Article Text

Abstract
Background: This study aimed to describe the clinical, microbiological, molecular epidemiology and treatment of multidrug resistant tuberculosis (MDRTB) cases in the UK and to determine factors associated with survival.
Methods: Ninety MDRTB cases were identified from 1 January 1996 to 30 June 1997; 69 were DNA fingerprinted. Date of diagnosis was determined and data were collated on key demographic factors, clinical, radiological and treatment details. Variables associated with survival were included in a Cox proportional hazards model.
Results: Most of the patients (72.4%) were male, born outside the UK (57.1%), were sputum smear positive (82.2%), and had entered the UK more than 5 years previously (61.9%). Thirty eight of 78 cases (48.7%) had prior TB. Sufficient data on 82 patients were available for survival analysis; 20/27 (74.1%) known to be dead at the end of the observation period had died of tuberculosis. Median survival time overall was 1379 days (95% CI 1336 to 2515) or 3.78 (95% CI 3.66 to 6.89) years (858 days (95% CI 530 to 2515) in immunocompromised individuals (n=32) and 1554 (95% CI 1336 to 2066) days in immunocompetent cases (n=48)). Median survival in patients treated with three drugs to which the bacterium was susceptible on in vitro testing (n=62) was 2066 days (95% CI 1336 to 2515) or 5.66 years, whereas in those not so treated (n=13) survival was 599 days (95% CI 190 to 969) or 1.64 years.
Conclusions: Immunocompromised status, failure to culture the bacterium in 30 days or to apply appropriate three drug treatment, and age were significant factors in mortality. An immunocompromised patient was nearly nine times more likely to die, while application of appropriate treatment reduced the risk (risk ratio 0.06). Increasing age was associated with increasing risk of death (risk ratio 2.079; 95% CI 1.269 to 3.402)—that is, for every 10 year increase in age the risk almost doubled. Overall survival was lower than that reported in previous studies.
- multiple drug resistant tuberculosis
- mortality
- survival
Statistics from Altmetric.com
Tuberculosis (TB) remains a major cause of morbidity and mortality producing an estimated 8 million new cases leading to 2–3 million deaths annually.1,2 Clinical drug resistance is becoming of increasing importance worldwide and is attributed to factors including patient non-adherence to treatment, inappropriate treatment regimens, drug malabsorption, and a poor health infrastructure needed for the effective delivery of treatment. The most difficult clinical cases are caused by multiple drug resistant tuberculosis (MDRTB) defined as resistance to at least isoniazid and rifampicin. These drugs constitute the mainstay of treatment and knowledge of resistance is likely to be of direct benefit to the individual patient and to public health TB programmes. MDRTB is increasingly recognised as a serious global clinical, microbiological, and public health problem.
The global incidence and prevalence of MDRTB is unknown. In part this has been due to methodological problems including the absence of longitudinal studies to detect trends, the failure to differentiate primary and acquired drug resistance in studies, the selection bias of many surveys, and the absence of high quality culture facilities.3
To address this, a joint World Health Organisation (WHO) and International Union Against Tuberculosis and Lung Disease (IUATLD) Project on Antituberculosis Drug Resistance Surveillance reported results from 35 countries which included a total of 50 000 cases.4 Drug resistance was seen in all countries. MDRTB was widespread with a third of countries surveyed having levels above 2% in new patients (median prevalence 1–4%, range 0–14%). High rates were found in former countries of the USSR, the Baltic Republics, Argentina, India and China.3
In the UK the steady reduction in TB cases reversed in 1987 and currently there are 6000 new cases per annum. Notification rates of 9.2 and 10.1/100 000 were reported in those not previously treated in England and Wales in 1993 and 1998, respectively.4,5 Initial MDRTB rates in the UK from 1993–6 increased from 0.6% to 1.7% (from 19 to 60 cases), declining to 0.8% (33 cases) in 1999.6 As in the USA, drug resistance is not evenly dispersed within the UK, with all measures of resistance being highest in England, particularly London.6
Earlier studies indicated that survival of MDRTB cases, particularly if patients are co-infected with HIV, is poor.7,8 Recent studies in New York and Korea have suggested that the early institution of treatment based on the results of in vitro susceptibility testing have been associated with improved survival, but most have followed small numbers of cases for relatively short periods of time.9–13
This study is the first national study of MDRTB cases in the UK in which the principal clinical, bacteriological, and epidemiological features underlying these cases are described and the effects of these factors on survival determined.
METHODS
Bacteriological culture, identification, drug resistance
Mycobacteriological cultures were referred from NHS hospitals and identified using standard microscopic and biochemical methods or DNA hybridisation techniques14 at the Public Health Laboratory Service (PHLS) Mycobacterium Reference Unit (MRU), the Scottish Mycobacteria Reference Laboratory (SMRL), and PHLS Regional Centres for Mycobacteria (RCM) in Birmingham, Cardiff, and Newcastle. These units identify 90–95% of all new bacteriologically proven TB cases in the UK. Drug resistance was identified using the resistance ratio or proportion methods in Lowenstein-Jensen or Bactec media using standard procedures.15,16 All isolates were tested for isoniazid, rifampicin, ethambutol, and pyrazinamide. Although the four centres assay the same first line drugs, there are some differences in the second line drugs tested—for example, streptomycin and ciprofloxacin are routinely tested at the PHLS MRU but not at other centres. Most isolates were repeat tested for drug susceptibility (DST), with third line agents assayed only at the PHLS MRU and SMRL. All MDRTB cases identified by the above centres from 1 January 1996 to 30 June 1997 were included.
Molecular epidemiology
Cultures were DNA fingerprinted using the IS6110 insertion sequence in accordance with standard protocols.17
Clinical and epidemiological factors
The exact date at which each case was first diagnosed bacteriologically was determined. A standard questionnaire was formulated and reviewed and approved by the independently chaired PHLS ethics committee. It was used to collate data from records at the MRU, RCMs and SMRL, from review of hospital records, and from the medical microbiologist in charge of the laboratory submitting the culture and the hospital physician (and/or TB nurse) treating the patient. Specifically, data were sought on sex, age at diagnosis, ethnicity, country of birth, year of entry into the UK where relevant, history of prior TB, and immunocompromised status. Clinical and radiological details were also sought. Brief details regarding treatment before the diagnosis of MDRTB were obtained, including whether combination fixed dose tablets had been used, whether three or four drugs had been administered, the choice of the fourth drug, and what drugs had been administered after the MDRTB diagnosis. Bacteriological details included specimen type from which the MDRTB isolate was cultured, microscopy smear status (pulmonary origin), whether three negative smears and/or one negative culture had been obtained on treatment after the MDRTB diagnosis, and the range of drug resistance occurring in each case. Cause of death was determined from review of the medical records and/or the death certificate.
All data were held on a secure password protected system in an Excel file format. Questionnaires were followed up with written and telephone reminders. The date of death or whether the patient was alive on 1 December 1997 and 1 December 1998 was obtained in order to determine the length of survival from first diagnosis.
Patient identifiers were removed and survival analysis was performed in SAS18,19 to generate a life table and median survival time, with time measured from the initial date that the primary sample was received by the laboratory for analysis. This was defined as the point of entry into the study. From this, variables were assessed for their potential significance for survival using log rank testing. Relevant variables were included in a Cox proportional hazards model.
RESULTS
Clinical, demographic, and bacteriological features of MDRTB cases
Bacteriological cultures from 90 MDRTB patients were identified by the participating laboratories during the study period. The principal bacteriological, clinical, and epidemiological factors associated with these patients are shown in tables 1, 2, and 3. Results, unless otherwise stated, are given as the number responding “yes” or, if drug resistance, the number “drug resistant”. Percentages are given using as denominator the number of patients for which data on the variable were known.
Patient demographic details
Clinical, microbiological, and radiological variables of patients
Summary of drug resistance profiles
Birth in the UK or abroad was known for 84 patients: 36 (42.9%) were born in the UK and 48 (57.1%) were born abroad. The country of birth was known for 83/90 (92.2%) patients. Seven (of 83 cases, 8.4%) were born in Pakistan, five (6.0%) in India, four (4.8%) in Bangladesh—that is, almost 20% of all cases where place of birth was known came from the Indian subcontinent. Similarly, 17 patients (20.5%) came from sub-Saharan Africa (20 (24.1%) from Africa as a whole; one (1.2%) from Algeria, two (2.4%) from an undefined African country, six (7.2%) from Somalia, two (2.4%) from Ethiopia, two (2.4%) from Uganda, one (1.2%) from each of Nigeria, Cameroon, Zaire, Sierre Leone, and Ghana). Four cases (4.8%) came from Europe (one (1.2%) each from Portugal, Italy, Lithuania and Turkey). Including the UK, 40 (48.2%) were known to have been born in Europe. One further case each came from the USA, Australia, Vietnam, China, Philippines, Japan, Trinidad, and Jamaica. Where the date of entry into the UK was known, 26 entered more than 5 years previously and 16 entered less than 5 years previously. In some individuals MDRTB was isolated from more than one site or was isolated from sputum specimens (in 74 individuals) and/or bronchial lavage (in five individuals). MDRTB was isolated from extrapulmonary sites in 14 individuals.
Table 3 indicates the range of drug resistance noted. By definition, all cases were resistant to at least isoniazid and rifampicin and 29 (32.2%) and 33 (36.7%) cases were resistant to pyrazinamide and ethambutol, respectively.
Transmission of MDRTB
Sixty nine viable isolates (76.7%) were available for DNA fingerprinting which linked 10 predominantly HIV positive patients (data not shown). Nearly all cases had been identified in previous studies of nosocomial transmission at hospitals in London.20,21 Interestingly, two further patients were identified as the same individual using two aliases at different hospitals.
Treatment and survival analysis
Table 4 summarises the treatment of MDRTB patients including the number of cases in which “appropriate therapy” was given, defined as chemotherapy with three drugs to which the bacterial isolate was sensitive on in vitro drug susceptibility analysis. A fourth drug was given empirically before diagnosis in 78 patients (86.7%) and was specifically identified in 42; most cases received ethambutol (n=35, 83.3%) or streptomycin (n=5, 11.9%). Capreomycin and ciprofloxacin were used in one case each.
Summary of MDRTB patient treatment
Fixed dose combination drugs were used in 48/73 (65.8%) cases (Rifinah, Rimactazid, and Rifater brands were specifically defined in 16, two, and 17 cases, respectively).
The principal end point analysed was survival, although patient improvement was judged by other descriptive criteria which were not necessarily used in the survival analysis. For example, the criterion “discharge from hospital” was not used as all patients were discharged unless they had died. Radiological improvement was seen in the chest radiograph of 45/74 (60.8%) cases, 35/67 (52.2%) patients had three negative sputum smears, and 39/71 (54.9%) patients had at least one negative culture.
There was sufficient date information available for 82 of the 90 patients (91.1%) to be included in the survival analysis. An asterisk in tables 1–4 indicates which variables were included in the survival analysis. The percentage of results missing for any variable (maximum n=82 in each case) and the result for each variable is also given in tables 1–4. For example, HIV status was not available for 11 of 90 patients but was missing from only five of 82 included in the model.
Overall there was an unequal distribution between the sexes with 63/87 (72.4%) of all cases and 58/81 (71.6%) of cases in the survival analysis being male. For the preliminary analysis, ethnic origin was split into four groups (African, n=18; Indian subcontinent (ISC), n=18; White, n=37; other, n=9). Age was divided into three groups as there were no patients under 15 years of age: 15–34 years (n=38); 35–54 years (n=32); and 55+ years (n=11). A patient was defined as “pulmonary” if the specimen type was sputum, the “sputum/BAL smear” was positive, or if the patient was productive of sputum. If none of these variables was present, the patient was defined as “extrapulmonary” (there were no cases which could not be defined into these categories): 73 (89.0%) were pulmonary patients.
The data available on the 82 cases were analysed using proc lifetest in SAS to generate a life table (table 5) and median survival times (table 5), with time being measured from the “initial sample received date” which is the study entry point. Table 6 summarises the survival statistics. Overall, the median survival time was 1379 days (95% CI 1336 to 2515) or 3.78 years (95% CI 3.66 to 6.89). The proportion surviving over time is represented graphically in fig 1. Twenty of 27 (74.1%) known to be dead at the end of the observation period had died of tuberculosis.
Summary statistics for the time variable (in days) for 82 patients.
Log rank test results of variables to determine those to be included in the Cox proportional hazards model
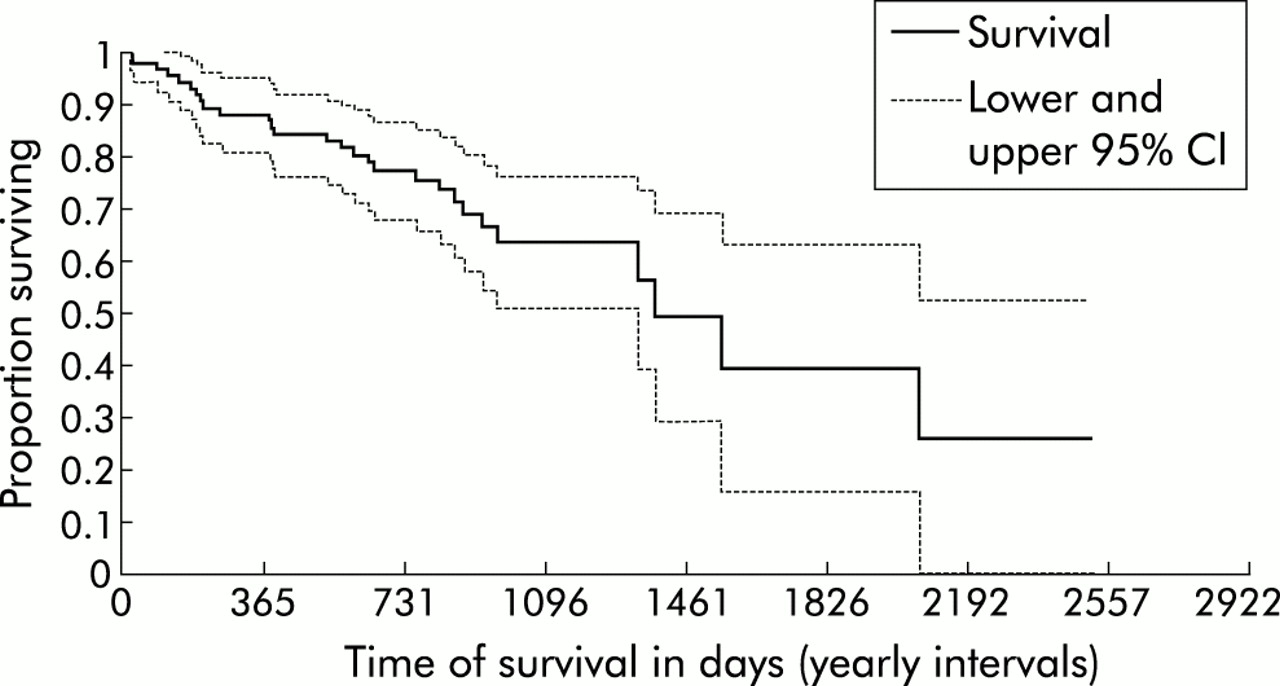
Proportion of MDRTB patients surviving over time.
By using the log rank test results, appropriate variables for inclusion in the Cox proportional hazards model18 were identified (table 6). Variables to be included were sex, immunocompromised status (IMMUNO), HIV status (HIV), whether a fourth drug was given before MDRTB diagnosis (PREMDR), whether appropriate three drug treatment was given based on in vitro testing (DRUGS3), whether there was concomitant resistance to pyrazinamide (PYRAZ), ethambutol (ETHAM), prothionamide (PROTH), amikacin (AMIK), the number of drugs the infecting organism was resistant to (DRUGS), age in 10 year units (AGEX), whether a bacterial culture was produced within 30 days (DAYSC), and whether a culture was produced and identified as MDRTB within 60 days (DID). This initial model could only use 44 of the 82 available cases (53.7%) due to missing information (data not shown). Using backward stepwise elimination, non-significant variables with large amounts of missing data were removed to obtain a final model which was able to use 55 of the 82 cases (67.1%); from this analysis, immunocompromised status, the application of appropriate three drug treatment, whether or not Mycobacterium tuberculosis was cultured within 30 days, and age were significant factors associated with survival. The results of the final model can be seen in table 7.
Analysis of final model of survival of MDRTB
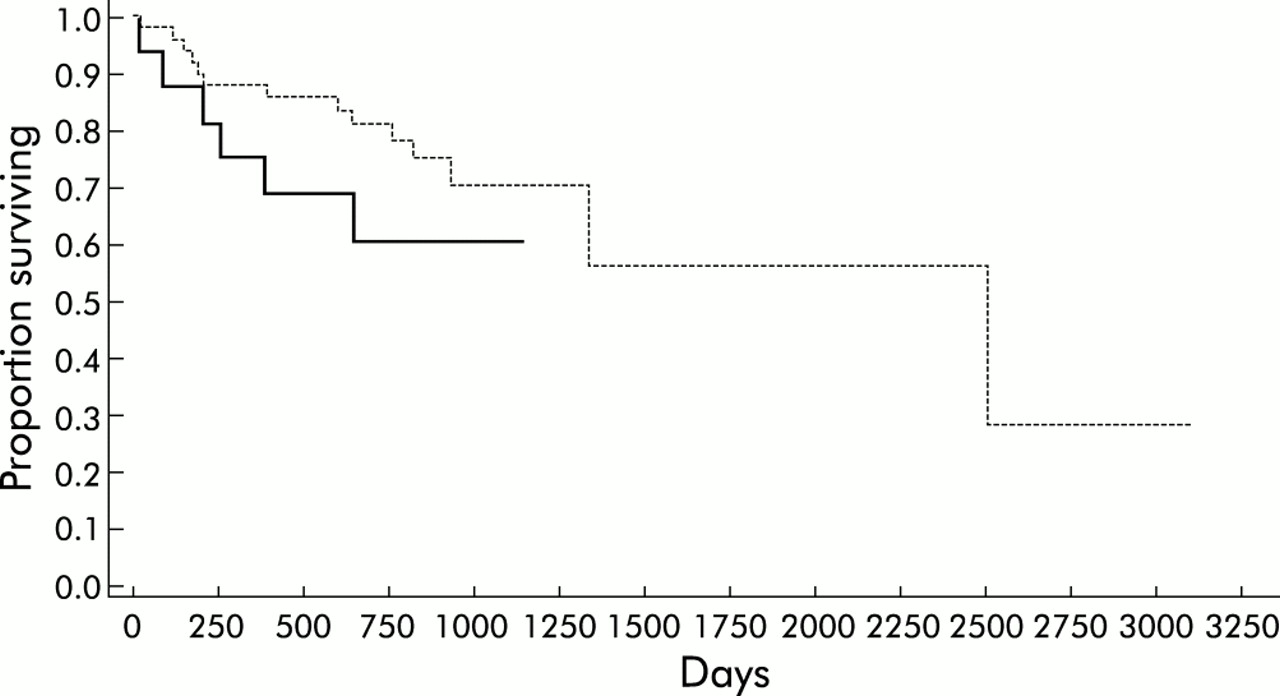
There was a significantly shorter median survival period of 858 days (95% CI 530 to 2515) in immunocompromised individuals (n=32) compared with 1554 days (95% CI 1336 to 2066) in those who were immunocompetent (n=48, fig 2).

Survival curves for immunocompromised (broken line, n=32) and immunocompetent MDRTB patients (solid line, n=48).
Of the cases where a culture was produced within 30 days (n=49) the median survival time was 2515 days (95% CI 1336 to incalculable). In the 16 cases where the culture was not produced within that time period the median survival time could not be calculated because 62.5% of these observations were censored (fig 3). Although significant differences in the survival time could not be calculated, those in whom the organism was cultured within 30 days were less likely to die with an estimated risk ratio of 0.23 (95% CI 0.06 to 0.86).

Survival curves for cases in which the specimen was cultured within 30 days (broken line) or not (solid line).
Figure 4 shows survival curves obtained when those patients treated with three drugs to which the bacterium was susceptible on in vitro drug susceptibility testing were compared with those treated with fewer agents with demonstrable susceptibility. In the former (n=62) the median survival period was 2066 days or 5.66 years (95% CI 1336 to 2515), whereas in the latter case (n=13) the median survival was 599 days or 1.64 years (95% CI 190 to 969).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curves obtained when patients treated with three drugs to which the bacterium was susceptible (dotted line ) on in vitro drug susceptibility testing were compared with those not so treated (solid line).
Survival was influenced by age. For those aged 15–34 years the median survival could not be calculated because, during the total study period, only 18.4% of the patients in this age group died—that is, 81.6% of patients were censored. For cases aged 35–54 years the median survival time was 1379 days (95% CI 649 to 2066) with 50.0% cases censored, and in the 55+ age group the median survival time was 2515 days (95% CI 119 to 2515) with 45.5% censored. There was, nevertheless, a general trend for risk of death at any specified time from entry to increase at a constant proportional rate with age (risk ratio 2.079; 95% CI 1.269 to 3.402)—that is, for every 10 year increase in age the risk almost doubled.
DISCUSSION
Previous studies, principally in the USA, have measured the therapeutic response microbiologically (conversion to sputum smear and/or culture negative) and/or clinically,7,10–13,22 with varying periods of follow up. This is the first national clinical UK study of survival of MDRTB cases and is also one of the largest and most comprehensive studies to date. Almost three quarters of the patients who died at the end of the observation period had died of tuberculosis.
MDRTB is a bacteriological diagnosis. It cannot be determined by clinical examination or by the application of epidemiological factors, although these are useful in determining those patients who are at greater risk of developing drug resistance. Appropriate laboratory infrastructures are required for the reliable identification of MDRTB. In the UK approximately 90–95% of all tuberculosis cultures are identified and the drug susceptibility determined by the participating centres using standardised methods. All bacteriologically proven MDRTB cases identified at these centres over an 18 month period were included and the date at which the first specimen producing an MDRTB culture was determined. Ninety cases were enrolled.
The majority of these patients (n=63, 72.4%) were male, born outside the UK (n=48, 57.1%), and had entered the country more than 5 years previously (26/42 cases with a date of entry, 61.9%). Birth in European countries including the UK, countries of the Indian subcontinent, and from Africa accounted for 71 cases. Of those in whom ethnicity was defined, 40 (46.5%), 19 (22.1%), 18 (20.9%), four (4.7%), and five (5.8%) were White, African, ISC, Afro-Caribbean or Oriental, respectively. Approximately half the cases (n=38, 48.7%) had had prior TB, although this figure is likely to be biased downwards as in many individuals there was an unbroken sequence of treatment at a single institution commencing with drug sensitive disease leading to stepwise accumulation of resistance.
Most patients had features typical of TB: fever (69/81, 85.2%), weight loss (64/79, 81.0%), a productive cough (69/84, 82.1%), and were sputum smear positive (65/78, 83.3%). Approximately half the patients were dyspnoeic (42/75, 56.0%). Chest pain and haemoptysis were rare. The chest radiograph was abnormal in 73/79 (92.4%) and severely so in almost two thirds of cases. Nearly 30% of the patients were known to be HIV positive.
Treatment of patients with TB throughout the study period conformed to the BTS guidelines published in 1990.23 For most cases this would have involved treatment for 2 months initially with three drugs (rifampicin, isoniazid and pyrazinamide) followed by 4 months of treatment with rifampicin and isoniazid. Four drugs were recommended initially if there was a likelihood of drug resistance. These guidelines were changed in 1998,24 recommending four drugs initially unless individuals were White, HIV negative, and known not to be contacts of drug resistant cases—that is, had a low risk of isoniazid resistance. Combination fixed dose tablets (FDC) were also recommended as an aid to compliance and to reduce the probability of resistance emerging through monotherapy. Some studies, however, have suggested poor bioavailability and poor treatment outcome using FDC.25 In this study 71/80 patients (88.8%) were given triple chemotherapy before MDRTB diagnosis and a fourth drug was given in 42/78 individuals (53.8%); 48/73 (65.8%) received FDC combination drugs at some point in their treatment before the diagnosis of MDRTB. No difference in survival was noted in those receiving combination medication, which suggests that, where FDC of proven bioavailability are used, the outcome will be comparable to those cases treated with single drugs. MDRTB emerges stepwise usually with isoniazid resistance initially; the use of two-drug FDC plus separate pyrazinamide in a poorly compliant individual with underlying isoniazid resistance may not prevent the emergence of MDRTB. Poor response rates were recently reported in isoniazid resistant patients on directly observed therapy (DOT).26 From the responses received, 43.1% and 47.1% of sputum smear positive patients had at least three negative smears and one negative culture, respectively, during the follow up periods; overall, 55% of patients had at least one culture negative sputum sample. Almost two thirds showed radiological improvement during treatment.
The analysis of the data set shows that survival time for MDRTB was significantly associated with three factors.
-
Patients who were immunocompromised had a significantly shorter median survival time (estimated risk ratio 8.67 (95% CI 1.36 to 55.4))—that is, immunocompromised patients with MDRTB were approximately nine times more likely to die than those who were immunocompetent. Concurrent HIV infection as a specific variable failed to achieve significance although it is likely that several immunocompromised cases were undiagnosed (or not stated) HIV positive cases. Historical reports, particularly from the USA in the early 1990s and in the two UK MDRTB outbreaks, indicated a low survival of MDRTB patients co-infected with HIV.8,20,21 The possibility of MDRTB should always be considered, regardless of HIV status.
-
A pattern of increasing risk with age was seen in the model with a risk ratio of 2.08 (95% CI 1.27 to 3.42)—that is, for every 10 year increase in age the risk almost doubles.
-
Whether a patient was given appropriate three drug treatment was also significant. The results suggest that those who received appropriate treatment would, on average, have a longer median survival time and a lower chance of death with an estimated risk ratio of 0.06 (95% CI 0.01 to 0.23). The usefulness of in vitro susceptibility testing is further supported by the fact that, of 39 streptomycin resistant cases, only seven (17.9%) were amikacin resistant—that is, the latter aminoglycoside would remain effective. Although there was no specific evidence to suggest a significant difference in survival time, those in whom the culture was produced within 30 days were less likely to die with a risk ratio of 0.23 (95% CI 0.06 to 0.86). The results indicate the importance of accurate in vitro drug susceptibility data in the clinical management of these patients. Although knowledge of the drug susceptibility profile within either 30 or 60 days was not associated with survival, there was a strong association between survival and accurate drug susceptibility data to guide treatment. Early culture of MTB was significant and it is reasonable to conclude that current combination treatment is able to ensure survival until definitive treatment can be introduced. However, early identification of MDRTB is important for immunocompromised patients in particular (who will die earlier than the immunocompetent) and for infection control to minimise the opportunity for cross infection.27 Early confirmation of MDRTB or that the bacteria in non-compliant persistently smear positive patients is drug sensitive can also reduce overall NHS costs.28 The PHLS MRU introduced a national molecular service for the rapid identification of rifampicin resistance as a surrogate of MDRTB in primary specimens 3 years ago and the MRU, RCMs and the SMRL identify cultures as MTB from new patients referred to them within 1–2 working days, a policy supported by this study. With novel automated liquid culture systems, culture and identification of MTB is achievable for all smear positive specimens—within 2 weeks in the majority of cases.
The longer follow up period and limited loss of cases in this study is important as survival in the first year supports the findings of earlier studies from New York which found excellent survival rates initially. The overall 5 year survival in immunocompetent individuals is approximately 50% from historical data before chemotherapy,29 indicating that long term survival was not significantly better than before the era of chemotherapy. One should be cautious in making direct comparisons as the studied population was not directly comparable with these historical groups. Nevertheless, overall survival was lower than that achieved at a single institution specialising in the management of MDRTB cases in the USA7 and, indeed, falls short of survival for some cancers. This would suggest that the management of MDRTB cases should be in specialised centres with access to an integrated approach including rapid diagnosis of MDRTB, accurate in vitro drug susceptibility data, expert supervision of treatment, drug monitoring, incentives to aid adherence to treatment, and appropriate facilities for case management. Further research is needed to define the best approach to treatment including the clinical role of early second and third line drug susceptibility testing and the range of therapeutic, psychological, and social interventions needed to optimise survival.
Acknowledgments
The help of J Herbert who identified MDRTB cases from the PHLS Mycobnet database, R Williams and P Flanagan, and S Wilson who fingerprinted many of the isolates, is gratefully acknowledged. They, together with J Watson, also provided invaluable advice and support. We would particularly thank all those clinicians, microbiologists, and TB nurses who helped with this study.
REFERENCES
Footnotes
-
The study was designed by F Drobniewski who, with I Eltringham, was primarily responsible for its execution. The descriptive analysis was performed by F Drobniewski and C Graham and survival analysis was performed by C Graham. F Drobniewski, C Graham, and I Eltringham drafted the paper and all investigators edited and critically reviewed the paper.
-
Funding was provided by the PHLS.
-
Conflicts of interest: none.