Article Text

Abstract
Background: Recent studies of the role of bacteria in chronic bronchitis have shown that bacterial colonisation is associated with enhanced inflammation and that purulent acute exacerbations of chronic bronchitis (AECB) are associated with bacteria and characterised by increased inflammation. Changes in bronchial inflammation in response to the success or failure of bacterial eradication following AECB were therefore studied.
Methods: Bacterial quantitative culture and sputum markers of inflammation (myeloperoxidase (MPO), neutrophil elastase, leukotriene B4 (LTB4), sol:serum albumin ratio, and secretory leukoprotease inhibitor) were measured in patients presenting with culture positive purulent AECB and repeated 10 days and 2 months later. 41 patients provided sputum sufficient for both bacteriology and assessment of inflammation at baseline and day 10, and 46 provided sufficient sample for bacteriology, 40 of which could also be analysed for inflammation at 2 months (when clinically stable).
Results: At day 10, 17 of the 41 patient samples had a positive bacterial culture. In the stable state, 18 of the 46 samples had a positive culture, but with a significantly lower bacterial load than at presentation. Although there was no difference between the groups at presentation, the concentration of MPO was lower (p<0.05) in those in whom bacteria were eradicated by day 10 than in those with persisting bacteria. The LTB4 concentration was similarly lower (p<0.001) in those in whom bacteria were eradicated than in those with persistent bacteria. In the stable clinical state the concentrations of both MPO and LTB4 were lower in those in whom bacteria were eradicated than in patients with persisting bacteria.
Conclusion: Resolution of bronchial inflammation following AECB is related to bacterial eradication. Those in whom bacteria continue to be cultured in their sputum have partial resolution of inflammation which may reflect continued stimulation by the reduced bacterial load.
- chronic bronchitis
- bronchial inflammation
- bacterial infection
Statistics from Altmetric.com
Exacerbations of chronic bronchitis cause substantial morbidity and mortality and their frequency has a significant impact on patient quality of life.1 In addition, there is evidence that exacerbation frequency influences decline in lung function.2,3 However, exacerbations vary in their clinical presentation (characterised by combinations of increased breathlessness, sputum volume, and new or increased sputum purulence4) and in their aetiology, which may be viral, bacterial, or due to increased airflow obstruction alone. This heterogeneity complicates the study of the episodes. For instance, inflammation is thought to be central to the pathogenesis of chronic obstructive pulmonary disease (COPD) but not all exacerbations are associated with increased inflammation,5 hence the relationship of exacerbations and inflammation to COPD progression remains unclear.
The importance of positive cultures in sputum from patients with chronic bronchitis has been the subject of some uncertainty.6 Pathogenic bacteria are frequently isolated from sputum obtained at the time of exacerbation, but the observation that such bacteria are also found in sputum and the oropharynx when patients are clinically stable7 has raised doubts about their role. The frequency of isolation of bacteria undoubtedly increases during exacerbation, but this is limited to those in whom purulent sputum is a key feature.8 In many of these patients bacterial isolation is a new feature, but in some bacteria are still present in the stable clinical state.
Evidence suggests, however, that bacteria promote inflammation even in stable chronic bronchitis9 and this is in part determined by the bacterial load.10 In vitro studies have shown that Haemophilus influenzae is proinflammatory11 and that different strains of this organism vary in their ability to promote inflammation. Those that do not persist induce more pronounced inflammation (at least in vitro) than those that do persist, and this effect is independent of the load.12 The reasons are unknown at present, but the fact that persisting strains are less able to stimulate a host inflammatory response may explain their continued colonisation when patients appear clinically stable. Furthermore, a recent study has shown that lower airway bacterial colonisation influences both the character and frequency of exacerbations.13
Inflammation increases during exacerbations5 and workers have suggested that the organisms isolated during these episodes differ in their ability to stimulate inflammation from those isolated in the stable state.14 In patients with bronchiectasis, sequential sampling of patients colonised with H influenzae has shown that some exacerbations are associated with changes in the outer membrane protein gene, while the phenotype is similar to the stable state isolate.15 Furthermore, molecular typing has shown that multiple strains of H influenzae coexist in some of those colonised with this organism,16 and it is possible that these strains vary in their ability to promote inflammation. Thus, four potential mechanisms associated with bacteria may result in the changes in bronchial inflammation associated with exacerbation: (1) acquisition of a new organism, (2) antigenic drift of colonising bacteria, (3) an increase in colonising bacterial load, or (4) a relative increase in the proportion of strains with increased inflammatory potential. Stimulation of inflammation is therefore likely to be dependent on the nature of the organism and, perhaps more importantly, the numbers.10
The purpose of the present study was to investigate the relationship between bacteriology and inflammation at the onset of exacerbation, 10 days later, and subsequently in the stable clinical state, some 2 months later. In particular, we wished to determine the effect of positive bacterial isolates, number of organisms, and changes associated with subsequent sterilisation of the airways or persistent colonisation.
METHODS
Patients
Patients aged 40–80 years who presented with an acute exacerbation of chronic bronchitis (daily sputum production for at least 3 months of 2 consecutive years) were studied. Global inflammatory data and the principles of identifying bacterial causes of exacerbation for some of these patients have been presented previously.5,8 The exacerbation was characterised by a combination of worsening respiratory symptoms which included at least one of breathlessness, sputum volume, colour, with or without sputum viscosity, cough, wheeze or chest pain, or systemic symptoms (malaise, fever, rigors) which caused the patient to seek medical advice (adapted from Anthonisen et al4). Patients who had received antibiotics within the preceding 4 weeks and those requiring systemic steroids were excluded from the study. If the history or examination suggested possible pneumonia, patients underwent chest radiography and were excluded where this was confirmed.
Sputum classification
A fresh spontaneous sputum sample was obtained at presentation (day 1) and allocated a number by reference to a standard colour chart,17 reflecting sputum purulence. Only patients in whom sputum colour was graded as at least number 3 on the colour chart (any yellow colouration through to darkest green) were included in the analysis (n=54). An adequate sputum sample was defined by the presence of more than 25 polymorphonuclear leucocytes and less than 10 squamous cells per low power field (×100) as described by Chodosh.18 Quantitative sputum culture was performed on an aliquot of the initial sample as described previously.19 Only those patients with a positive bacterial culture of a known respiratory pathogen at presentation were included in the follow up analysis. Patients were classified as pathogen positive or pathogen negative on day 10 after starting antibiotic treatment and 2 months later (the stable clinical state).
The remaining sputum sample was centrifuged at 50 000g (4°C) for 90 minutes and the sputum sol phase was separated and stored at −70°C until analysis. Ten ml of blood was also obtained, allowed to clot, centrifuged at 3000 revolutions per minute, and the serum was stored at −70°C until required.
Treatment protocol
All patients were treated and followed as outpatients. They received up to 10 days of continuous treatment with oral cefuroxime axetil (500 mg twice a day), chosen for its known activity against the common pathogens associated with exacerbations of chronic bronchitis.20
Patient follow up
Patients were reviewed 10 days after starting treatment and at 2 months, when in the stable clinical state. Patients who had relapsed and required further treatment were also seen around this time, but at least 2 weeks after any episode had resolved. Further blood and sputum samples were taken at these times, processed, and stored as stated previously. All patients had HRCT scans performed to assess for the presence of bronchiectasis using the criteria first described by Naidich et al.21 Subjects with cystic/varicose bronchiectasis were excluded from further analysis.
Biochemical analysis
Myeloperoxidase (MPO) (as a marker of neutrophil numbers and activation), neutrophil elastase (NE), the chemoattractants interleukin 8 (IL-8) and leukotriene B4 (LTB4), and secretory leukoprotease inhibitor (SLPI) were measured as described previously.22 Sputum sol and serum albumin were measured by radial immunodiffusion to provide an assessment of protein “leakage” from the blood into the lung.23
Statistical analysis
All statistical analyses were performed using the SPSS statistical package (Version 10.0; Chicago, USA). Age and forced expiratory volume in 1 second (FEV1) are expressed as mean (SD) and the patient groups were compared using the unpaired t test. χ2 or Fisher’s exact tests were used to compare categorical data between groups and within groups where necessary. Inflammatory data are expressed as median values with interquartile range or displayed graphically. Changes within groups were analysed using the Wilcoxon signed rank test for paired data, and differences between patient groups were compared using the Mann-Whitney U test. Two tailed tests were used to compare the concentrations of markers of inflammation and bacterial numbers at presentation. As resolution of exacerbations has previously been shown to be associated with a reduction in bronchial inflammation, single tailed tests were used for within group analysis of markers of inflammation from exacerbation through to the stable state. In addition, because bacteria stimulate inflammation, we tested our a priori assumption that eradication of bacteria would result in greater reductions in inflammation using single tailed tests for the between group comparisons at day 10 and in the stable state. The level of statistical significance was taken as <0.05.
The study was approved by the South Birmingham Health Authority ethics committee and all subjects provided written informed consent.
RESULTS
A positive culture of pathogenic bacteria was obtained in 48 of the 54 patients who presented with an acute purulent exacerbation of chronic bronchitis; 41 of these patients also provided an adequate sputum sample at day 10, and 46 provided an adequate sample 2 months later.
Sputum microbiology at presentation
The pathogens isolated at presentation were H influenzae (n=27), Moraxella catarrhalis (n=9), Streptococcus pneumoniae (n=6), Haemophilus parainfluenzae (n=9), Neisseria meningitides (n=1), and Escherichia coli (n=1) (some patients had more than one pathogen). The median bacterial load for the whole group was 3 × 108 cfu/ml (interquartile range 3.6 × 107−1.0 × 109).
Changes in bacteriology by day 10
Seven of the 48 patients with positive sputum cultures were unable to produce a sample on day 10. Of the remainder, 17 samples (41%) cultured at least one respiratory pathogen including H influenzae (n=10), M catarrhalis (n=4), and H parainfluenzae (n=3). The changes in bacterial load observed between presentation and day 10 are shown in table 1. By day 10 all but six of the patients had some symptom resolution. Of these, two were culture negative and four had bacterial persistence (p=NS).
Changes in markers of bronchial inflammation and bacterial load from day 1 to day 10
Changes in bacteriology between day 1 and the stable state
Forty six of the initial 48 patients produced adequate sputum samples at the 2 month visit. Eighteen (39%) of these cultured at least one recognised respiratory pathogen including H influenzae (n=11), M catarrhalis (n=4), H parainfluenzae (n=4), Pseudomonas spp (n=1), and Staphylococcus aureus (n=1). The bacterial load was significantly lower than at presentation in these 18 patients (table 2). The characteristics of patients with and without bacterial persistence at the two time points are summarised in table 3. Between presentation and the stable assessment 10 of the 48 patients had symptoms of an exacerbation that required further treatment. The median time after initial presentation that further treatment was given was 19.5 days (minimum 10, maximum 24). Three of the 10 patients required a short course of oral corticosteroid and the remainder had further antibiotic therapy. Five of these patients had a positive culture in the stable clinical state and five were pathogen negative.
Changes in markers of bronchial inflammation from day 1 to the stable state
Characteristics of patients with and without bacterial persistence at day 10 and in the stable state
Markers of bronchial inflammation
The inflammatory markers at presentation showed a wide range consistent with our previous data.5 The median (interquartile range) values for the group as a whole were: MPO 0.92 units/ml (0.45–2.00), NE 8.73 nM (0.96–32.31), LTB4 8.36 nM (5.05–21.96), IL-8 5.82 nM (2.96–12.73), SLPI 1.33 μM (0.50–3.03), sol:serum albumin ratio 1.51% (0.69–3.36). Concentrations of all markers of bronchial inflammation were the same in both groups at presentation (tables 1 and 2), with the exception of albumin leakage which was greater in those in whom bacteria continued to be isolated, especially in the stable state (table 2).
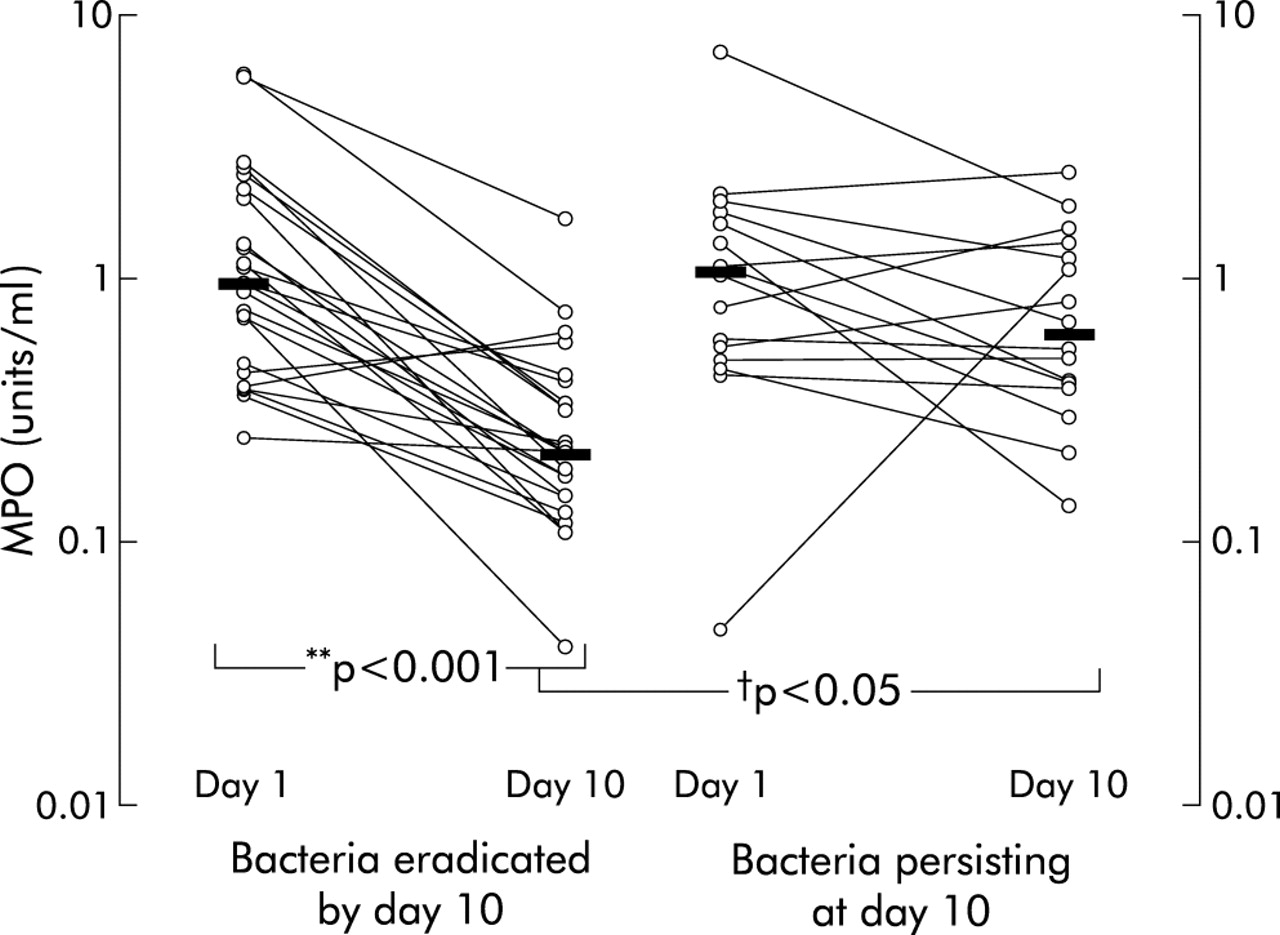
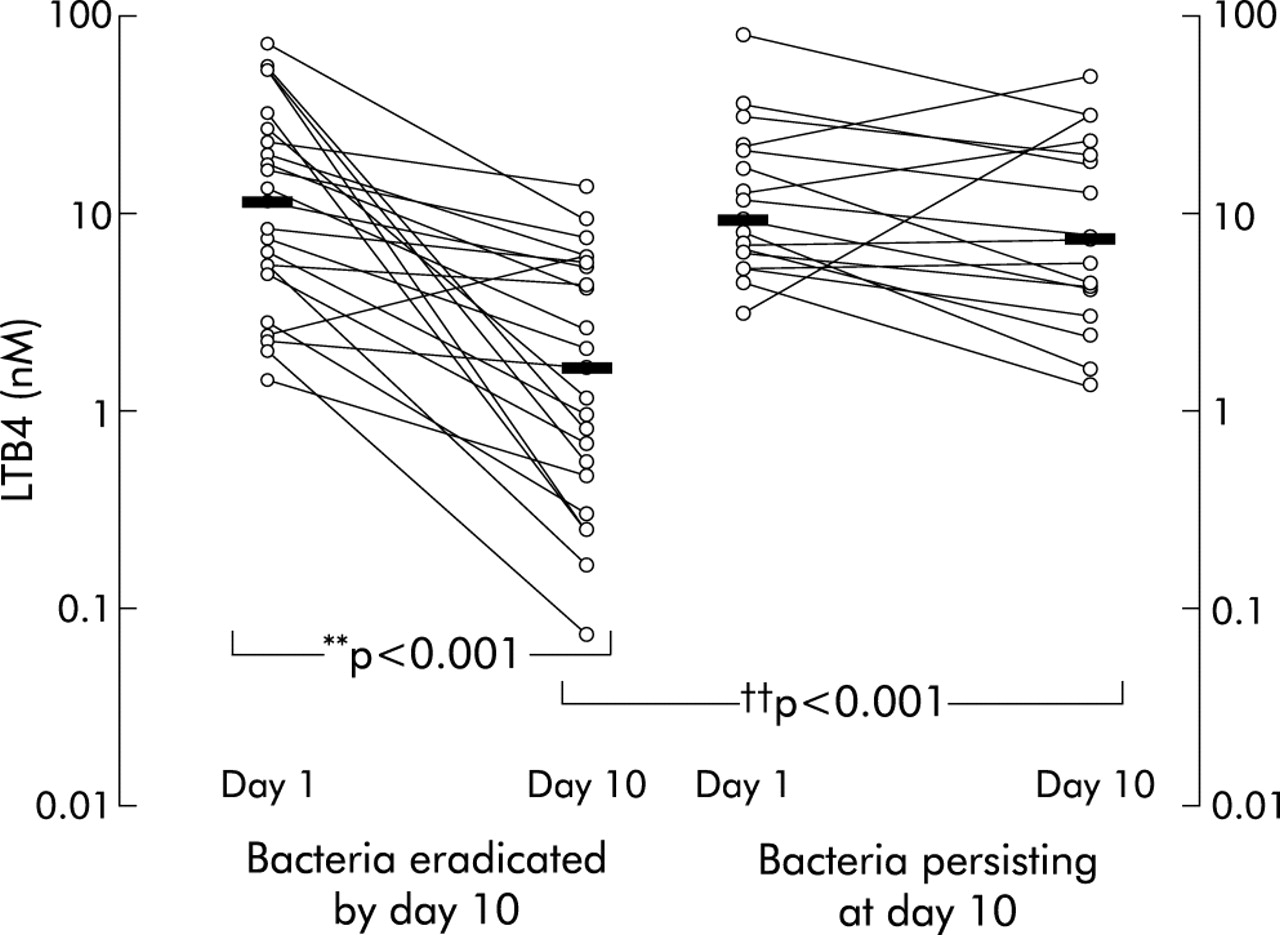
By day 10 a significant fall in inflammatory markers (MPO, NE, LTB4, IL-8, and albumin leakage) was observed in subjects in whom the bacteria had been eradicated, but in those in whom bacteria persisted only NE and albumin leakage fell (table 1, figs 1–3). During the first 10 days there was no significant change in SLPI in either group. The concentrations of MPO and LTB4 at day 10 were lower in the group in whom the bacteria were eradicated than in those who continued to have pathogens cultured in their sputum (table 2, figs 1–3). Furthermore, when the changes in these markers were compared, there was a significantly greater fall in MPO and LTB4 in the group in whom bacteria were eradicated (table 4).
Changes in markers of bronchial inflammation between days 1 and 10 and day 1 and the stable clinical state, comparing those eradicating bacteria with those patients with persistent pathogens

Change in myeloperoxidase (MPO) concentration (on a logarithmic scale) between presentation and following treatment (day 10). The individual data points for a given patient are joined by a straight line for both the “eradicated” and “persisting” groups. The horizontal bar represents the median MPO value for each group. There was a reduction in sputum MPO concentration in patients in whom bacterial pathogens were eradicated (**p<0.001), but there was no significant change in those in whom bacteria persisted. At day 10 those with bacterial persistence had higher concentrations of MPO than those eradicating pathogens (†p<0.05).

Change in leukotriene B4 (LTB4) concentration (on a logarithmic scale) between presentation and following treatment (day 10). The individual data points for a given patient are joined by a straight line for both the “eradicated” and “persisting” groups. The horizontal bar represents the median LTB4 value for each group. There was no difference between the groups at presentation, but by day 10 the concentration was lower in those in whom bacteria were eradicated (††p<0.001). The LTB4 concentration fell in this group (**p<0.001) but in those with bacterial persistence no significant fall was observed.

{kind=link}
{kind=link}
{kind=link}
Change in albumin sol:serum ratio (on a logarithmic scale) between presentation and following treatment at day 10. The individual data points for a given patient are joined by a straight line for both the “eradicated” and “persisting” groups. The horizontal bar represents the median sol:serum ratio value for each group. The reduction in sol:serum ratio was significant for both patient groups (both **p<0.001).
When studied in the stable state, there was only sufficient sample to carry out biochemical assessment in 40 patients. Both groups showed a resolution of airways inflammation as indicated by the fall in albumin leakage. The remaining changes (MPO, NE, LTB4 and SLPI) were most marked in the group in whom bacteria had been eradicated. Furthermore, the concentrations of MPO, NE, and LTB4 were lower and SLPI was higher in this group than in samples obtained from those who continued to have viable pathogens cultured in their sputum (table 2). The changes in LTB4 and SLPI were greater when bacteria were eradicated (table 4), although the difference in change in MPO did not quite achieve statistical significance. Interestingly, IL-8 concentrations did not change in either group (table 2).
The changes in bronchial inflammation were reflected in changes in sputum colour which became less purulent when bacteria were eradicated. Sputum colour was the same in both groups at presentation (mean (SE) colour number 4.15 (0.12) in those in whom bacteria were eradicated v 4.28 (1.6) in those with bacterial persistence). However, colour number fell more in those with bacterial eradication (p<0.05) and was lower by the stable state in those in whom bacteria were eradicated than in those in whom bacteria persisted (2.35 (0.16) v 3.11 (0.29), p=0.009). These data are consistent with previous work showing the relationship between sputum colour and inflammation24 and bacteriology.8
We also analysed data from the subgroup of patients in whom a pure growth of H influenzae was isolated at the exacerbation and assessed differences in inflammation based on bacterial eradication. Again, markers of bronchial inflammation in those in whom bacteria were eradicated and those with persistent bacteria were broadly similar at presentation and behaved in a similar fashion to the whole group (results are shown in tables 5 and 6 available in the online Thorax data supplement at www.thoraxjnl.com/supplemental). The concentrations of MPO were similar at presentation in subjects in whom bacteria were eradicated by day 10 and those in whom bacteria persisted (median (IQR) 1.33 (0.75–2.46) units/ml v 1.15 (0.52–1.71) units/ml), but differed significantly at day 10 (median (IQR) 0.22 (0.15–0.33) units/ml v 0.44 (0.31–0.72) units/ml, p<0.05). Likewise, the concentration of LTB4 at presentation was similar in both groups (median (IQR) 9.88 (4.70–22.20) nM v 7.68 (5.00–30.12) nM), but by day 10 it was lower in those with bacterial eradication (median (IQR) 2.27 (0.29–4.30) nM v 12.37 (2.34–19.28 nM, p<0.05). In the stable state, however, there was no significant difference in MPO or LTB4 concentration between the two groups (MPO: 0.28 (0.11–0.39) units/ml v 0.31 (0.16–2.38) units/ml; LTB4: 4.72 (2.50–5.99) nM v 7.24 (2.80–27.85) nM. In this subset of patients IL-8 fell significantly over the first 10 days in both those in whom bacteria were eradicated as well as those with persistent bacteria (from 8.18 (3.86–15.91) nM to 2.35 (0.89–4.64) nM, p<0.03 and from 7.57 (5.36–12.88) nM to 4.64 (2.81–5.64) nM, p<0.03, respectively).
DISCUSSION
These results provide strong evidence in support of the role of bacteria in bronchial inflammation, both during exacerbations of chronic bronchitis and following their resolution. The reduction in bronchial inflammation observed was shown to relate to eradication of bacteria, whether in the short (10 days) or longer term (2 months), and supports the hypothesis that bacteria stimulate the inflammatory process during these episodes. Bronchial inflammation also decreased (although less completely) in those with persisting bacteria, and this may reflect the fall in bacterial load10 in the stable state after the episode. This short term study occurs in a phase where bacterial isolation reflects (in some patients) the loss and reacquisition of some organisms. The reacquisition may reflect a different phenotype which could influence the results.25 This possibility has only been described recently and could not therefore be addressed in retrospect. Nevertheless, bacterial load is strongly associated with inflammation10 and, in general, the results presented here can be explained by such changes alone.
In this cohort of patients, failure to eradicate bacteria in the short term (over 10 days) was associated with greater use of inhaled corticosteroids before the exacerbation, although this was not found to be associated with longer term bacteriological status (table 1). The reasons for this observation are currently unclear and prospective studies are required to investigate this further. Airflow obstruction was similar in both groups (table 1), and there was no difference in the proportion of patients with mild tubular bronchiectasis identified on the CT scan.21
Albumin leakage was greater at presentation in those in whom bacteria persisted, although the explanation for this is not clear. It is possible that albumin leakage reflects the severity of the exacerbation or epithelial damage which may subsequently influence bacterial persistence. However, the similarity of other markers of inflammation makes this less likely. It is possible that the greater albumin leakage reflects some other (as yet) undetermined factor which influences bacterial persistence, and further work is needed to validate and resolve this issue.
Bacterial persistence was reflected most strongly in the concentrations of MPO, a marker of neutrophil recruitment and activation,24 and LTB4, an important neutrophil chemoattractant.26 In the short term a significant fall in IL-8 was observed but this effect was lost over the longer term. Interpretation of these changes in IL-8 is difficult because many cell types are capable of secreting this cytokine, including epithelial cells and neutrophils, and the source of sputum IL-8 in the stable state and during exacerbation is currently unknown. For instance, the short term fall in IL-8 could be due to a direct anti-inflammatory effect of an antibiotic.27 However, all patients were treated with a beta-lactam antibiotic which is not associated with such properties. Alternatively, it may reflect reduced production by epithelial cells damaged during the exacerbation rather than neutrophil recruitment and activation. In the stable state the IL-8 concentration was no longer different from that at presentation in the group in whom pathogens had been eradicated.
The reduction in albumin leakage from exacerbation to resolution was highly significant in both groups and there was no evidence that bacterial eradication influenced this reduction. Indeed, we have previously reported that increased albumin leakage is also associated with mucoid exacerbations (where bacteria are not implicated) and decreased with symptom resolution.5 The mechanism whereby albumin leakage occurs and resolves is poorly understood, but it may also be a marker for epithelial damage caused by viruses, other vascular inflammatory changes, as well as by mucosal invasion by bacteria or as a consequence of elastase release28 as part of the neutrophilic response. Resolution of albumin leakage in spite of bacterial persistence may reflect the reduced proinflammatory response induced by bacteria below a critical threshold, or reduced tissue invasion while colonisation of the airway lumen continues. Again, further studies will be necessary to determine the exact mechanism.
Concentrations of SLPI did not change over the first 10 days of the exacerbation in either group. However, SLPI had increased significantly in both groups 2 months after the exacerbation, and the increase was greater in those where bacteria had been eradicated than in those who were still colonised. Several potential mechanisms may explain the observed changes: (1) the initial low levels may be a reflection of the presence of NE activity which has been shown to reduce secretion of SLPI29; (2) secretion of SLPI may be reduced by epithelial tissue damage30 likely to occur during exacerbations; or (3) SLPI secretion may be reduced by bacterial products such as lipo-oligosaccharide (LOS) of H influenzae.31 The lower levels of SLPI found in patients who continued to be colonised could also reflect this LOS effect or may be a primary defect that predisposes to bacterial colonisation. This latter concept is supported by the fact that SLPI has antibacterial activity32 and by the observation that low SLPI levels are found in patients who experience increased exacerbation rates.33
It has been suggested that a change in the characteristics of the organism causes the increased inflammation in patients colonised with H influenzae when an exacerbation occurs.34 For this reason we analysed data from the subgroup of patients in whom a pure growth of H influenzae was obtained at the exacerbation. In general, the inflammatory data from these patients showed similar changes to those in the whole group in relation to the bacteriological status (results shown in tables 5 and 6 available in the online Thorax data supplement at www.thoraxjnl.com/supplemental). However, although inflammation fell when the organism persisted, this was also associated with a fall in bacterial numbers which would influence inflammation in its own right.10 Further studies with the individual isolates following extensive characterisation will therefore be necessary to clarify any potential difference in the proinflammatory nature of the organisms.
In summary, the results presented here show that resolution of bronchial inflammation associated with bacterial exacerbations of chronic bronchitis relates to clearance of bacteria. Persistence of bacteria is associated with partial resolution which probably reflects the change in bacterial load. Longitudinal studies are required to investigate this association more closely, especially the influence of prior colonisation on inflammation during exacerbation.
REFERENCES
Supplementary materials
. Web-only Tables
The tables are available as downloadable PDFs (printer friendly files).If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [View PDF] - Changes in markers of bronchial inflammation from day 1 to day 10 in those with Haemophilus influenzae cultured at exacerbation
- [View PDF] - Changes in markers of bronchial inflammation from day 1 to the stable state in those with Haemophilus influenzae cultured at exacerbation
Footnotes
-
The study was supported by an unrestricted research grant by GlaxoSmithKline. Dr White’s salary was funded by Bayer.