Article Text

Abstract
BACKGROUND Surgical resection is the recognised treatment of choice for patients with stage I or II non-small cell lung cancer (NSCLC). In the UK surgical resection rates have remained far lower (<10%) than those achieved in Europe and the USA (>20%), despite the recent introduction of fast access investigation units. It remains unclear therefore why UK surgical resection rates lag so far behind those of other countries.
METHODS A new quick access two stop investigation service was established at Papworth in November 1995 to investigate all patients presenting to any of three surrounding health districts with suspected lung cancer. Once staging was complete, all patients with confirmed lung cancer were reviewed by a multidisciplinary team which included an oncologist and a thoracic surgeon. Time from presentation to definitive treatment and surgical resection rates were reviewed.
RESULTS Two hundred and nine (76%) of a total of 275 consecutive patients investigated had confirmed lung cancer (28 small cell, 181 non-small cell). Of the remainder, eight patients (2%) had metastatic disease, four (1%) had other thoracic malignancy (thymoma, mesothelioma), four patients (1%) had benign thoracic tumours, and 50 (18%) had other non-malignant diseases. Of the 181 patients with non-small cell primary lung cancer, 47 (25%) underwent successful surgical resection, of whom 59% had stage I and 21% stage II disease. The failed thoracotomy rate was 11%. Median time from presentation at the peripheral clinic to surgical resection was 5 weeks (range 1–13).
CONCLUSION Quick access investigation, high histological confirmation rates, routine CT scanning, and review of every patient with confirmed lung cancer by a thoracic surgeon led to a substantial increase in the successful surgical resection rate. These results support the growing concern that many patients with operable tumours are being denied the chance of curative surgery in our present system.
- lung cancer
- surgical resection rate
Statistics from Altmetric.com
Standards for the investigation of patients with lung cancer vary widely despite the recent publication of recommendations by the Working Group of the Standing Medical Advisory Committee1and by a National Workshop organised in 1993 by the British Thoracic Society, the Royal College of Physicians, and by the York Health Economics Consortium.2 Regional guidelines have also recently been developed in the Anglia and Oxford region, derived from a series of study days organised to plan for the implementation of the Calman Cancer Report. Surgery remains the treatment of choice for patients with early stage lung cancers.3
The annual national summary of resections for lung cancer carried out by all UK cardiothoracic surgeons shows a stable figure of 10%.4 In East Anglia the estimated resection rate is also around 10%, although in the Oxford region surgical resection rates as low as 1% have been reported in some areas where there is no designated respiratory physician. The UK surgical resection rate compares with a resection rate of 28% from a national survey in the USA,5 although the latter was derived from tumour registries only of hospitals with approved cancer programmes. European resection rates are also reportedly higher than in the UK,6 a fact which has previously been attributed to a younger age distribution, less aggressive tumours, or more aggressive surgical treatment of advanced disease.
Recent guidelines stress the importance of avoiding delay in arranging investigations for patients with suspected lung cancer. A previous study from this hospital found the mean interval from first presentation to surgery was 109 days, of which 58 days were taken up with diagnostic and staging investigations.7 Although there is no evidence to suggest that management delays adversely affect clinical outcomes, it seems likely that some patients with borderline operable tumours at presentation will become inoperable.
It is also well recognised that elderly patients with lung cancer are less likely to be seen by a chest physician than younger patients, an important fact since predictions from Regional Registry Data suggest that, by the year 2000, it is likely that more than 40% of patients in the UK will be aged over 75.8 This is particularly relevant since evidence suggests that the capacity to benefit from treatment is similar across the age bands.9 Histological confirmation rates for lung cancer also tend to be much lower for patients over 75 than for younger patients. One comprehensive regional survey found that only 39% of patients over 75 had had their diagnosis confirmed histologically compared with 82% of patients under 60 years of age.8 Overall rates of histological diagnosis also compare very unfavourably with other sites of cancer where it is not unusual to find rates of over 90%. The Yorkshire Cancer Registry mean for all sites in 1990–2 was 81%, with the rate for lung cancer being lowest at 64% compared with 79% for stomach cancer which has a similarly poor prognosis.
The five year survival rate for all stages of lung cancer in England and Wales is 6%. Survival rates are reported as being considerably higher in other European countries,10 although it is not known whether this is due to a more active investigation and management programme, sampling error, or different age distribution or severity of disease. As a result of reorganisation in our regional centre we have recently set up a “two stop” investigation and management service for all patients presenting with suspected lung cancer in the three surrounding health districts. This paper presents the results of the first year (November 1995 to December 1996) and assesses whether a more active, streamlined, uniform investigation protocol improves the rates of active treatment with the potential for an effect on long term survival.
Methods
All patients presenting with suspected lung cancer to each of three district general hospitals (Addenbrooke’s Hospital, Cambridge; Hinchingbrooke Hospital, Huntingdon; and West Suffolk Hospital, Bury St Edmunds) were investigated in a standardised way via a “two stop” investigation and management service recently established at Papworth Hospital, the regional centre. Patients are initially seen by one of nine respiratory physicians serving these three hospitals in the local clinic and then referred for further investigation at Papworth. History, examination, blood tests, spirometric tests, and consent for further investigations (both fibreoptic bronchoscopy and fine needle lung biopsy) are obtained in the district general hospital clinic and the admission date (within 10 working days) obtained by a telephone call to the investigation co-ordinator at Papworth. Patients are told that the diagnosis of lung cancer is either “possible” or “probable”. Patient notes and radiographs are subsequently reviewed at Papworth by the designated respiratory physician and a specialist respiratory radiologist when the need for other staging investigations such as ECG, exercise test, echocardiography, bone scan, brain CT scan, full lung function testing, and blood gas tensions are identified. Patients can also be admitted to the “two stop” service via inpatient referrals to the nine chest physicians at the three district general hospitals. In addition, a quick access clinic has been established at Papworth which allows patients to be seen by a chest physician within the standard of 10 working days should the peripheral clinics be overbooked. Some patients from other health authorities have also been referred. All GPs in the three health authorities were informed of the change in practice and were encouraged to send all patients to their local respiratory physicians for initial assessment. A series of road shows and meetings have been arranged for GPs, general physicians, and geratricians to encourage them to refer patients into the service via their local respiratory physician.
On the investigation day patients are asked to provide their own transport if possible and to bring a relative or friend to stay with them. On arrival patients are assessed by a nurse, and only seen by a junior doctor if any change in symptoms or medication has occurred since the visit to the peripheral clinic. The patients are then seen by the specialist Macmillan nurse (EL) who attempts to identify any psychological or social problems likely to require early intervention.
Patients initially all undergo a staging CT scan of the thorax, upper abdomen and adrenal glands. After discussion between the designated respiratory physician (CL) and respiratory radiologist (RC) they either undergo fibreoptic bronchoscopy or fine needle lung biopsy, depending on whether the lesion appears to have an endobronchial component on CT scanning or not. CT scans are performed using a modern spiral scanner (Somatom Plus 4, Siemens, Erlangen). Spiral scans of the thorax are obtained before and after intravenous contrast medium with the scan following the contrast medium being acquired with 3 mm thick sections through the airway. The post-contrast images of the liver and adrenal glands are also obtained. Other tests such as lung function, ECG, echocardiography, etc are usually performed immediately after staging CT scanning. Patients who undergo bronchoscopic examination are sedated with midazolam (up to 7 mg) intravenously with no premedication and are allowed home later in the day. Patients from whom lung biopsy specimens are taken are given no sedation/premedication except those assessed as being particularly anxious who are also given midazolam intravenously. Fine needle lung biopsy specimens are all taken by the radiologist under CT guidance, and patients are discharged after a check chest radiograph four hours later.
Patients in whom the CT scan shows no intrapulmonary or endobronchial lesion are referred for appropriate alternative investigations—for example, mediastinoscopy for isolated nodal enlargement—as required. Patients identified as having pleural disease only undergo CT guided pleural aspiration and biopsy if significant localised pleural thickening is present, or are referred for thoracoscopic pleural biopsies if more appropriate.
Progress through the investigation day is documented via a multidisciplinary integrated care pathway which was drawn up prior to the onset of the two stop investigation service. This pathway facilitates audit by allowing routine collection of patient information and by providing a means of monitoring variances from the identified protocol of care and investigation.
Three days after the investigation day all patients (up to nine patients) are reviewed by the multidisciplinary team which comprises chest physician(s), radiologist(s), thoracic surgeon(s), specialist respiratory pathologist(s), specialist lung cancer oncologist, and Macmillan nurse, as part of the regular weekly clinicopathological conference held at Papworth. At this meeting the possibility of surgical resection, need for further surgical staging procedures or further histological investigation, or need for other presurgical investigation is discussed and agreed and documented in the patient’s notes. The patients are then recalled to either a follow up clinic later that morning or four days later to receive their diagnosis and management plan.
In the follow up clinic patients requiring chemotherapy or radiotherapy receive their diagnosis from the lung cancer oncologist (AP, DG) who subsequently arranges their treatment at the local radiotherapy centre at Addenbrooke’s hospital. Patients being referred for surgery or with a non-malignant disease are seen either by the oncologist or by the designated respiratory physician. The Macmillan nurse sits in on approximately two thirds of consultations, while a trained clinic nurse sits in on the remainder. Following the consultation the specialist nurse sees the patient separately to provide clarification, if necessary, and an empathic response to the distress of hearing bad news. She then makes a brief assessment of immediate needs. Patients are given written information concerning their treatment or intended surgery. In some instances surgical nurses are available to explain more details of the surgery. All patients are given the telephone number of the Macmillan nurse to contact with any subsequent queries. The patient’s GP is contacted either by telephone or fax on the day of the clinic to inform him of the patient’s diagnosis and management plan. A full typed summary follows within 14 days.
Results
Two hundred and seventy five patients were investigated in the 13 month study period, 171 men and 104 women. Their mean age was 69 years (median 74 years; mode 69 years; range 61–88 years). Investigations performed on these patients are shown in fig 1. In 38 patients the CT scan showed no evidence of malignancy and, as there was no other indication to justify bronchoscopy, no further investigations were performed that day. These patients were discharged back to the referring respiratory physician for further follow up.

Investigations performed at “two stop” lung cancer clinic.
In 14 patients the CT scan showed no endobronchial or intrapulmonary disease, but there was evidence of either mediastinal lymphadenopathy or pleural disease. These patients were referred for mediastinoscopy, thoracoscopy, or underwent a cutting pleural biopsy under CT scanning as appropriate.
In 124 patients the CT scan suggested that a diagnosis could be obtained bronchoscopically. In the remaining 99 patients a fine needle lung biopsy specimen was taken. If both routes were possible, bronchoscopic examination was performed preferentially as a preliminary audit suggested it was better tolerated by patients and it avoided the risk of pneumothorax.
Fifty patients (18%) were found to have other diseases—for example, resolving pneumonia, sarcoidosis, rheumatoid lung disease, benign pleural thickening, tuberculosis, lung abscess, pulmonary calcification, pulmonary fibrosis, bronchiectasis, pulmonary emboli, emphysema, asthma, idiopathic hemidiaphragm paralysis. Four patients were found to have other thoracic tumours (one endobronchial hamartoma, one paraganglioma, two carcinoid) and were referred for surgical resection.
The remaining 221 were confirmed as having malignant disease: 209 patients had primary lung cancer (181 non-small cell, 28 small cell), eight patients had metastatic disease (primary sites breast, thyroid, colon, prostate), three patients had mesothelioma, and one had malignant thymoma.
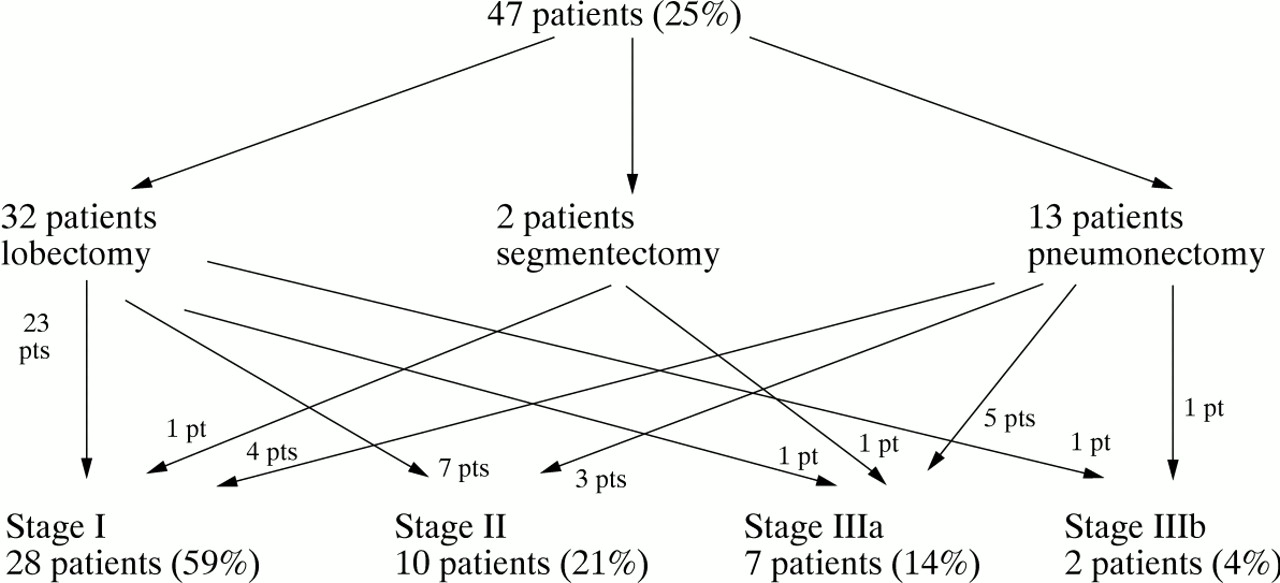
Of the 181 patients with non-small cell primary lung cancer, 16 patients (9%) underwent further surgical staging procedures after the first investigation day (fig 2). Of these, five patients underwent subsequent successful surgical resection and one underwent unsuccessful thoracotomy, despite negative mediastinoscopy. In all, 53 patients (29%, mean age 68 years, median 68 years, range 48–87 years) underwent thoracotomy: 32 (18%) underwent successful lobectomy, 13 (7%) pneumonectomy, and two segmentectomy (fig 3). There was only one postoperative death, a patient who died eight days after lobectomy. Resection was unsuccessful in six patients (11%), three because of unsuspected T4 disease, two with extensive unsuspected N2 disease, and one with chest wall invasive T3 disease too extensive for resection. Those in whom thoracotomy was unsuccessful were treated with radiotherapy with or without chemotherapy. One patient died one month after surgery and the remaining patients survived for 9–12 months. Presurgical staging of these patients is shown in figs 4 and 5. The overall successful resection rate was 25% with 38 patients (80%) being stage I or II (fig 6). Median time from presentation at the peripheral clinic to surgical resection was 5 weeks (range 1–13 weeks).

Diagnostic biopsies.

Surgical resection rates.

Presurgical staging of patients who underwent lobectomy.

Presurgical staging of patients who underwent pneumonectomy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patients undergoing surgical resection.
Discussion
The results of the first year of the Papworth two stop investigation service for lung cancer show that it is possible to increase surgical resection rates substantially by a more systematic investigation and review process. This compares favourably to other resection rates of 5–6% published recently elsewhere.11 ,12
Our results suggest that the higher resection rate is not due to a more aggressive surgical approach as 80% of patients had stage I or II disease, similar to that reported elsewhere.13 Similarly, the high resection rate was not due to our operating on more elderly patients as the average age of our surgical patients was also no different from that reported from elsewhere.13 The exact explanation for the dramatic increase in surgical resection rate is unclear. Of note is the fact that this increased rate was achieved immediately from the outset of the service. Possible explanations include: (1) quick diagnosis, within four weeks of GP referral, (2) high histological confirmation rate, (3) CT staging of every patient, and (4) surgical review of every patient.
In the study reported by Deegan in Nottingham14 only 8% of patients were referred for surgery despite a high diagnostic rate of 84% and fast track investigation. Our median time from presentation to resection represented a halving of our previously reported times7 and is comparable to that achieved in other reported fast track series.11-13 The two unique aspects of our service at present are the universal CT scan staging and the surgical review of every patient, both of which may be important. We are currently performing a study to see whether prior CT scanning also improves diagnostic accuracy of subsequent fibreoptic bronchoscopy.
We think it unlikely that the high surgical resection rate in patients with confirmed lung cancer is due to patient selection by referring respiratory physician since the age distribution of our patients is not significantly different from other studies and the proportion of patients confirmed as having malignant disease is also similar. However, some 50 patients were referred direct to the specialist respiratory oncologist at Addenbrooke’s having bypassed the outpatient investigation service at Papworth. We do not feel that this situation alters the significance of our results as, even if all these patients had NSCLC, the overall surgical resection rate would still be more than 20%.
Our failed thoracotomy rate of 11% is similar to that reported previously from other centres with similar surgical resection rates15 ,16 and occurred despite CT scanning in all patients. It has been suggested that the use of video-assisted thoracoscopy (VATS) may reduce the incidence of failed thoracotomy.15 We are currently looking to see whether increasing the frequency of VATS in selected patients does lead to a fall in the number of patients who undergo unsuccessful resection.
It will obviously also be important to follow our cohort of patients to see whether the increased surgical resection rate is associated with improved long term morbidity/mortality.
In conclusion, this study has shown that it is possible to match the surgical resection rates found in Europe and the USA by investigating patients according to a set protocol which includes universal CT staging and surgical review. This service was made possible by a reorganisation of services which entailed centralising the investigation of patients with lung cancer from several health districts in a cardiothoracic centre with immediate access to specialist thoracic radiology, pathology, and surgery. Other potential benefits of such a service include centralisation of other services such as palliative care, audit and data collection, targeting of research, and increased entry of patients into clinical trials.
Footnotes
Sources of funding: nil.
Conflict of interest: none.