Article Text

Abstract
There is increasing evidence that inflammatory mechanisms other than eosinophilic inflammation may be involved in producing the final common pathway of enhanced bronchial reactivity and reversible airflow obstruction that characterises asthma. A review of the literature has shown that, at most, only 50% of asthma cases are attributable to eosinophilic airway inflammation. It is hypothesised that a major proportion of asthma is based on neutrophilic airway inflammation, possibly triggered by environmental exposure to bacterial endotoxin, particulate air pollution, and ozone, as well as viral infections. If there are indeed two (or more) subtypes of asthma, and if non-eosinophilic (neutrophil mediated) asthma is relatively common, this would have major consequences for the treatment and prevention of asthma since most treatment and prevention strategies are now almost entirely focused on allergic/eosinophilic asthma and allergen avoidance measures, respectively. It is therefore important to study the aetiology of asthma further, including the underlying inflammatory profiles.
- asthma
- non-eosinophilic asthma
- sputum induction
- airways inflammation
Statistics from Altmetric.com
The prevalence of asthma is increasing worldwide, but the reasons for the striking increases are unclear.1 The pathophysiological mechanisms involved in the development of asthma are also not completely understood. Asthma is known to involve a heterogeneous airway inflammatory response where many cells play a part.2 In recent decades allergic mechanisms have been closely studied and defined. Consequently, asthma has almost universally been regarded as an atopic disease involving allergen exposure, allergic (IgE mediated) sensitisation with a Th2 CD4+ lymphocyte response and subsequent IL-5 mediated eosinophilic airways inflammation, resulting in enhanced bronchial reactivity3 and eventually in reversible airflow obstruction (asthma).
There is now increasing evidence that other inflammatory mechanisms may be involved in producing the final common pathway of enhanced bronchial reactivity and reversible airflow obstruction that characterises asthma. In a recent systematic review of population based studies we have shown that the proportion of asthma cases that are attributable to atopy is usually less than 50%.4,5 Standardised comparisons across populations or time periods show only a weak and inconsistent association between the prevalence of asthma and the prevalence of atopy.4 A recent comparison of asthma and atopy in 9–11 year old children in Albania and the UK6 is particularly interesting in this regard. Large differences were seen in the prevalence of current wheeze (4.4% and 9.7%, respectively) and exercise induced bronchial reactivity (0.8% and 5.4%) but not in skin prick test positivity (15.0% and 17.8%), suggesting that considerable variations in the prevalence of asthma can occur without differences in the frequency of atopy. Furthermore, treatment with antibodies that neutralise IgE (anti-IgE) are only partially effective in asthma,7–12 adding to the evidence that other inflammatory mechanisms operate in asthma and that the role of IgE may be less important than has often been assumed.13 Several animal studies also support this view and, in addition, question the relative importance of IgE in the pathogenesis of allergic asthma.14–17
Recent studies using sputum induction and/or bronchoalveolar lavage (BAL) techniques to measure and characterise airways inflammation in asthmatic subjects have shown that at least some, and potentially a substantial proportion, of cases have an underlying pathology that is clearly different from that observed in “classic” allergic asthma.18–24 Specifically, patients are observed to have severe and persistent asthma in the absence of eosinophilic inflammation, and may experience an exacerbation of asthma without an increase in eosinophilic inflammation.24 In addition, it is well known that non-allergic asthma is quite common in occupational populations.25 These studies, from a variety of different laboratories, clearly demonstrate the existence of non-eosinophilic asthma. This raises the question as to the role of non-allergic inflammatory mechanisms in the pathophysiology of asthma, and whether these may be involved in a substantial proportion of asthma cases in the general population.
In this review we try to quantify the contribution of non-eosinophilic asthma in the general population, to explore whether non-allergic occupational asthma can be used as a model for this type of asthma in the general population, and discuss potentially relevant exposures and mechanisms that may result in non-eosinophilic asthma.
DEFINITIONS
Atopy
We consider “atopy” as IgE mediated sensitisation to “common allergens” such as house dust mite, pet, and various food allergens. Atopy is usually assessed by skin prick tests or specific serum IgE measures of sensitisation to common allergens. However, a positive test only indicates that a subject is sensitised against a common allergen but does not constitute proof that symptoms experienced by the subject are caused by allergic (IgE) mediated mechanisms.
Asthma
We consider asthma as a heterogeneous chronic inflammatory disorder of the airways involving airflow limitation that is at least partly reversible and which results in recurrent episodes of symptoms such as wheezing, breathlessness, chest tightness, and cough.2 We define eosinophilic asthma as symptomatic airway inflammation characterised by the presence of eosinophils in the airways. Non-eosinophilic asthma then represents symptomatic asthma in the absence of eosinophilic airway inflammation. This definition, based on the underlying pattern of airway inflammation, can now be studied relatively easy using sputum induction techniques.26,27 Eosinophilic inflammation is generally considered to be the main feature of allergic asthmatic airways and is presumed to be crucial in the pathogenesis of allergic asthma.28 In addition to eosinophils, interleukin (IL)-5 and possibly IL-4 play a key role in allergic asthma (IL-5 stimulates the growth, differentiation and activation of the eosinophils, and IL-4 stimulates B cells to IgE production and naïve Th0 cells to differentiate toward a Th2 state), and thus increased levels of IL-5 and IL-4 (in combination with raised eosinophil levels) may be used as other “specific” markers.
PROPORTION OF NON-EOSINOPHILIC ASTHMA IN THE GENERAL POPULATION
Using the classification described above (based on the presence or absence of eosinophils in bronchial biopsy specimens, BAL fluid, or sputum), we have attempted to quantify the proportion of non-eosinophilic asthmatics in the general population. However, previous studies on airways inflammation have been conducted mainly on selected populations—that is, subjects attending asthma clinics, severe asthmatics, atopic asthmatics, asthmatics with bronchial hyperreactivity (BHR), etc—and only a few were conducted in a random sample of asthmatic subjects. These studies therefore give only a crude estimate of the proportion of asthma which is non-eosinophilic in selected populations.
For the purpose of this review we have selected from Medline studies from 1995 onwards with data on eosinophil levels in biopsy specimens, BAL fluid, or sputum of asthmatic subjects where the subjects were not clearly selected on the basis of atopic characteristics (positive skin prick tests or IgE determinations), and where data were presented so that the subjects could be classified as eosinophilic or non-eosinophilic asthmatics. Cut off values used to define eosinophilic and non-eosinophilic asthma were the same as those reported in the original studies (2–4%) or, when the authors did not define a cut off level, we used 2% based on the upper normal limit for eosinophil counts in sputum as previously published.29,30 Table 1 summarises the proportion of asthmatic subjects with eosinophilic inflammation for all eligible studies. The weighed mean proportion of subjects with eosinophilic asthma was 51%, so 49% had non-eosinophilic asthma. Exclusion of infant wheezers19 who may not be truly asthmatic did not significantly change the overall estimate (52% versus 51% eosinophilic asthma).
Proportion of asthmatics with lung eosinophilia
This estimate of the percentage of asthmatics that are “attributable” to eosinophilia is probably an overestimate since non-asthmatic control subjects may have eosinophilia as well, and thus not all asthmatic subjects with eosinophilia necessarily have asthma due to eosinophilia (just as not all asthmatic subjects with atopy have asthma due to atopy4). Only six studies reported findings for non-asthmatic controls. In two studies 20% of the non-asthmatic controls had increased eosinophil levels,19,20 in one 9.4% had increased sputum eosinophil levels,42 and in the other three studies none of the controls had raised sputum eosinophil levels.23,31,35 For the studies with 20% and 9.4% eosinophil positive controls we calculated the population attributable risk (PAR)4 to estimate the true proportion of asthma cases that were attributable to eosinophilia. The PARs for the study by Gibson et al20 were 26% and 51%, respectively, compared with the crude estimates (the proportion of asthmatics with eosinophilia) of 41% for children with current symptoms and 62% for children with BHR. The PAR for another recent study by Gibson et al42 in children with current wheeze was 36% compared with a crude estimate of 45%, while in the study by Marguet et al19 the PAR was 46% compared with a crude estimate of 57% (for children).
This suggests that our estimate of 49% of non-eosinophilic asthma is conservative. On the other hand, the figure of 51% for eosinophilic asthma would be an underestimate (and the figure of 49% for non-eosinophilic asthma would be an overestimate) if a significant proportion of eosinophilic asthmatic subjects did not have eosinophilia at the time they were studied, either because of treatment with corticosteroids or because they had no current symptoms. However, as shown in table 1, the percentage was still relatively low even in asthmatic subjects who were not receiving corticosteroids. Also, the proportion of eosinophilic asthmatic subjects was equally “low” in those with current symptoms (table 1), indicating that this hypothesis was unlikely to account for our findings.
“allergic mechanisms may not be the only and/or the most important underlying mechanism for asthma”
The weighed mean percentage of eosinophilic asthmatics in children was 46% compared with 53% in adults. It is therefore clear that non-eosinophilic asthma is very common both in children and adults. In addition, although it has been speculated that non-eosinophilic inflammation may be a typical characteristic for severe asthma,18,36 the findings in table 1 show that non-eosinophilic asthma is also very common in mild and moderate asthma. Of particular interest is the study by Gibson et al20 in 56 asthmatic children who had experienced symptoms in the previous 2 weeks, since this is a study in a random population of asthmatics. The estimate of 41% (with a PAR of “only” 26%) suggests that approximately 60% (or more) of all asthma cases in children could be attributable to non-allergic or non-eosinophilic mechanisms. This was confirmed in another random population study conducted by the same group.42 Restricting the population to only those children with BHR resulted in an increase in the proportion of eosinophil positive asthmatics to 62% (PAR 51%),20 suggesting that BHR is associated with eosinophilic asthma but less so with non-eosinophilic asthma. This has also been shown previously by others.24
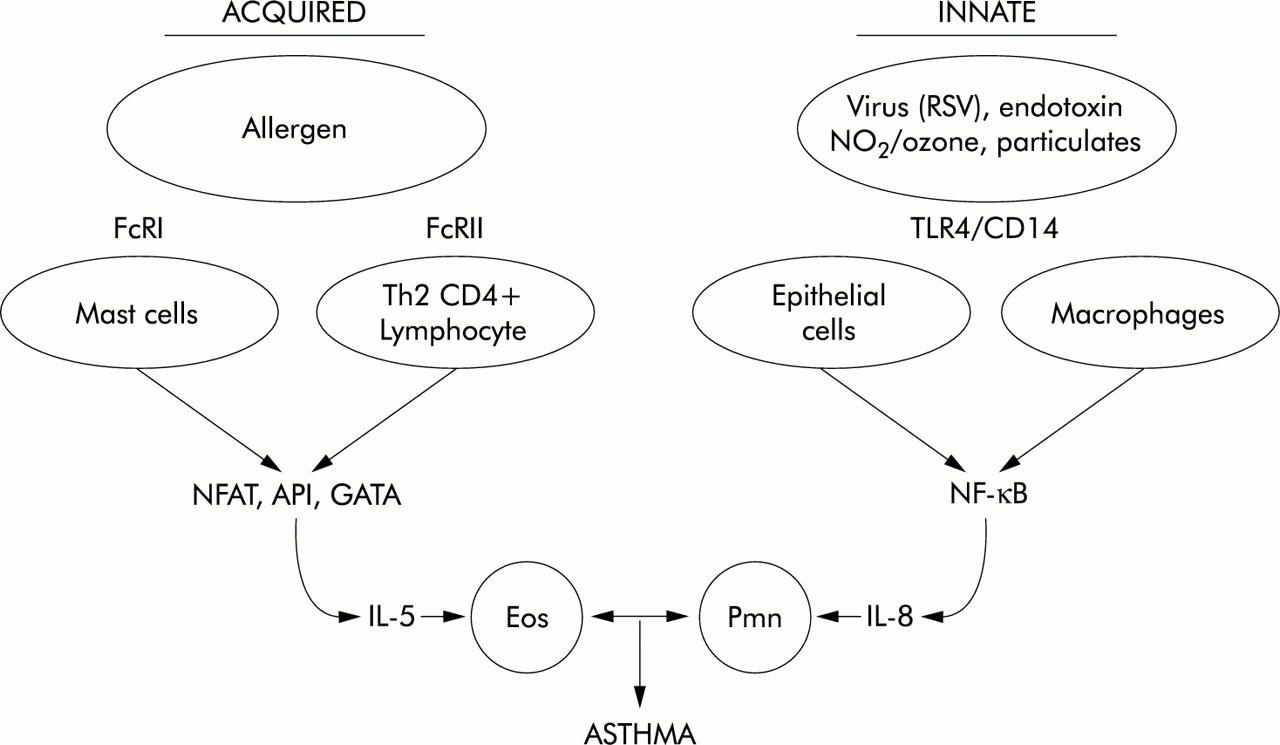
It is striking that in most studies non-eosinophilic asthma was associated with increased neutrophil and IL-8 levels,18,19,21,36,43,44 which suggests that non-allergic neutrophil driven airways inflammation was the underlying mechanism for non-eosinophilic asthma. Interestingly, the inflammatory profile appears to be very similar to that described for non-eosinophilic occupational asthma (see below), and is consistent with activation of innate immune mechanisms mediating the inflammatory process in non-eosinophilic asthma (fig 1).
{kind=link}
Acquired and innate immune pathways leading to IL-5 mediated eosinophil (Eos) inflammation (acquired pathway) or IL-8 mediated neutrophil (Pmn) inflammation (innate pathway) and subsequent asthma. Receptors for triggers (FcRI, FcRII, TLR4, CD14) and transcription factors (NFAT, API, GATA, NF-κB) are shown as intermediate steps.
NON-ALLERGIC OCCUPATIONAL ASTHMA
Our focus in this review is on asthma in the general population, but it is interesting also specifically to consider studies of occupational asthma since these provide further evidence of the importance of non-allergic mechanisms for asthma and suggest what these mechanisms may be. In occupational medicine it has long been recognised that a substantial proportion of work related asthma is non-allergic. One type of non-allergic asthma frequently referred to as “asthma like disorder or syndrome” or “irritant induced asthma”25,45 may be a useful model for non-allergic asthma in the general population, since it is relatively common in occupational populations and causal exposures are diverse and are often present also in the general environment. It is highly prevalent in farmers and those in farm related occupations, but also in many other occupations with exposures to bio-aerosols containing microbial agents.45 Although some prefer the term “asthma like syndrome”, it meets the clinical criteria of asthma—that is, reversible airways obstruction. However, in contrast to allergic asthma, previously unexposed subjects can develop symptoms and (reversible) airflow obstruction without any prior sensitisation or latency period,46,47 and the underlying inflammation is one in which neutrophils rather than eosinophils dominate.48,49 Thus, both atopic and non-atopic subjects may develop non-eosinophilic asthma, although atopic subjects may be more sensitive.50 Moreover, non-allergic occupational asthma is not clearly related to non-specific bronchial hyperresponsiveness,51 although a transient increase in BHR may be apparent.46
Although the exact pathophysiology is not clear, it is well established that non-allergic occupational asthma is mediated by an acute inflammatory response involving a number of cytokines, including IL-1, IL-6, IL-8, and tumour necrosis factor (TNF)-α, and the subsequent massive infiltration and activation of neutrophils in the lower and upper airways52–54 which is very similar to the inflammatory response observed in non-eosinophilic asthma in the general population (see above). The primary agent inducing these inflammatory responses in workers exposed to organic dust is believed to be bacterial endotoxin. Macrophages carry specific endotoxin binding receptors (CD14, TLR4) that play a crucial role in the activation of these cells and the subsequent inflammatory reactions.55,56
RELEVANT EXPOSURES
Which exposures may contribute to the development of non-eosinophilic asthma in the general population? Several non-allergenic exposures such as bacterial endotoxins, particulate air pollution, and ozone which are commonly present in the environment have been shown, both in experimental and epidemiological studies, to induce neutrophilic airway inflammation, airway obstruction, and symptoms of asthma.57–67 Endotoxin, a strong proinflammatory cell wall component from Gram negative bacteria,56 has been recognised as an important factor in the aetiology of occupational lung diseases including non-allergic asthma.45,57 In addition, it has been shown that endotoxin in house dust is associated with exacerbations of pre-existing asthma in children and adults.68–71 Finally, one recent birth cohort study in 499 infants with a familial predisposition to asthma or allergy reported that early exposure to indoor endotoxin was associated with an increased risk of repeated wheeze during the first year of life (RR=1.6, 95% CI 1.03 to 2.38).72 Thus, despite a recent hypothesis that exposure to endotoxin early in life may have a protective effect on the development of atopy and thus potentially also on allergic asthma by enhancing Th1 immunity,73–76 a role for endotoxin as a risk factor for non-allergic asthma cannot be excluded; in fact, it seems likely.77
Ozone is a powerful oxidant and air pollutant that has been shown to exacerbate pre-existing asthma,78–83 but some evidence from large epidemiological studies has been presented that suggests a role for ozone also in the primary causation of asthma.84–86 Similarly, particulates such as diesel exhaust increase asthma symptoms, induce neutrophilic airways inflammation,64 and promote neutrophil mobilisation from the bone marrow.65 These responses are most probably mediated by NF-κB activation and IL-8 secretion.87 Thus ozone, particulates, and endotoxin have the potential to induce asthma by non-allergic mechanisms and, while they are commonly present in increased concentrations in the environment, they may contribute to the development of non-eosinophilic asthma in the general population.
In addition, viral infections may induce non-eosinophilic asthma. Viral respiratory tract infections are the most common cause of significant asthma exacerbations in children88 and adults.89 As for endotoxin, particulates, and ozone, viral infection of respiratory epithelial surfaces promotes a vigorous chemokine response with increased IL-8 secretion that is believed to be responsible for the typical neutrophil inflammation in viral induced asthma.90
ROLE OF INNATE IMMUNE ACTIVATION
The common pathophysiological features of non-eosinophilic asthma involve an IL-8 mediated neutrophil influx and the subsequent neutrophil activation is a potent stimulus to increased airway hyperresponsiveness.91 Although the stimuli that trigger this response are diverse (endotoxin, ozone, particulates, virus infection), the common features are consistent with activation of innate immune mechanisms rather than IgE mediated activation of acquired immunity. Recent data indicate a role for Toll-like receptors (TLR) and CD14 in this process.92 TLRs can recognise a large variety of chemically diverse stimuli which then trigger proinflammatory responses involving NF-κB activation and chemokine production93,94 characteristic of non-eosinophilic asthma (fig 1).
There is also the potential for combined activation of both innate and allergen specific inflammatory mechanisms to occur in asthma. This could result in a mixed eosinophil/neutrophil response as has been observed in some cases of acute asthma,41 and may explain the ability of ozone and NO2 to potentiate allergen induced asthmatic responses.95
CONCLUSIONS
We have previously shown that atopic mechanisms may account for, at most, “only” 40% of cases of asthma in the general population.4 Interestingly, in this review we have shown that, at most, “only” 50% of all asthma cases are attributable to eosinophilic airway inflammation. Thus, evidence from studies of eosinophilia and asthma is consistent with that from studies of atopy and asthma: in both instances, at most about 50% of asthma cases appear to be due to “allergic” mechanisms (whether these are defined in terms of atopy or in terms of eosinophilia). This further adds to the evidence that allergic mechanisms may not be the only and/or necessarily the most important underlying mechanism for asthma. Non-eosinophilic asthma is associated with neutrophilic responses not only in severe asthmatics but also in those with moderate and mild asthma, and we thus hypothesise that a major proportion of asthma is based on neutrophilic airway inflammation. Environmental exposure to bacterial endotoxin, particulate air pollution, and ozone, as well as viral infections, may play an important role as triggers of neutrophilic airway inflammation in asthma.
The inflammatory picture in surveys of the general population appears to be very similar to that observed in non-allergic asthma in occupational populations which thus may serve as a suitable model for non-allergic asthma in the general population. It is not clear whether neutrophilia develops as a primary pathological process (as is the case in occupational non-allergic asthma) or is secondary to high doses of inhaled corticosteroids (ICS) that are known to prolong the survival of neutrophils96 and to reduce eosinophil survival.97 One study38 seems to confirm the latter hypothesis to a certain extent; after cessation of treatment with ICS the percentage of eosinophils increased significantly in seven of 20 subjects with recurrent symptoms but only marginally in the 13 subjects without recurrence of asthma symptoms (not significant). Furthermore, two studies31,37 indicated a lower proportion of eosinophilic asthmatic subjects in those receiving ICS. However, in these two studies the prevalence was still relatively low even in those who did not receive treatment with ICS (67% and 29%, respectively). In addition, in the study by Gibson et al20 only six of the 56 asthmatic children were on ICS but the percentage of eosinophilic asthma was “only” 41%. In the study by Ottanelli et al39 no difference was seen in the mean proportion of eosinophils in the obstructed ICS naïve and ICS treated asthma patients. Finally, several other studies24,43 showed that corticosteroid treatment was unlikely to explain the differences in inflammatory responses since no difference in treatment existed between the groups with and without increased bronchial eosinophilic cells. However, regardless of the exact mechanisms involved, neutrophils appear to be important in the pathophysiology of asthma, both in occupational populations and in the general population. The features suggest a common mechanism involving activation of innate immune responses in the generation of chemokine release and neutrophil influx.
Our focus has been on assessing the relative importance of non-eosinophilic mechanisms for asthma and on the need for more research into what these mechanisms may be. Nevertheless, on the basis of current evidence it is tempting to speculate that most non-eosinophilic asthma is neutrophil mediated, in contrast to allergic asthma which is eosinophil mediated. If there are indeed two (or more) subtypes of asthma as hypothesised, and if non-eosinophilic (neutrophil mediated) asthma is relatively common, this would have major consequences for the treatment and prevention of asthma since most treatment and prevention strategies are now almost entirely focused on allergic/eosinophilic asthma and allergen avoidance measures, respectively. It is therefore important to study the aetiology of asthma further, including the underlying inflammatory profiles. Furthermore, since little is known about the prognosis of both types of asthma, future studies need prospective evaluation. A better understanding of the underlying mechanisms will also provide a firmer basis for new theories to explain why there is a world wide increase in asthma, and would provide new insights into which factors determine primary causation of asthma. The current “hygiene hypothesis”, which is based on the assumption that a lack of certain exposures early in life (for example, infections) may enhance Th2 or atopic immune responses,74 can potentially only explain an increase in allergic but not of non-allergic asthma. Thus, with the large proportion of non-allergic asthma it is questionable whether the “hygiene hypothesis” (as defined above) on its own can explain the large increase observed over the last decades.
Acknowledgments
The Centre for Public Health Research is funded by the Health Research Council of New Zealand. Jeroen Douwes is supported by a research fellowship from the Netherlands Organization for Scientific Research (NWO).