Article Text

Abstract
Background: Exacerbations represent an important feature of the clinical manifestation and natural history of chronic obstructive pulmonary disease (COPD). Nuclear localisation of p65 is a signal of nuclear factor-κB (NF-κB) activation. A study was undertaken to evaluate whether NF-κB activation is modified in sputum cells during COPD exacerbations.
Methods: Total and nuclear p65 immunoreactivity was measured by immunocytochemistry in the sputum cells of 11 smokers with moderate COPD during an exacerbation and after 6–8 weeks of clinical stability.
Results: Total sputum cell count was significantly increased during exacerbations from a median (IQR) of 880 (510–1865) to 1914.5 (1065–3205) × 103/ml (p<0.05). The main inflammatory cells in the sputum were neutrophils (83.2 (75.4–92.3)%) and macrophages (14.7 (2.6–21.6)%) and their relative proportion did not change during exacerbations. Nuclear staining for p65 was absent in sputum neutrophils, both during exacerbations and in the stable phase. In contrast, the percentage of macrophages expressing nuclear p65 increased significantly during exacerbations from a median (IQR) of 16 (7–24)% to 41.4 (6–69)% (p<0.05).
Conclusions: NF-κB appears to be activated in sputum macrophages but not in sputum neutrophils during exacerbations of COPD
- p65
- chronic obstructive pulmonary disease
- sputum neutrophils
- sputum macrophages
Statistics from Altmetric.com
Exacerbations represent an important feature of the clinical manifestation and natural history of chronic obstructive pulmonary disease (COPD),1 and are associated with a transient acute-upon-chronic increase in airway inflammation.2 In stable COPD there is infiltration of T lymphocytes (with an increased CD8+/CD4+ ratio), macrophages and neutrophils into the airway,2 associated with increased expression of inflammatory mediators such as cytokines, chemokines, and adhesion molecules.3 The genes for a number of cytokines and proteins involved in airway inflammation in COPD are regulated by nuclear factor-κB (NF-κB).4 NF-κB is a heterodimer of p65 and p50 which, in unstimulated cells, is localised to the cytoplasm. Upon activation, NF-κB translocates into the nucleus where it binds to specific κB elements in the promoters of target genes.4 The nuclear expression of p65 is therefore a signal of NF-κB activation.4 Induced sputum has been used to characterise inflammatory cells and mediators involved in COPD exacerbations.5 The aim of this study was to evaluate whether NF-κB activation is modified during COPD exacerbations.
METHODS
Subjects
Eleven smokers with moderate COPD were examined during an exacerbation and after 6–8 weeks of clinical stability (table 1). A COPD exacerbation was defined as increased dyspnoea associated with a change in quality and quantity of sputum which led the subject to seek medical attention.1 Patients enrolled underwent clinical/functional assessment and sputum collection within 24 hours of the beginning of the exacerbations, before any change in their pharmacological treatment. They had no history of asthma or other allergic disease. There was one current smoker and the others were all ex-smokers with a smoking history of >20 pack-years (mean (SE) 60.5 (12.5)). The medical history was taken and physical examination, pulmonary function tests, and a single time sputum cell analysis were performed during both the exacerbations and when clinically stable. Chest radiographs were performed during exacerbations to exclude pneumonia. All patients remained on their treatment for the duration of the study. Exacerbations were treated with systemic glucocorticoids and, when indicated, antibiotics.1
Characteristics of study patients (n=11)
The study was approved by the ethics committee of the University Hospital of Ferrara and all patients gave their written informed consent.
Pulmonary function
Pulmonary function tests (Biomedin Spirometer, Padova, Italy) were performed as previously described.6
Lung tissue processing
Lung parenchyma was obtained from seven male smokers with moderate stable COPD (age 74 (1) years; smoking history 35 (5.6) pack years; forced expiratory volume in 1 second (FEV1) 1.8 (0.08) l, forced vital capacity (FVC) 2.97 (0.14) l; FEV1/FVC 63.1 (1.8)) undergoing lung resection for a solitary peripheral carcinoma.
Two to four randomly selected tissue blocks (template size 2 × 2.5 cm) were taken from the subpleural parenchyma of the lobe obtained at surgery, avoiding areas involved by tumour. Samples were fixed in 4% formaldehyde in phosphate buffered saline (PBS) at pH 7.2 and, after dehydration, embedded in paraffin wax. Tissue specimens were orientated and 4 μm thick serial sections were obtained for immunohistochemical analysis.
Sputum collection and analysis
Sputum was collected after bronchodilator inhalation and analysed as previously described.6 Sputum plugs from the lower respiratory tract were selected for sputum cell counts. The total cell count was standardised for the sample size (ml) as previously described.6 Cytospin slides were prepared and dried for 30 minutes. The slides were wrapped in aluminum foil and stored at –20°C before immunostaining. An average of six slides were prepared from each patient.
Immunocytochemistry for p65 in sputum cells
Sputum immunocytochemistry with alkaline phosphatase was performed as previously described with some modifications.7 Cytospins were fixed with periodate-lysine-paraformaldehyde (PLP, 10 minutes), washed (15% sucrose, 20 minutes, 22°C), and cells permeabilised (0.1% nonidet-P40/PBS). Non-specific binding was blocked (5% normal goat serum, 20 minutes, 22°C) before incubation with the specific rabbit anti-p65 (sc-372, Santa Cruz Biotechnology, USA; 1:50 dilution, 1 hour, 22°C) and p65 detected using alkaline phosphatase (Vectastain ABC alkaline phosphatase kit, Vector Laboratories, Burlingame, CA, USA) and fast-red substrate according to the manufacturer's instructions. Negative control slides were included in each staining run for each patient for both exacerbations and the stable phase. p65+ cells were quantified for cytoplasmic and/or nuclear staining by two independent blinded observers; 400 cells staining red, indicating p65 immunoreactive cells, were counted on each slide. The mean intra-observer and inter-observer coefficients of variance with counting were less than 10%.
Immunoperoxidase double staining for CD68/p65 in lung sections
After deparaffinisation and rehydration to expose the immunoreactive epitopes of CD68 and p65, the sections to be stained were immersed in citrate buffer 5 mM at pH 6.0 and incubated in a microwave oven (Model NN S200W; Panasonic, Milano, Italy) on high power. Endogenous peroxidase activity was blocked by incubating the slides in 3% hydrogen peroxide in PBS followed by washing in PBS. Cell membranes were permeabilised by adding 0.1% saponin to the PBS. Non-specific labelling was blocked by coating with blocking serum (5% normal horse serum) for 20 minutes at room temperature. After washing in PBS the sections were incubated for 1 hour at room temperature with mouse anti-human CD68 (Dako) at a dilution of 1:100 of a 160 μg/ml solution.
For negative control slides normal mouse non-specific immunoglobulins (Santa Cruz Biotechnology) were used at the same protein concentration as the primary antibody. After repeated washing steps with PBS the sections were incubated with anti-mouse biotinylated antibody (Vector ABC Kit, Vector Laboratories) for 30 minutes at room temperature. After further washing the sections were incubated with ABC reagent (Vector ABC Kit, Vector Laboratories) for 30 minutes at room temperature. The slides were then incubated with chromogen-fast diaminobenzidine (DAB) for 1–5 minutes. Non-specific labelling was again blocked by coating with blocking serum (5% normal goat serum) for 20 minutes at room temperature. After washing in PBS the sections were incubated for 1 hour at room temperature with rabbit anti human p65 (Santa Cruz Biotechnology) at a dilution of 1:50 of a 200 μg/ml solution.
For the negative control slides normal rabbit non-specific immunoglobulins (Santa Cruz Biotechnology) were used at the same protein concentration as the primary antibody. After repeated washing steps with PBS the sections were incubated with anti-rabbit biotinylated antibody (Vector Alkaline Phosphatase Kit, Vector Laboratories) for 30 minutes at room temperature and, after further washing, the sections were incubated with ABC reagent (Vector Alkaline Phosphatase Kit, Vector Laboratories) for 30 minutes at room temperature. The slides were then incubated with chromogen fast red for 10–20 minutes, after which they were counterstained in haematoxylin and mounted on aqueous mounting medium.
Statistical analysis
Data are expressed as mean (SE) or median and interquartile range (IQR) as appropriate. The groups were compared by the Kruskal-Wallis or Mann-Whitney U test as appropriate. Bonferroni's correction was applied when indicated.
RESULTS
The total sputum cell count was significantly increased during exacerbations from a median (IQR) of 880 (510–1865) × 103/ml to 1914.5 (1065–3205) × 103/ml (p<0.05). The main inflammatory cells in the sputum were neutrophils (83.2 (IQR 75.4–92.3)%) and macrophages (14.7 (2.6–21.6)%) and their relative proportion did not change significantly during exacerbations (86.7 (78.1–96.4)% and 12.4 (3.1–17.6)%, respectively, p=NS). Treatment with inhaled glucocorticoids (n=6) did not affect any parameters measured (data not shown).
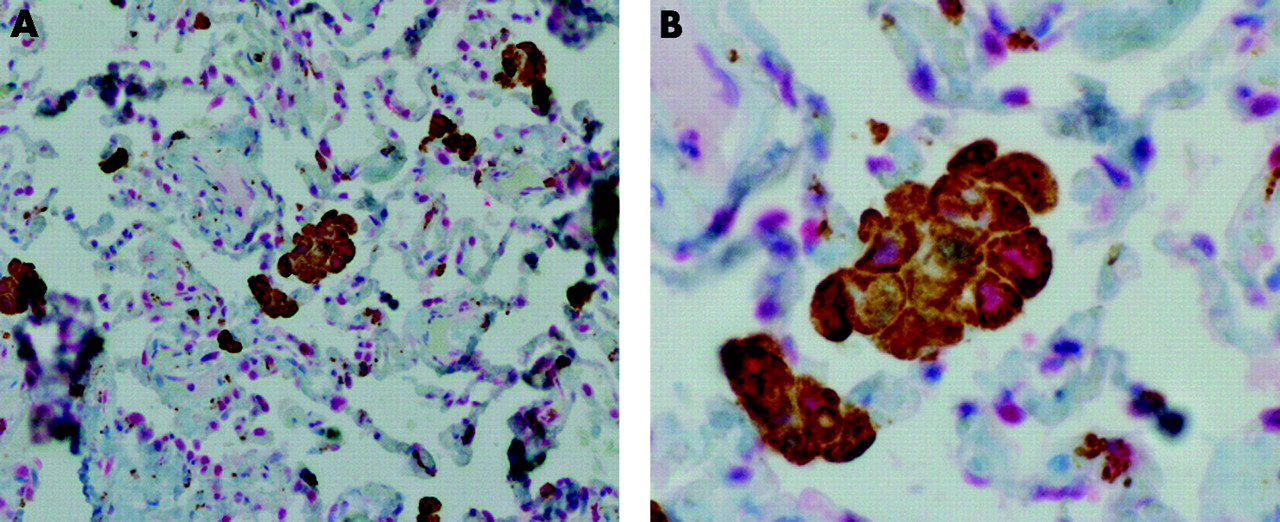
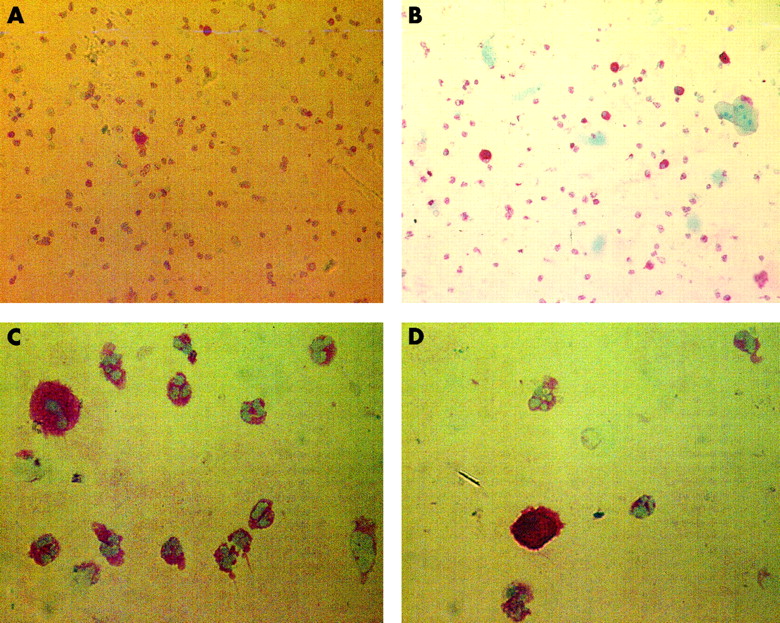
Most of the sputum inflammatory cells were p65 immunoreactive, both during exacerbations and during the stable phase (88 (81.1–93)% and 87.7 (71.5–88.7)%, respectively, p=NS; table 2). Nuclear staining for p65, an index of its activation, was absent in sputum neutrophils, both during exacerbations and in the stable phase (fig 1, table 2). In contrast, nuclear p65 was present in a proportion of sputum macrophages in the stable phase (16 (7–24)%) and was significantly increased during exacerbations (41.4 (6–69)%, p<0.05; fig 2, table 2). Treatment with inhaled glucocorticoids did not affect p65 nuclear expression (data not shown). Nuclear staining for p65 was present in CD68+ alveolar macrophages in the lung parenchyma as determined by double staining (fig 3).
Total and nuclear p65 immunoreactive sputum cells in patients with COPD during exacerbations and under stable conditions
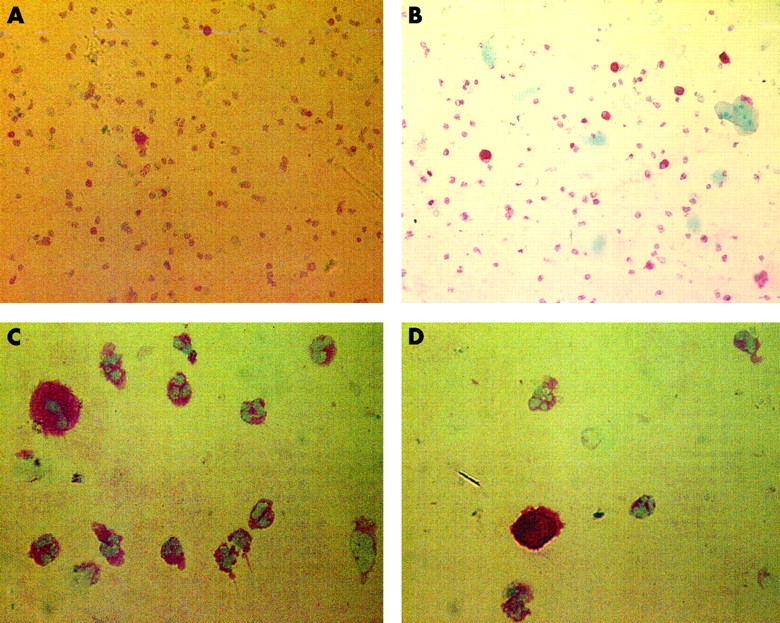
Representative immunocytochemical stain for p65+ cells (red) of a microscopic field rich in neutrophil granulocytes in a sputum cytospin sample from a patient with stable COPD (A and C) and during an exacerbation (B and D) at low (×400, A and B) and high (×900, C and D) magnifications.

Representative immunocytochemical stain for p65+ cells (red) of a microscopic field rich in alveolar macrophages in a sputum cytospin sample from a patient with stable COPD (A and C) and during an exacerbation (B and D) at low (×400, A and B) and high (×900, C and D) magnifications.
{kind=link}
{kind=link}
{kind=link}
Representative immunohistochemical stain of lung parenchyma from a patient with COPD double stained for identification of CD68 stained (brown) and p65+ stained (red) cells at (A) low magnification (×400) and (B) high magnification (×900).
DISCUSSION
NF-κB activation is increased in sputum alveolar macrophages from smokers with moderate COPD during exacerbations, as indicated by increased nuclear localisation of p65 protein. No nuclear p65 was found in sputum neutrophils from patients with stable COPD or during exacerbations. Although an increase in proinflammatory mediators whose synthesis is critically dependent on NF-κB activation has been previously reported in COPD,2,3 the role of NF-κB activation has not previously been evaluated. We speculate that, during COPD exacerbations, trigger factors such as viral and bacterial infections may lead to NF-κB activation, cytokine and chemokine production, and further inflammatory cell infiltration of the airways.2,3,5 The collection of bronchial biopsy specimens from subjects with COPD exacerbations is difficult to perform and is rarely accepted by the patients. Direct evidence of NF-κB involvement in bronchial inflammation during exacerbations of COPD is therefore difficult to obtain by the current methodology. However, using sputum immunocytochemistry we found evidence of p65 activation in alveolar macrophages during COPD exacerbations. Nuclear expression of p65 is recognised as a direct expression of NF-κB activation, although it does not directly record gene activation and protein production.4 In this study we have also shown, for the first time, nuclear localisation of p65 in CD68+ alveolar macrophages, confirming the presence of activated NF-κB in lung parenchyma macrophages of patients with stable COPD. Interestingly, we did not find any nuclear localisation of p65 in sputum neutrophils. The absence of nuclear staining for p65 is unlikely to be due to unsuccessful permeabilisation of the nuclear membrane of the neutrophils as we have observed clear nuclear staining for glucocorticoid receptors in sputum neutrophils using the same conditions of permeabilisation.8 Our results are in agreement with a recent report that the nuclear translocation of p65 can be induced in bronchoalveolar macrophages after stimulation with lipopolysaccharide.9 Interestingly, Gram negative bacterial infections are recognised as a possible cause of COPD exacerbations.10 In contrast, nuclear localisation of p65 has never been described in vivo in neutrophil granulocytes. The nuclear translocation of p65 has been shown in vitro in peripheral blood neutrophils following stimulation with high doses of proinflammatory cytokines (such as tumour necrosis factor alpha) and/or lipopolysaccharide.11 Clearly, further in vivo and in vitro studies are necessary to elucidate the differences in activation of the NF-κB pathway in macrophages and neutrophils observed in our study.
In this preliminary report we have shown evidence of NF-κB activation in bronchial inflammation during exacerbations of COPD, although this was restricted to alveolar macrophages. These findings suggest that NF-κB is involved in the activation of sputum macrophages, but not neutrophils, during COPD exacerbations.
Acknowledgments
This work was supported by grants from MURST (Grant 60%), GlaxoSmithKline UK and Italy, Associazione per la Ricerca e la Cura dell'Asma (ARCA, Padova, Italy) and AstraZeneca, Italy.