example, had COPD. However, the 180-day survival rate for the COPD± group was approximately 60% compared with around 90% for the “pure asthma” group. Also, these diagnostic categories were significant predictors of prognosis in a multivariate prognostic model that took account of factors such as age and functional status.13
Comparison with other studies
On a scale of 0–100, the mean rating by survivors of their overall quality of life was 54.9, significantly less than VAS scores for members of the public aged 65–74 years (mean 77.3)14 but similar to the mean (SD) score of 50.9 (16.4) for 132 outpatients with COPD of mean age 67 years and mean forced expiratory volume in 1 s 47% attending a chest clinic.15
Although they reported widespread discomfort and disability, around 75% of the responding survivors considered their quality of life to be similar to or better than it had been in the stable period before they were admitted, and over 95% of them would choose similar treatment again. This is broadly consistent with the results of an earlier study in which 87% of 81 patients with COPD of mean age 75 years said they would accept a “high burden” of treatment if it was life-saving and restored current health.16
In an earlier analysis we found that clinicians appeared to be pessimistic about the probability of survival of patients with COPD on admission to ICUs.4 This was also found in the SUPPORT study.2 Here we report that clinicians’ predictions of the quality of life of survivors were undiscriminating as well as slightly pessimistic, but that functional status in the period of stability 2 weeks before ICU admission was a reasonable discriminator, if a slightly optimistic predictor, of function in the longer term. Again, these findings are consistent with results from other studies. Frick et al17 in the USA found that neither doctors nor nurses could predict outcomes well, and the SUPPORT study showed that functional status before ICU admission was a better indicator of longer-term function than doctors’ predictions.18
This is the largest study to have systematically collected data on outcomes for patients with airway obstruction admitted to ICUs in the UK. Over 60% survived for at least 180 days after ICU admission and, even among the relatively sick group who were “not to be intubated”, 180-day survival was almost 50%. Functional capacity in the period of stability in the 2 weeks before hospital admission is a reasonably discriminating indicator of function at 180 days. Although survivors still had impaired quality of life, almost all of them would have wanted similar treatment again. We think that these findings should inform decision making for patients who are being considered for intubation.
Acknowledgments
The authors thank all the CMP units that participated in the study for recruiting the patients to make the study possible; the Intensive Care National Audit and Research Centre for their invaluable role in recruiting units and data linkage; and Jan Van Der Meulen for advice on the data analysis.
REFERENCES
Supplementary materials
web only appendix 64/2/128
Footnotes
▸ Tables 4 and 5 are published online only at http://thorax.bmj.com/content/vol64/issue2
Contributors: MJW, CS, KR, JA, BR and DY were involved in the original design of the study. MJW coordinated the study and carried out the initial data analysis and drafting of the paper. JG helped to collect the data. CS carried out additional analyses and drafted the final paper. KR and DH helped recruit the units and facilitated data linkage with the CMP. All the authors revised the manuscript critically for important intellectual content and approved the final version. MW is the guarantor.
Funding: MW was funded by an MRC Health Services Research Fellowship. JG was funded by an NHS R & D grant. The funder had no role in the design, analysis, interpretation or reporting of this research.
Competing interests: None.
Ethics approval: The study had multicentre research ethics committee approval.
Linked Articles
- Airwaves