Article Text

Abstract
Background: Early exposure to parental smoking appears to influence the development of the airways and predispose to respiratory symptoms. A study was undertaken to determine whether the consequences of parental smoking could be traced in adulthood.
Methods: Information from interviewer-led questionnaires was available for 18 922 subjects aged 20–44 years from random population samples in 37 areas participating in the European Community Respiratory Health Survey. Lung function data were available for 15 901 subjects.
Results: In men, father’s smoking in childhood was associated with more respiratory symptoms (ORwheeze 1.13 (95% CI 1.00 to 1.28); never smokers: ORwheeze 1.21 (95% CI 0.96 to 1.50)) and there was a dose-dependent association between number of parents smoking and wheeze (one: OR 1.08 (95% CI 0.94 to 1.24); both: OR 1.24 (95% CI 1.05 to 1.47); ptrend = 0.010). A reduced ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) was related to father’s smoking (−0.3% (95% CI −0.6 to 0)) and number of parents smoking (ptrend <0.001) among men. In women, mother’s smoking was associated with more respiratory symptoms and poorer lung function (ORwheeze 1.15 (95% CI 1.01 to 1.31), never smokers: ORwheeze 1.21 (95% CI 0.98–1.51); FEV1 −24 ml (95% CI −45 to −3); FEV1/FVC ratio −0.6% (95% CI −0.9 to −0.3)). These effects were possibly accounted for by maternal smoking in pregnancy (ORwheeze 1.39 (95% CI 1.17 to 1.65); FEV1 −23 ml (95% CI −52 to 7); FEV1/FVC ratio −0.9% (95% CI −1.3 to −0.4)) as there was no association with paternal smoking among women (interaction by sex, p<0.05). These results were homogeneous across centres.
Conclusion: Both intrauterine and environmental exposure to parental tobacco smoking was related to more respiratory symptoms and poorer lung function in adulthood in this multicultural study. The age window of particular vulnerability appeared to differ by sex, postnatal exposure being important only in men and a role for prenatal exposure being more evident in women.
- environmental tobacco smoke
- smoking
- parental smoking
- maternal smoking in pregnancy
- obstructive lung disease
- BHR, bronchial responsiveness
- ECRHS, European Community Respiratory Health Survey
- ETS, environmental tobacco smoke
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
Statistics from Altmetric.com
- environmental tobacco smoke
- smoking
- parental smoking
- maternal smoking in pregnancy
- obstructive lung disease
- BHR, bronchial responsiveness
- ECRHS, European Community Respiratory Health Survey
- ETS, environmental tobacco smoke
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
An increased risk for wheeze and asthma in children whose parents smoke is fairly well documented.1–4 Several studies have shown that intrauterine exposure to products from tobacco smoking in pregnancy reduces infant lung function.5–9 An independent effect of postnatal exposure to environmental tobacco smoke is suggested by an increased risk of asthma in children with fathers who smoke.1 Even if some studies of children indicate that the harmful effects of parental smoking decrease when the children grow older,4 there is some evidence of permanent damage to the airways with reduced lung function10,11 and an increased risk for asthma12,13 or wheezing illness14 in adults exposed to parental smoking in childhood. Information on the long term consequences of parental smoking for adult respiratory health is, however, relatively scarce and we address this issue in the European Community Respiratory Health Survey (ECRHS).
There is some evidence that the airways of men and women respond differently to exposure to tobacco smoke products.3–6,8,11,15,16 This is plausible as there are differences between the male and female airways from early in fetal lung development and throughout life.17,18 Female lungs mature earlier with regard to surfactant production. Throughout life women have smaller lungs than men, but their lung architecture is more advantageous with a greater airway diameter in relation to the volume of the lung parenchyma. After puberty the relative advantage of the female airways is lost, possibly as a result of hormonal changes in women and increased muscular strength among men which enhances lung function. Thus, in childhood airway hyperresponsiveness and asthma is more common among boys than girls, while this is reversed after puberty.17,19 It seems likely that the age windows for vulnerability to tobacco smoke products and to manifestation of symptoms could differ between the sexes. However, most studies do not give separate data for men and women. In this study we address possible sex differences in the effects of parental smoking on adult respiratory health. The ECRHS is large enough for analyses of interactions, and the international setting of the study to some extent allows for separation of heterogeneous effects of sociocultural sex differences and homogeneous effects related to biological sex differences.
METHODS
Data collection
The methodology for the ECRHS has been fully described elsewhere.20,21 Briefly, participating centres selected an area defined by pre-existing administrative boundaries with a population of at least 150 000. At least 1500 men and 1500 women aged 20–44 years were randomly selected from each centre. In stage I subjects were sent the ECRHS screening questionnaire, a self-completed questionnaire about adult respiratory health. In stage II a smaller random sample of subjects who had completed the screening questionnaire was invited to attend for a more detailed interviewer-led questionnaire, lung function testing, and blood tests. The informed consent of all participants was obtained and the study was approved by all the involved ethics committees. This analysis includes data for 18 922 subjects from 37 centres representing 17 countries.
Specific IgE to house dust mite, cat, timothy grass and Cladosporium was measured in serum samples provided by 13 972 (74%) of the subjects. The test for specific IgE was considered to be positive if >0.35 kU/l. Details of the IgE measurements are described elsewhere.22 “Atopy” was defined as having specific IgE to cat, grass, house dust mite, and/or mould.
Forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) were recorded by a standard spirometric method.23 Spirometric data were available for 15 901 (84%) subjects. The ratio between FEV1 and FVC was calculated and used as a continuous variable unless otherwise explicitly stated. Metacholine challenge was performed with a dosimeter (Mefar, Brescia, Italy), providing information for 13 206 (70%) subjects. The degree of bronchial responsiveness (BHR) was expressed as the ECRHS slope.24 Height was measured before measurement of lung function.
Information on parental smoking habits was collected using an interviewer-led questionnaire (table 1). Nearly all subjects gave information about maternal and paternal smoking, while a substantial number answered “don’t know” to the question about maternal smoking in pregnancy. A variable describing whether one or both parents had smoked was created in order to provide a crude graded measure of exposure.
Parental smoking as reported by men and women aged 20–45 years
“Asthma” was defined as using current asthma medication or reporting asthma attacks during the previous 12 months. “Three or more asthma symptoms” was defined as answering “yes” to three or more questions about asthma symptoms during the previous 12 months (wheeze, wheeze with shortness of breath, wheeze without having a cold, waking with tightness in chest, waking with shortness of breath, night cough, asthma attacks, asthma medication). “Chronic bronchitis” was defined as having both regular cough and regular phlegm.
Statistical analysis
Logistic regression models were used to assess the independent effects of parental smoking in childhood on adult respiratory symptoms, and adjustments were made for number of siblings, sex, age, body mass index, current passive smoking, current smoking (never, ex, and current smoking), current occupation (European Economic Community Status Groups-14),25 and study centre. Linear regression models were used to analyse the effects of parental smoking on lung function, adjusting for the same confounders and for the interaction terms of sex with age, height, weight, and weight squared in analyses of all subjects, for age, height, weight and weight squared in sex-specific analyses. Potential heterogeneity between centres in the effect of each exposure variable on wheeze was studied by meta-analyses according to DerSimonian and Laird.26 All analyses were carried out using the statistical software program Stata 7.0 (Stata Corporation, Texas, USA).
Differences according to sex, adult smoking status, and atopy were investigated. As all these aspects were important but sub-stratification by three variables is not feasible, the following strategy was chosen: Data for all subjects are presented to allow comparison with studies that do not stratify by sex; data for men and women are presented separately due to differences between the sexes in airways development. Non-atopic and atopic subjects differed with regard to associations with maternal smoking and these data are presented for men and women together as the associations with maternal smoking did not differ significantly by sex. Data for never smokers are presented in case of residual confounding by smoking.
RESULTS
In all, 67% of subjects reported that their father had smoked during their childhood. There were relatively small differences in this proportion between countries (table 2). Maternal smoking varied widely, from 3% to 17% in the centres in Spain, Estonia, France and Italy to over 40% in Denmark, Iceland and the English speaking centres. Similarly, maternal smoking in pregnancy varied greatly, from 1% in Spain to 27% in Ireland (table 2).
Prevalence of parental smoking by country in study subjects born 1945–72
Considering men and women together (table 3), paternal smoking was not significantly associated with adult respiratory symptoms or lung function. Maternal smoking was associated with an increased risk for respiratory symptoms and with reduced FEV1 and FEV1/FVC ratio. The associations of maternal smoking with wheeze (fig 1) and with FEV1/FVC ratio <75% were consistent between centres (pheterogeneity = 0.4 and pheterogeneity = 0.3, respectively). Among subjects who gave information about maternal smoking in pregnancy, this exposure was strongly associated with respiratory symptoms and with reduced FEV1/FVC ratio (table 3) which was consistent between centres (wheeze: pheterogeneity = 0.2). The association of parental smoking and measures of adult respiratory health increased in strength with number of smoking parents, a dose-response relationship that was significant for several symptoms, FEV1 and FEV1/FVC ratio (table 3). Adult asthma or BHR was not associated with any measure of parental smoking.
Association of adult respiratory symptoms and lung function with parental smoking in childhood
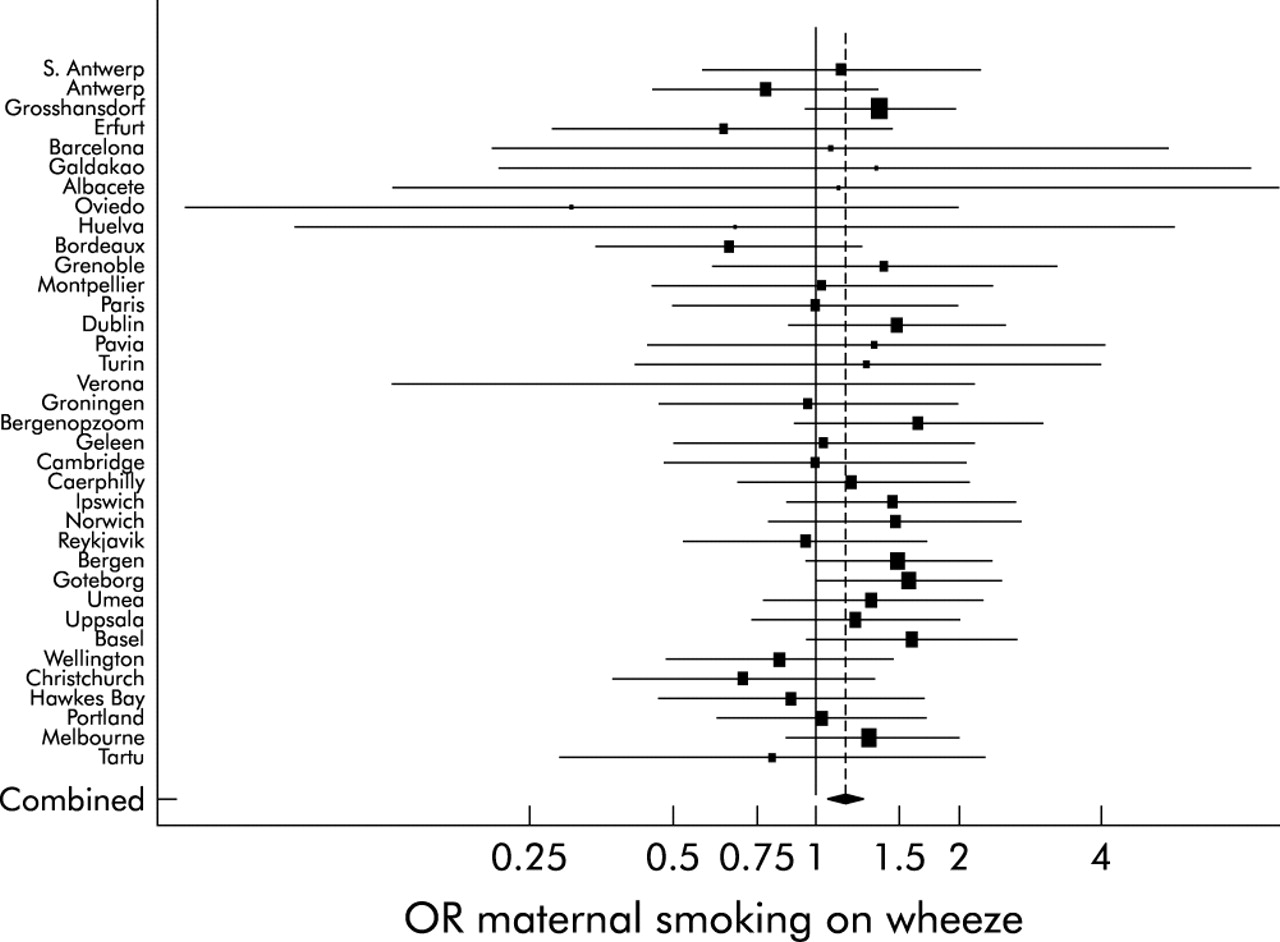
Odds ratios for the association of maternal smoking and adult wheeze by centre. Adjustment within centre for paternal smoking, adult passive smoking, adult smoking, number of siblings, sex, age, and occupation. For each centre horizontal lines indicate 95% CI. For combined odds ratio the diamond indicates 95% CI from model with centre as random effect. The size of each square is proportional to the sample size.
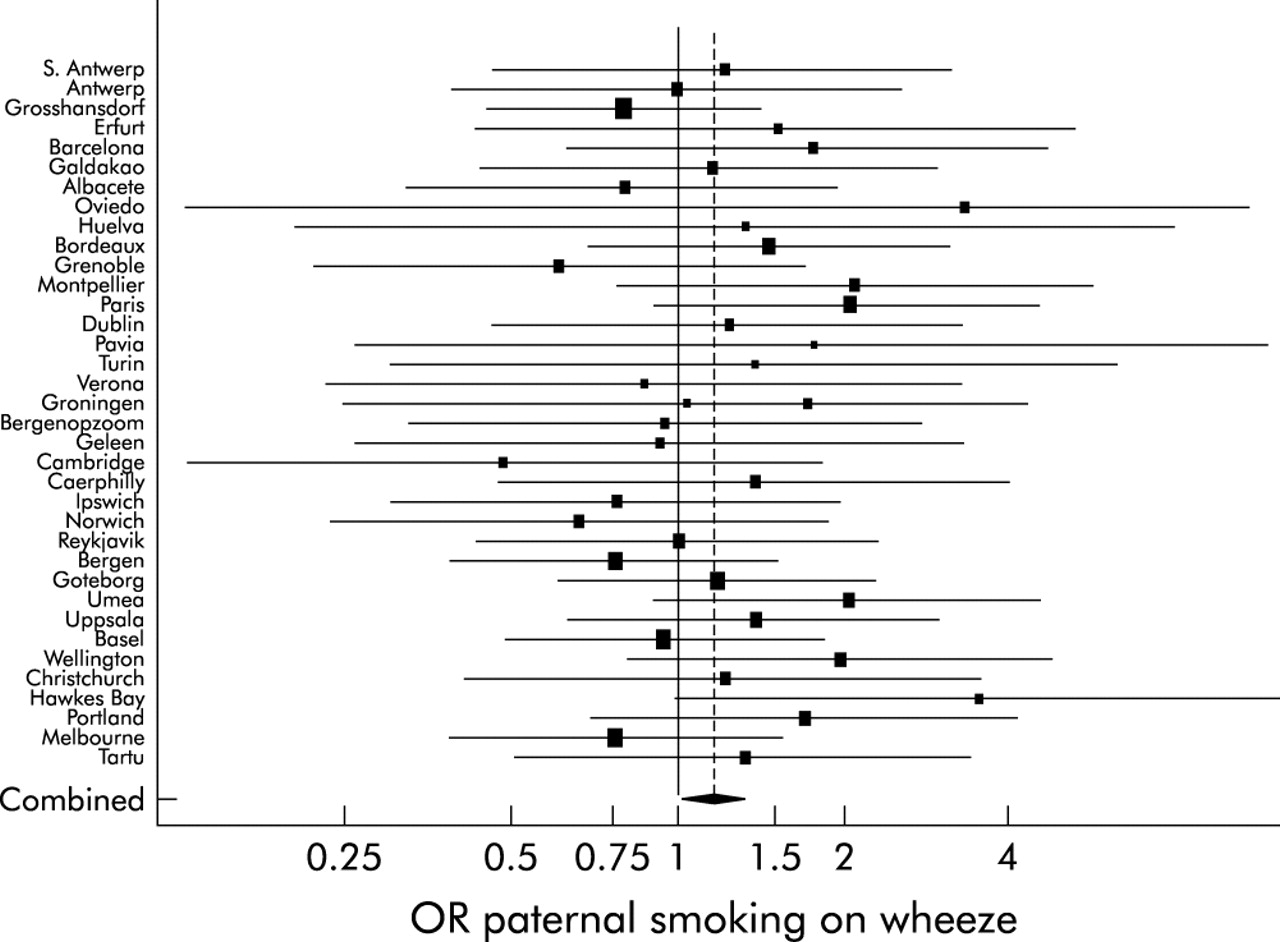
An association of adult respiratory symptoms and father’s smoking was identified in men (table 4, fig 2) but not in women (table 5). This difference between the sexes was significant (wheeze: pinteraction = 0.033; wheeze without cold: pinteraction = 0.011) and consistent between centres (pheterogeneity = 0.2 for the interaction effect of sex with paternal smoking on wheeze). Father’s smoking was further associated with decreased lung function in men but not in women; interaction by sex was not statistically significant (FEV1: pinteraction = 0.1; FEV1/FVC ratio: pinteraction = 0.4). The risk for respiratory symptoms and poor lung function increased with an increasing number of parents smoking only in men (table 4). These differences in the sexes were also significant (wheeze: pinteraction = 0.024 (excluding maternal smoking in pregnancy); FEV1: pinteraction = 0.035). Mother’s smoking was associated with increased risk for respiratory symptoms and reduced lung function in women (table 5); the effects were particularly strong for maternal smoking during pregnancy. Most associations with maternal smoking in men did not reach statistical significance, although the estimates were only slightly smaller than in women.
Association of adult respiratory symptoms and lung function with parental smoking in childhood in 7678 men
Association of adult respiratory symptoms and lung function with parental smoking in childhood in 7799 women

Odds ratios for the association of paternal smoking and adult wheeze among men by centre. Adjustment within centre for maternal smoking, adult passive smoking, adult smoking, number of siblings, age, and occupation. For each centre, horizontal lines indicate 95% CI. For combined odds ratio, diamond indicates 95% CI from model with centre as random effect. The size of each square is proportional to the sample size.
When only never smokers were considered, the key findings were similar to those of the total population although many estimates did not reach statistical significance (table 6). In men, paternal smoking was associated with an increased risk for symptoms and an indicated decrease in the FEV1/FVC ratio. In women, maternal smoking was associated with more symptoms and poorer lung function. These findings did not show a significant interaction with adult smoking status. The differences between the sexes in the associations of paternal smoking with symptoms and maternal smoking with symptoms and lung function were significant or of borderline significance (table 6). The full table of sex-specific effects of parental smoking stratified by current adult smoking status is available online at www.thoraxjnl.com/supplemental.
Association of adult respiratory symptoms and lung function with maternal smoking in childhood in never smoking men (n = 3043) and women (n = 3582)
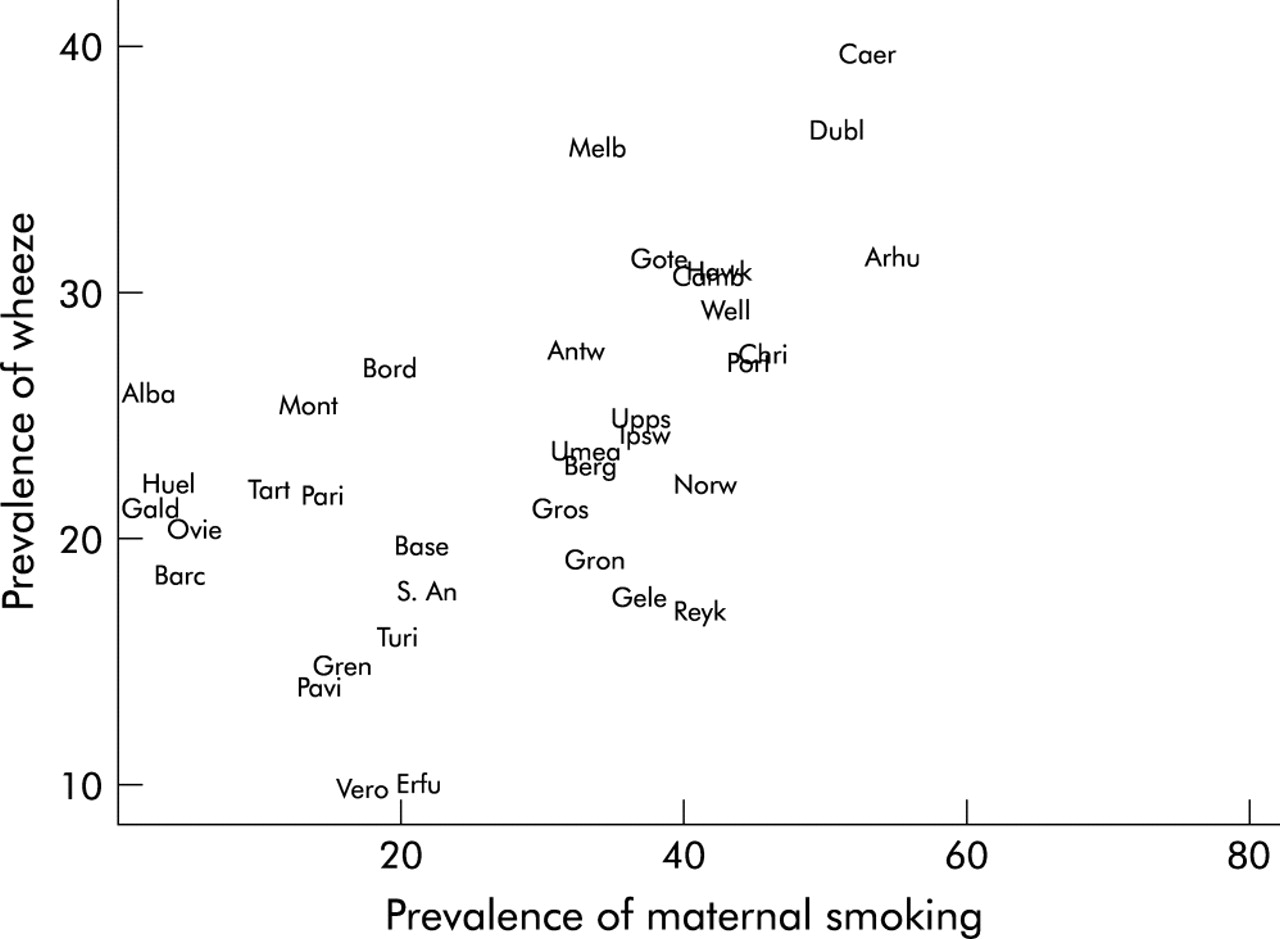
The effects of maternal smoking on respiratory symptoms differed with regard to atopic status, with a stronger effect of maternal smoking on some symptoms among non-atopic subjects (table 7; wheeze: pinteraction = 0.024). A corresponding difference by atopy was not found for lung function. Interactions by atopy in the associations of paternal smoking with respiratory symptoms or lung function were smaller and not significant. Atopy was a negative confounder for the associations between parental smoking and respiratory symptoms. Adjustment increased the strength of the associations but was not included in the final results because of the interaction effects noted above. Centre prevalence of wheeze was strongly correlated with centre prevalence of maternal smoking (r = 0.57, fig 3). The English speaking centres had a particularly high prevalence of wheeze and of maternal smoking. In the Latin countries, maternal smoking in pregnancy was uncommon and the prevalence of wheeze was relatively low in most centres.
Association of adult asthma and lung function and maternal smoking in childhood according to atopic status (atopy defined as specific IgE to cat, grass, house dust mite and/or mould) (including 13791 subjects with information from blood tests as well as other variables)

{kind=link}
{kind=link}
{kind=link}
Prevalence of wheeze in subjects aged 20–44 years and prevalence of maternal smoking in 37 study centres in 17 countries.
DISCUSSION
Subjects whose parents had smoked experienced more respiratory symptoms and poorer lung function in adulthood consistently across 37 centres in the western world. Thus, parental tobacco smoking appears to influence the development of the child’s airways with permanent consequences in terms of poorer adult respiratory health. Our analysis indicated that both intrauterine exposure to maternal smoking during pregnancy and postnatal exposure to ETS was of importance. In men, exposure to father’s smoking in childhood was related to more respiratory symptoms and more airways obstruction in adulthood, and there was a dose-response relationship between the number of parents smoking and respiratory symptoms and lung function. There was therefore a convincing effect of postnatal exposure to ETS on adult lung health among men. The possible influence of intrauterine exposure could not be separated from postnatal effects of maternal smoking. In women, no convincing effect of postnatal exposure to paternal smoking could be identified, so the consistent associations of mother’s smoking with respiratory symptoms and poorer lung function in adult women may be related to the prenatal exposure to products from maternal smoking during pregnancy. This study therefore indicates that the age window for particular vulnerability to parental smoking differs between men and women.
Recall bias is a potential problem in this study. However, parental smoking was significantly associated with reduced lung function also among non-wheezers. Nearly all participants (99% and 97%) reported whether their mother or father had smoked when they were children, even though they had been given an option of responding “don’t know” (an option used by 40% when asked about mother’s smoking in pregnancy). Symptomatic and non-symptomatic subjects might have recalled parental smoking differently but, for differential recall to explain our findings, non-atopic subjects rather than atopic subjects, and wheezers rather than diagnosed asthmatics, would have over-reported parental smoking. This seems unlikely. Thus, while we do not have information to validate the information on parental smoking, the role of differential recall bias seems to be limited. Information on whether the parents smoked or not, however, gives a very crude measure of exposure and, together with non-differential measurement error, this may be the reason why some main effects in subgroups did not reach statistical significance despite large sample sizes and near identical point estimates between subgroups. The small but consistent effects may therefore possibly reflect stronger underlying associations. The strengths of the study are the overall sample size that permit subgroup analyses and the broad range of populations studied in an international setting.
The main results were similar in never smokers to those in the total population sample, arguing against a role of residual confounding by current smoking habits and related lifestyle factors. The findings were also consistent between centres that, particularly during the post-war years, differed with regard to social, economic and cultural factors as illustrated by the wide variation in women’s smoking habits (table 2). This argues against a major role for confounding by smoking related lifestyle factors of the parents.
The quality of the information on maternal smoking in pregnancy is considered less reliable and is not an important basis for the conclusions of this paper. The 40% who reported that their mother had smoked when she was pregnant probably constitute a group with intrauterine exposure and, possibly, with heavier postnatal exposure. Those who answered “don’t know” may include a considerable number with intrauterine exposure as well. The lack of recall in this group could be suspected to be associated with better adult respiratory health, but more symptoms and poorer lung function were also observed in this group.
Our findings are in agreement with studies in children.1–4 Based on meta-analyses of a large number of relevant studies, Cook and Strachan concluded that father’s smoking—as well as mother’s smoking—was related to respiratory symptoms in children, with strong evidence for a causal relationship.1 The effect of paternal smoking, often not evident in smaller studies but convincing in their meta-analysis, argues for an independent effect of postnatal passive smoking. An in utero effect of maternal smoking during pregnancy has been indicated by several studies, most convincingly shown as changes in infant lung function.5–9 A few studies follow the effects of parental smoking into adult life. Upton et al10 observed a significant effect of maternal (but not paternal) smoking on lung function in 2295 adults, including a dose-response relationship with the daily number of cigarettes smoked. Masi et al11 showed an effect of childhood ETS on lung function in young men, while Strachan et al14 reported an effect of maternal smoking in pregnancy on wheezing illness before age 7 and at ages 17–33 years in the 1958 British cohort. Hu et al13 found an increased asthma risk in young adults related to paternal as well as maternal smoking, and a dose-response relationship with the number of parents smoking. Larsson et al12 showed significant effects of childhood passive smoking on asthma among 3556 never smoking adults in Sweden, while Jenkins et al27 found no significant associations of self-reported asthma or wheeze with paternal or maternal smoking in a study of 1494 young adults.
In our study the vulnerability towards prenatal and postnatal exposure to tobacco smoke appeared to differ between men and women. In agreement with our findings in adults, several studies indicate a stronger effect of intrauterine exposure on female than on male newborns.4,5,8 It has been suggested that nicotine induces “masculinisation” of the airways with narrower airways, reduced airway compliance, and reduced elastic recoil.8 This view is supported by animal studies showing structural changes in the fetal lungs including loss of elastic recoil, lung hypoplasia, and atelectasis related to in utero exposure to tobacco smoke products.28–30
The stronger association between childhood ETS and obstructive lung disease in men, as shown in this study and by Hu et al,13 could be related to boys having less mature lungs and relatively narrower airways during childhood. These factors are believed to contribute to the generally higher rates of pulmonary morbidity in boys than in girls, and could possibly also explain a higher susceptibility for permanent damage by exposure to ETS during this age window. It has been suggested that the association of paternal smoking and asthma among males could be explained by boys spending more time with their fathers than girls. However, in the multicultural setting of this study this association was homogeneous across centres (fig 2), so a biological explanation seems more plausible than a behavioural explanation that would tend to differ between cultures.
Parental smoking was associated with respiratory symptoms, reduced FEV1, and increased airways obstruction, but not with diagnosed asthma and increased bronchial hyperresponsiveness. Exposure to tobacco smoke early in life may influence the development of airways structure (reflected in FEV1 and FEV1/FVC ratio) more than susceptibility to mucosal inflammation decades later (contributing relatively more to BHR), and this may contribute to a clinical picture slightly different from classical asthma.
Parental smoking was strongly associated with respiratory symptoms among non-atopic subjects. This suggests that parental smoking is an important causal factor for non-atopic asthma, a condition that deserves far more focus among researchers. Born in 1945–72, our study subjects are the offspring of the post-war generation of parents. Smoking among men was common all over the western world during the post-war years. The young women in the English speaking and the Northern European countries often took up the habit of smoking during this period, while smoking was still uncommon among women in the Latin countries. Differences in post-war smoking habits of women could partly explain the high prevalence of wheezy illness observed in the English speaking countries.
In conclusion, both mother’s and father’s smoking appears to cause permanent damage to the developing airways of the child, leading to more respiratory symptoms and impaired lung function in adult life. Exposure to ETS in childhood was related to more respiratory symptoms in men but not in women, while maternal smoking in pregnancy increased the risk for obstructive lung disease in women and, possibly, also in men. We speculate that tobacco smoke products lead to structural changes in the developing lungs in females, particularly during fetal life, and in males to a larger extent postnatally. Other factors such as sex specific growth of the airways and hormonal factors may contribute to determine at what age and to what extent this susceptibility is manifested as respiratory symptoms. In young adults we found an increased risk for obstructive lung disease in both men and women whose parents had smoked, although this appeared to be related to exposure at different age windows during lung development.
Acknowledgments
The coordination of this work was supported by the European Commission and we are grateful to the late Colette Baya and Dr Manuel Hallen for their help during the study and to Professor K Vuylsteek and the members of the COMAC for their support. The following grants helped to fund the local studies: Australia: Allen and Hanbury’s, Australia; Belgium: Belgian Science Policy Office, National Fund for Scientific Research; France: Ministère de la Santé, Glaxo France, Institut Pneumologique d’Aquitaine, Contrat de Plan Etat-Région Languedoc-Rousillon, CNMATS, CNMRT (90MR/10, 91AF/6), Ministre delegué de la santé, RNSP; Germany: GSF, and the Bundesminister für Forschung und Technologie, Bonn; Greece: The Greek Secretary General of Research and Technology, Fisons, Astra and Boehringer-Ingelheim; India: Bombay Hospital Trust; Italy: Ministero dell’Università e della Ricerca Scientifica e Tecnologica, CNR, Regione Veneto grant RSF n. 381/05.93; New Zealand: Asthma Foundation of New Zealand, Lotteries Grant Board, health Research Council of New Zealand; Norway: Norwegian Research Council project no 101422/310; Portugal: Glaxo Farmacêutica Lda, Sandoz Portugesa; Spain: Ministero Sanidad y Consumo FIS grants #91/0016060/00E–05E and #93/0393, and grants from Hospital General de Albacete, Hospital General Juan Ramón Jiménenz, Consejeria de Sanidad Principado de Asturias; Sweden: The Swedish Medical Research Council, the Swedish Heart Lung Foundation, the Swedish Association against Asthma and Allergy; Switzerland: Swiss National Science Foundation grant 4026–28099; United Kingdom: National Asthma Campaign, British Lung Foundation, Department of Health, South Thames Regional Health Authority; USA: United States Department of Health, Education and Welfare Public Health Service Grant #2 S07 RR05521–28.
REFERENCES
Supplementary materials
Web-only Table
The table is available as a downloadable PDF (printer friendly file). If you do not have Adobe Reader installed on your computer, you can download this free-of-charge, please Click Here
Files in this Data Supplement:
- [View PDF] - Table Association of adult asthma and lung function with maternal smoking in childhood in men and women according to smoking status
Footnotes
-
Coordinating Centre (London): P Burney, S Chinn, C Luczynska, D Jarvis, E Lai.
-
Project Management Group: P Burney (Project leader), S Chinn, C Luczynska, D Jarvis, P Vermeire (Antwerp), H Kesteloot (Leuven), J Bousquet (Montpellier), D Nowak (Hamburg), the late J Prichard (Dublin), R de Marco (Verona), B Rijcken (Groningen), J M Anto (Barcelona), J Alves (Oporto), G Boman (Uppsala), N Nielsen (Copenhagen), P Paoletti (Pisa).
-
Participating Centres: Austria: W Popp (Vienna); Australia: M Abramson, J Raven, J Rolland (Melbourne); Belgium: P Vermeire, F van Bastelaer (Antwerp South, Antwerp Central); Denmark: M Iversen (Aarhus); Estonia: R Jögi (Tartu); France: J Bousquet J Knani (Montpellier) F Neukirch, R Liard (Paris), I Pin, C Pison (Grenoble), A Taytard (Bordeaux); Germany: H Magnussen, D Nowak (Hamburg), H E Wichmann, J Heinrich (Erfurt); Greece: N Papageorgiou, P Avarlis, M Gaga, C Marossis (Athens); Iceland: T Gislason, D Gislason (Reykjavik); Ireland: J Prichard, S Allwright, D MacLeod (Dublin); Italy: M Bugiani, C Bucca, C Romano (Turin), R de Marco Lo Cascio, C Campello (Verona), A Marinoni, I Cerveri, L Casali (Pavia); Netherlands: B Rijcken, A Kremer (Groningen, Bergen-op-Zoom, Geleen); New Zealand: J Crane, S Lewis (Wellington, Christchurch, Hawkes Bay); Norway: A Gulsvik, E Omenaas (Bergen); Portugal: J A Marques, J Alves (Oporto); Spain: J M Antó, J Sunyer, F Burgos, J Castellsagué, J Roca, J B Soriano, A Tobías (Barcelona), N Muniozguren, J Ramos González, A Capelastegui (Galdakao), J Castillo, J Rodriguez Portal (Seville), J Martinez-Moratalla, E Almar (Albacete), J Maldonado Pérez, A Pereira, J Sánchez (Huelva), J Quiros, I Huerta, F Pavo (Oviedo); Sweden: G Boman, C Janson, E Björnsson (Uppsala), L Rosenhall, E Norrman, B Lundbäck (Umeå), N Lindholm, P Plaschke (Göteborg); Switzerland: U Ackermann-Liebrich, N Künzli, A Perruchoud (Basel); United Kingdom: M Burr, J Layzell (Caerphilly), R Hall (Ipswich), B Harrison (Norwich), J Stark (Cambridge); USA: S Buist, W Vollmer, M Osborne (Portland).
Linked Articles
- airwaves