Article Text

Abstract
Background: The 72 kDa matrix metalloproteinase 2 (MMP-2) and the 92 kDa matrix metalloproteinase 9 (MMP-9) are type IV collagenases implicated in various aspects of inflammation including accumulation of inflammatory cells, tissue injury, and development of remodelling. The role of these enzymes in the pathogenesis of asthma exacerbations is unknown.
Methods: Circulating levels of MMP-2 and MMP-9 proteins and the expression of their inhibitor, tissue inhibitor of metalloproteinase 1 (TIMP-1), were measured in 21 patients experiencing an asthma exacerbation and 21 age matched patients with stable asthma. Circulating gelatinolytic activity was compared during the asthma exacerbation and during subsequent convalescence by gelatin zymography in the same individuals. In addition, MMP-9 specific activity was quantified with a colorimetric assay which uses an artificial proenzyme containing a specific domain recognised by MMP-9 in the same paired samples.
Results: A significant increase in the circulating level of MMP-9 was seen in patients with an asthma exacerbation compared with patients with stable asthma (202.9 (22.0) v 107.7 (9.9) ng/ml, p=0.0003). There were no significant differences in the circulating levels of MMP-2 or TIMP-1. Gelatin zymography identified two major circulating gelatinolytic activities corresponding to MMP-2 and MMP-9, and showed that asthma exacerbations are characterised by markedly increased MMP-9 activity with no significant change in MMP-2 activity compared with the activities during convalescence in the same individuals. Direct measurement showed that MMP-9 specific activity is significantly increased during asthma exacerbations compared with subsequent convalescence (269.6 (31.7) v 170.4 (12.6) ng/ml, p=0.0099).
Conclusions: Asthma exacerbations are characterised by increased circulating MMP-9 activity. This increased activity may be related to exaggerated airway inflammation and airway remodelling.
- asthma
- matrix metalloproteinases
- asthma exacerbation
Statistics from Altmetric.com
It is generally accepted that chronic inflammation leads to airway remodelling in patients with asthma1 and that this may contribute to irreversible airflow obstruction in affected individuals.2 The role of inflammation in the pathophysiology of asthma is related to the fact that the intensity of inflammation is associated with the degree of airway remodelling,2 as well as with the severity of disease.3 The inflammatory processes underlying asthma involve a complex interaction of cell communications that result in increases in airway wall thickness. These alterations include an increase in vascularity, the development of oedema, smooth muscle hypertrophy and hyperplasia, and hyperplasia of mucus glands.4 Increases in the thickness of the basement membrane and subepithelial fibrosis4,5 also occur and are currently recognised as the hallmarks of remodelled asthmatic airways.6 These changes are believed to be related to the severity of the disease.7 Several lines of evidence suggest that these changes are part of the repair process designed to restore tissue integrity in response to inflammatory insults.7
The acute inflammation that occurs in asthma is most commonly recognised clinically as a sudden symptomatic deterioration due to bronchoconstriction and increased airway hyperresponsiveness. However, the underlying pathophysiology is still unknown. It is important to determine the role of exacerbations on the long term complications of asthma such as the development of airway remodelling. Recent investigations have suggested that repeated antigen challenges, which provoke episodes of acute inflammation, promote airway remodelling in a murine model of asthma8 by altering the homeostasis of extracellular matrix (ECM) components such as collagen. In this context, it is essential for the understanding of the pathophysiology of asthma exacerbations to characterise the factors involved in inflammation and tissue remodelling.
Zinc matrix metalloproteinases (MMPs) are members of a family of enzymes that cleave ECM proteins. MMPs digest collagen, gelatin (denatured collagen), and other components of the ECM that have profound effects on the development, migration, and metabolic function of cells. Furthermore, MMPs have been implicated in many inflammatory conditions. Specifically, MMP-9 has been shown to mediate vascular leakage9 and induce the migration of inflammatory cells into sites of inflammation.10 Both of these functions are prominent components of asthma exacerbations, so we hypothesised that circulating MMPs might have a crucial role in exacerbations of asthma. A study was therefore undertaken to characterise changes in MMP activity during asthma exacerbations.
METHODS
Subjects
The subjects were recruited consecutively from regular attenders at the outpatient clinic of Kurume University Hospital in the year from April 1999 to March 2000 after obtaining informed consent. The diagnosis and classification of the severity of asthma were based on GINA guidelines.11 The severity was classified as step 1 (intermittent), step 2 (mild persistent), and step 3 (moderate persistent). Patients who required regular systemic corticosteroid therapy were excluded from the study. Atopy was defined by a raised serum total and specific IgE to common environmental allergens including house dust mite, cat, dog, cockroach, grasses and trees.11 None of the patients had a history of smoking. Twenty one patients were recruited during a moderate to severe exacerbation,11 either on their scheduled visit to the clinic or during an emergency visit.
The patients underwent complete clinical examination and chest radiography, if required, to exclude the presence of concomitant acute illnesses such as pneumonia. The minimum criteria for the diagnosis of an asthma exacerbation included intense subjective breathlessness, audible wheezing on auscultation, and a morning peak expiratory flow (PEF) <70% of the personal best value in the previous 3 months.11 Patients were monitored to the subsequent convalescence which was defined by the continuous resolution of subjective symptoms and physical findings for at least 2 weeks, with a morning PEF or forced expiratory volume in 1 second (FEV1) >80% of the personal best value.
Twenty one age matched patients with stable asthma were recruited on their scheduled visit if the symptoms and PEF were stable with no change in treatment for at least 1 month. Table 1 summarises the clinical characteristics and morning PEF (expressed as a percentage of the personal best value) of the patients on recruitment to the study. Serum samples were collected on the visits, aliquoted, and stored at −80°C until the time of assay.
Clinical characteristics of patients with asthma
Determination of MMP-2, MMP-9, and TIMP-1 protein concentrations
The concentrations of MMP-2, MMP-9, and TIMP-1 were determined using commercially available ELISA based (for MMP-2 and MMP-9) and EIA based (for TIMP-1) assay systems (all from Fuji Chemical Industries, Takaoka, Japan). Assays were performed using the protocols recommended by the manufacturer. The sensitivities of each assay were 0.37 ng/ml for MMP-2, 1 ng/ml for MMP-9, and 1.25 ng/ml for TIMP-1. The assay for MMP-2 does not crossreact with MMP-1, -3, -7, -8, -9, or MT1-MMP. The assay for MMP-9 detects proMMP-9 and proMMP-9-TIMP-1 complexes and does not crossreact with proMMP-1, proMMP-2, or proMMP-3. The assay for TIMP-1 does not crossreact with TIMP-2.
Gelatin zymography
Gelatin zymography was performed on paired serum samples obtained during exacerbations and subsequent convalescence to characterise the changes in circulating gelatinolytic activity. Each serum sample was diluted 1:20 in non-reducing sample buffer containing sodium dodecyl sulfate (SDS), glycerol, and bromophenol blue and subjected to electrophoresis on 8% (w/v) polyacrylamide SDS gels containing 1 mg/ml porcine skin gelatin (Sigma, St Louis, MO, USA). Protein standards (New England Biolabs, Beverly, MA, USA) were run on the same gel to estimate the molecular weight of the lytic bands. After electrophoresis the gels were washed in 2.5% Triton X-100 for 30 minute, rinsed briefly, and incubated at 37°C for 24 hours in a buffer containing 50 mM Tris HCl (pH 8.0) and 10 mM CaCl2. Following incubation the gels were stained with Coomassie blue R-250 and destained in a solution of 5% acetic acid and 10% methanol. Gelatinolytic activity appeared as unstained zones against a blue background.
Measurement of MMP-9 specific activity
The MMP-9 specific activity was quantified on the paired samples mentioned above using a colorimetric assay with a modified detection proenzyme which is activated by active MMP-9 (Amersham Pharmacia Biotech, Piscataway, NJ, USA).12 The proenzyme is activated by the cleavage of an amino acid sequence recognised specifically by active MMP-9 and, in turn, digests a chromogenic peptide substrate. The system detects a minimum of 0.125 ng/ml MMP-9 and does not crossreact with MMP-1, MMP-2, MMP-3, MMP-8, TIMP-1, or TIMP-2.
Statistical analysis
Statistical analysis was performed using StatView (Version 4.5, Abacus Concepts, Berkeley, CA, USA). The Mann-Whitney U non-parametric test was used to calculate p values for unpaired comparisons. Comparisons for values in the same individual were performed using the Wilcoxon test. A p value of <0.05 was considered statistically significant.
RESULTS
MMPs and TIMP-1
Patients with an asthma exacerbation had significantly higher circulating MMP-9 concentrations than patients with stable asthma. There was no significant difference in the circulating MMP-2 concentrations between the two groups, nor was there a significant difference in the circulating concentration of TIMP-1 which is an inhibitor of MMP-2 and MMP-9 (table 2). Coefficients of variation for MMP-2, MMP-9, and TIMP-1 were 0.196, 0.497, and 0.268 in the stable group, and 0.188, 0.420, and 0.216 in the exacerbation group, respectively.
Serum MMPs and TIMP-1 concentrations
Gelatin zymography
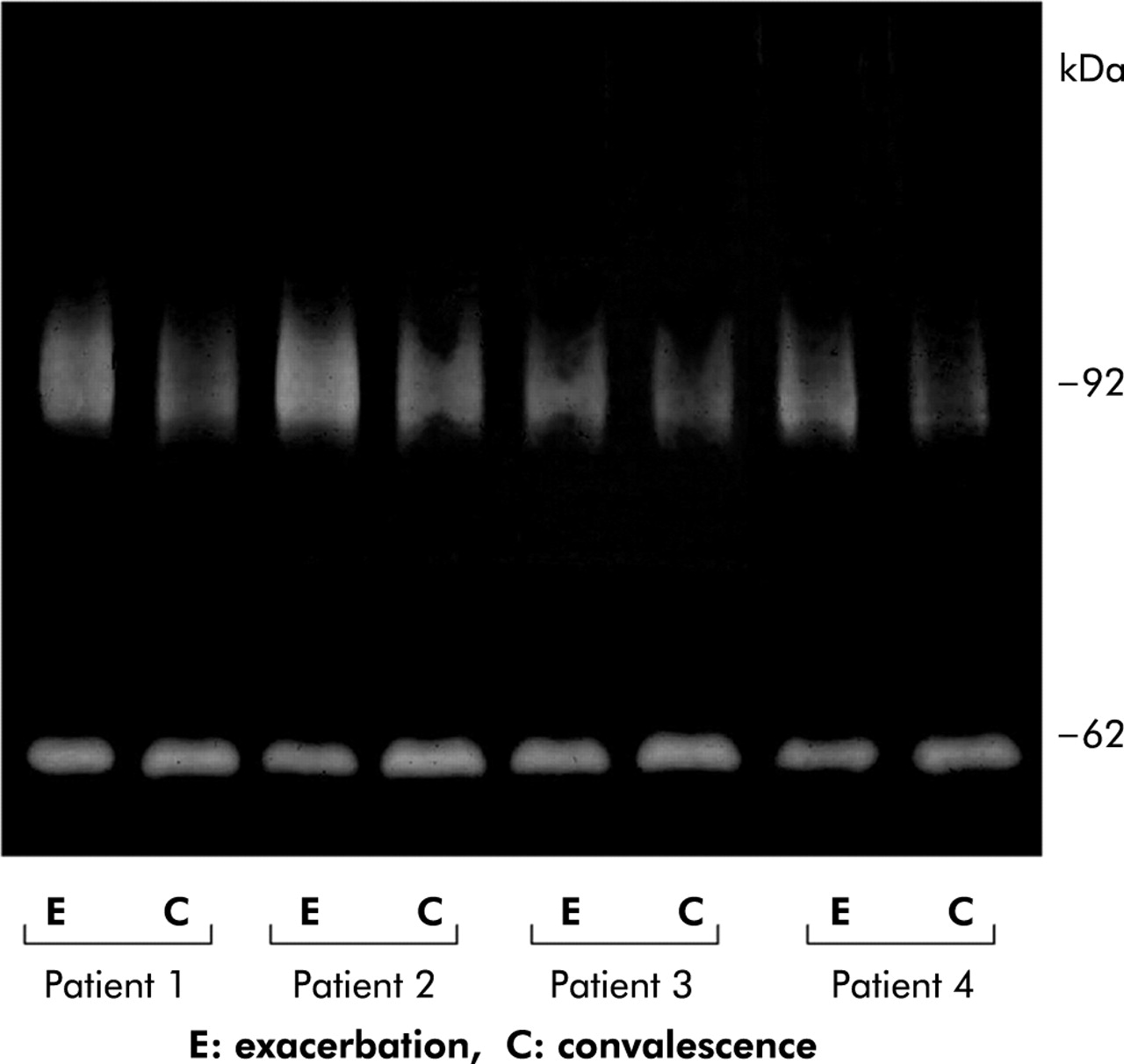
Twelve of the 21 patients with an asthma exacerbation fulfilled the definition of convalescence during the investigation period. A representative gelatin zymogram is shown in fig 1. Gelatin zymography revealed two major zones of gelatinolytic activity in the serum samples corresponding to MMP-2 and MMP-9 activity.13 The serum samples obtained during an asthma exacerbation had markedly higher MMP-9 activity than those obtained during convalescence in the same individuals. In contrast, the gelatinolytic activity corresponding to MMP-2 remained constant.

Representative gelatin zymogram showing circulating gelatinolytic activities and their changes during an asthma exacerbation and subsequent convalescence in four patients. Two major activities are visible, corresponding to MMP-9 and MMP-2. MMP-9 activity is higher during asthma exacerbations than during convalescence, whereas MMP-2 activity remains constant.
MMP-9 specific activity
Although gelatin zymography is a sensitive method for detecting MMP-2 and MMP-9 activity, it is difficult to quantify. Furthermore, it is not suitable for the evaluation of a large number of samples.14 A colorimetric assay specific for MMP-9 activity was therefore used to quantify changes in the circulating activity of the enzyme. Based on this assay, circulating MMP-9 levels during exacerbations were significantly higher than during the subsequent convalescence (269.6 (31.7) v 170.4 (12.6) ng/ml, p=0.0099; fig 2) in the same individuals.

{kind=link}
{kind=link}
Circulating MMP-9 activity during asthma exacerbations and subsequent convalescence. Specific MMP-9 activity was measured using a colorimetric assay system.
DISCUSSION
In this study we have measured changes in the expression and activity of the circulating metalloproteinases MMP-2 and MMP-9 and their inhibitor TIMP-1 during asthma exacerbations. The results showed that the circulating MMP-9 concentration is increased in patients with asthma exacerbations compared with patients with stable asthma. In contrast, there were no significant differences in the MMP-2 and TIMP-1 concentrations, suggesting that MMP-9 plays a role in the pathophysiology of asthma exacerbations. The coefficient of variation for MMP-9 was relatively high compared with those for MMP-2 and TIMP-1. This may represent a wide variability in serum MMP-9 levels in nature, at least in patients with asthma.15 We further characterised the changes in circulating MMP-9 activity in the same individuals using gelatin zymography and a specific colorimetric activity assay and confirmed increased MMP-9 activity during exacerbations compared with subsequent convalescence. These biochemical changes may have significant implications in the pathophysiology of asthma exacerbations.
Current evidence suggests that MMP-9 mediates several important pathways responsible for asthma exacerbations including airflow obstruction,16 increased vascular permeability,16 and exaggerated airway hyperresponsiveness.17 MMP-9 has also been implicated in the development of tissue fibrosis.18 In a study conducted by Hoshino et al19 inhaled corticosteroids reduced the amount of reticular basement membrane in association with decreased MMP-9 immunoreactivity in bronchial tissue, suggesting that enhanced MMP-9 activity promotes subepithelial fibrosis in asthmatic individuals. It is therefore likely that asthma exacerbations promote airway remodelling by altering MMP-9 mediated ECM homeostasis. Although many cell types can generate MMP-9, neutrophils are considered to be the major source of MMP-9 in the lower airways in status asthmaticus20 and in asthmatic individuals challenged with allergens.21 Circulating MMP-9 levels may therefore reflect a “spill over” of MMP-9 produced in the airways. As MMP-9 is a mediator of inflammation10,22 and tissue remodelling,18 an increase in its activity is likely to play a significant role in the pathophysiology of asthma exacerbations.
Inhaled or systemic corticosteroids are the mainstay of the current treatment for asthma, but they are not always effective in the treatment of asthma exacerbations.23 The most common trigger for an asthma exacerbation is known to be a respiratory tract infection,24 and the lower airway inflammation induced by experimental rhinovirus infection in asthmatic patients is not ameliorated by inhaled corticosteroids.25 Recent investigations have shown that MMP-9 activity in the lower airways is enhanced by allergen challenge,21,26 and that inhaled corticosteroids have no effect on this enhancement.26 Better treatments for asthma exacerbations need to be established for the optimal management of the disease. In this context, MMP-9 may be a potential target for the management of exacerbations of asthma.
Acknowledgments
This work is partially supported by a grant (to Dr Koga) from Clinical Research Foundation.
REFERENCES
Linked Articles
- Airwaves