Article Text

Abstract
Background: Cysteinyl leukotrienes (cysteinyl-LTs) have been implicated in the pathogenesis of allergen induced airway responses. Airway responsiveness (AR) to inhaled cysteinyl-LTs is dramatically increased following allergen challenge in animal studies. The effect in man has not been evaluated.
Methods: Ten mild steroid-naïve asthmatic subjects with an isolated early asthmatic response (EAR) and 21 with an additional late asthmatic response (LAR) took part in a randomised controlled crossover study to assess AR to inhaled methacholine (MCh) and cysteinyl-LT D4 (LTD4) 22 and 24 hours, respectively, after allergen challenge. Eight subjects had two further LTD4 challenges separated by a 2 week washout period to assess the reproducibility of inhaled LTD4 challenge.
Results: In subjects with an isolated EAR, non-significant mean (SE) increases in AR of 0.4 (0.4) doubling doses (DD) for MCh and 0.4 (0.5) DD for LTD4 followed allergen challenge compared with control. A significant correlation between AR to MCh and LTD4 followed both control (r=0.91, 95% CI 0.67 to 0.98; p=0.0002) and allergen challenge (r=0.79, 95% CI 0.32 to 0.95; p=0.0063). In subjects with an additional LAR there was a significant increase in AR to MCh (1.2 (0.3) DD, p=0.0005) following allergen challenge but no overall effect on AR to LTD4 (0.69 (0.4) DD, p=0.11). A significant correlation between AR to MCh and LTD4 was again observed (r=0.70; 95% CI 0.38 to 0.87; p=0.0004) following control, although it was reduced following allergen challenge (r=0.48; 95% CI 0.063 to 0.76; p=0.027). LTD4 challenge was highly reproducible with a mean difference of 0.2 (0.3) DD between challenges.
Conclusions: Allergen challenge significantly increases AR to inhaled MCh but not to LTD4 in subjects with LAR. The lack of a comparable increase in AR to LTD4 is surprising. Endogenous cysteinyl-LTs are produced in abundance following allergen challenge and may enhance AR to MCh or induce a degree of tachyphylaxis to LTD4.
- asthma
- methacholine
- LTD4
- allergen challenge
- airway responsiveness
Statistics from Altmetric.com
Airway inflammation plays a central role in the pathogenesis of asthma and is associated with an increase in airway responsiveness (AR) to various spasmogens. Allergen challenge has proved a useful and reproducible clinical model of asthma to study inflammatory mechanisms and assess the efficacy, pharmacological, and anti-inflammatory properties of therapeutic agents.1
Inhalation of allergen by sensitised subjects results in an early asthmatic response (EAR) within 30 minutes which generally resolves within 1–3 hours. This is characterised by airway mast cell activation, release of histamine, cysteinyl leukotrienes (cysteinyl-LTs) and reactive oxygen species with subsequent airway bronchoconstriction, increased microvascular permeability, and mucus secretion.2,3 A more prolonged late asthmatic response (LAR) occurs in more than 50% of these subjects 3–10 hours after allergen inhalation, secondary to both bronchoconstriction and recruitment and activation of airway inflammatory cells.4,5 This is often associated with a 1–3 “doubling dose” increase in AR to the “direct” acting smooth muscle spasmogens methacholine (MCh) and histamine and the “indirect” spasmogen adenosine 5`-monophosphate (AMP).6,7 Persistence varies according to test spasmogen—<24 hours for AMP and 1–7 days for MCh and histamine—while bradykinin shows large protracted changes in sensitivity of up to 3–5 doubling doses over 2 weeks.8 Although not previously studied in man, dramatic increases in responsiveness to the cysteinyl-LTs have been shown following allergen challenge in guinea pigs.9
It is generally accepted that the cysteinyl-LTs are important in allergen induced early asthmatic responses with increased levels detected in bronchoalveolar lavage (BAL) fluid and urine.3,10 Increased cysteinyl-LT levels during the LAR and attenuation of the LAR as well as the EAR following cysteinyl-LT antagonist therapy also provides support for their involvement in the LAR.11,12 The more potent second generation cysteinyl-LT antagonists also attenuate allergen induced increases in AR.13
In view of the efficacy of cysteinyl-LT antagonist therapy in attenuating allergen induced responses and the heterogeneity of increased AR, the aim of this study was to evaluate the effect of allergen challenge on AR to the cysteinyl-LTs in man. AR to inhaled cysteinyl-LT D4 (LTD4) and MCh was measured before and after an acute allergic reaction. Reproducibility of the inhaled LTD4 challenge was also assessed in a randomly selected subgroup of subjects.
METHODS
Study subjects
Thirty one non-smoking subjects (22 men) aged 18–35 years took part in the study. All subjects had mild asthma (forced expiratory volume in 1 second (FEV1) ≥70% predicted) and a positive skin prick test to common airborne allergens (Dermatophagoides pteronyssinus, mixed grass pollen, or cat) and a documented sensitivity to MCh (concentration provoking a fall in FEV1 of 20% or more (PC20) <8 mg/ml) during the previous 4 weeks. None had an exacerbation of asthma or respiratory infection in the preceding 6 weeks. Each subject had infrequent symptoms, controlled with occasional inhaled short acting β2 agonists alone. No subject was taking any regular anti-asthma therapy and none had taken inhaled corticosteroids for at least 3 months prior to entry. Written informed consent was obtained from each subject and the study was approved by the ethics committee of King's College Hospital.
Study design
Subjects were randomised into a controlled crossover study with a 3–4 week washout period. Following baseline spirometric tests, each subject had either an allergen inhalation challenge according to skin prick testing or a control challenge. The control challenge consisted of two “prolonged” MCh challenges 6 hours apart with no bronchodilator relief between challenges or for 4 hours after the second challenge. This was designed to mimic the early and late bronchoconstrictive response following allergen challenge. MCh followed by LTD4 challenges were carried out, in that order, 22 and 24 hours, respectively, after both allergen and control challenges, provided FEV1 was within 10% of baseline.
After a washout period of at least 4 weeks from the main study, eight subjects went on to have two further LTD4 challenges with a 2 week washout period in between to assess LTD4 challenge reproducibility. These challenges were carried out at the same time of day.
All subjects refrained from using rescue medication and caffeinated beverages for at least 8 hours before each visit and challenge and attended the laboratory at the same time each morning
Bronchial provocation and lung function measurement
“Standard” methacholine challenge
Fresh solutions of MCh (Northwick Park and St Marks Hospitals, Harrow, UK) were made up in 0.9% saline in concentrations from 0.0625 to 32 mg/ml. Each solution was administered from a nebuliser attached to a breath activated dosimeter (Mefar, Brescia, Italy). The nebuliser delivered particles with an aerodynamic mass median diameter of 3.5–4 μm at a mean output of 12 μl per breath.
Pulmonary function was assessed by measurement of FEV1 using a dry wedge spirometer (Vitalograph, Buckingham, UK). A standard challenge protocol was used for all provocation tests. Following a 15 minute rest period, subjects performed three measurements of FEV1 1 minute apart, the best of which was taken as baseline. Subjects then inhaled five breaths of saline as control with an inhalation time of 1 second and breath hold time of 6 seconds. Provided FEV1 remained within 10% of baseline, subjects continued by inhaling five breaths of doubling concentrations of MCh at 3 minute intervals. FEV1 was measured at 1.5 and 2.5 minute intervals following each concentration and the highest value recorded for analysis. Challenges were terminated when a fall in FEV1 of at least 20% from the post-saline value was recorded or the maximum concentration had been given. A logarithmic concentration-response curve was constructed and the PC20 calculated by linear interpolation.
LTD4 challenge
LTD4 was purchased at a concentration of 10 mg/ml in ethanol (Cascade Biochem Ltd, Reading, UK), diluted in phosphate buffered saline (PBS), and stored in 2 ml aliquots of 100 μg/ml in amber glass vials under argon at –70°C. Within 2 hours of use, twofold dilutions of this stock solution were prepared ranging from 100 μg/ml to 0.0244 μg/ml (200 μM to 48.8 nM). Dilutions were kept under argon and only opened for immediate use. The same protocol as for the standard MCh challenge was used except subjects inhaled five breaths of doubling concentrations of LTD4 at 7 minute intervals with FEV1 measured at 5 and 6 minute intervals.
“Prolonged” methacholine (control) challenge
The same protocol as for the standard MCh challenge was used except subjects inhaled five breaths of doubling concentrations of MCh at 7 minute intervals with FEV1 measured at 5 and 6 minute intervals. The challenges were terminated when a fall in FEV1 of at least 30% was recorded.
Allergen challenge
Allergen for skin prick tests (Soluprick SQ, Alk Abelló (UK) Ltd) was stored at 4°C; each subject was assessed for sensitivity to house dust mite, cat, grass pollen, and positive and negative controls. The allergen for inhalation was selected according to the largest skin test wheal (positive >3 mm) and clinical history. Fresh solutions of allergen (Aquagen SQ, Alk Abelló (UK) Ltd) were made up in 0.9% saline in doubling concentrations from 250 SQ-U/ml to 32 000 SQ-U/ml. Subjects inhaled five breaths of saline as control followed by five breaths of the lowest concentration of allergen. Each solution was administered under the same conditions from a nebuliser attached to a breath activated dosimeter as above. FEV1 was measured at 5 and 10 minutes after inhalation and the lowest value recorded for analysis. If the fall in FEV1 was <10% of the post-saline value, a further five breaths of a quadruple concentration of allergen was inhaled. If a 10–15% fall in FEV1 was achieved, a further five breaths of a double concentration was inhaled. Challenges were terminated when a fall in FEV1 of at least 15% from the post-saline value was recorded or the maximum concentration had been given. FEV1 was then measured at 20, 30, 45 and 60 minutes and every 30 minutes thereafter for a total of 10 hours after the challenge. An early asthmatic response (EAR) was defined as a fall in FEV1 of >20% within the first 2 hours and late asthmatic response (LAR) as a fall in FEV1 of >15% 4–10 hours after allergen on three separate occasions.
Analysis of data
Results are expressed as mean (SE) values unless otherwise stated. PC20 values on each study day were logarithmically transformed and the two tailed Student's t test for paired observations was used to evaluate differences in AR for each spasmogen following allergen, control, and LTD4 reproducibility challenges. The change in PC20 is also expressed as mean (SE) doubling doses (DD). The two tailed Pearson correlation test was used to compare AR to MCh and LTD4 following both allergen and control challenges. The Pearson correlation coefficient, r, and two sided 95% confidence intervals (CI) are given. Relative potency of inhaled LTD4 to MCh was evaluated following μmol conversion of geometric mean PC20 results. Statistical analysis was performed using Graphpad Prism version 3.0. Statistical significance was taken as p<0.05.
RESULTS
All subjects completed the study. According to our criteria, 21 subjects were defined as having a dual asthmatic response—that is, an EAR followed by an LAR—with a fall in FEV1 of ≥15% on three separate occasions 4–10 hours after allergen challenge. Ten subjects were defined as having an isolated EAR to inhaled allergen. The mean cumulative dose of allergen required to achieve the initial 15% fall in FEV1 was higher for subjects who had an isolated EAR than in those who also had an LAR (table 1).
Individual and mean baseline characteristics and allergen challenge responses
There was no difference in baseline characteristics in subjects with an isolated EAR and those with an additional LAR, and no significant difference in airway responsiveness to MCh (PC20) at screening and 22 hours after control challenges in subjects with either an isolated EAR or LAR.
Isolated early asthmatic responders
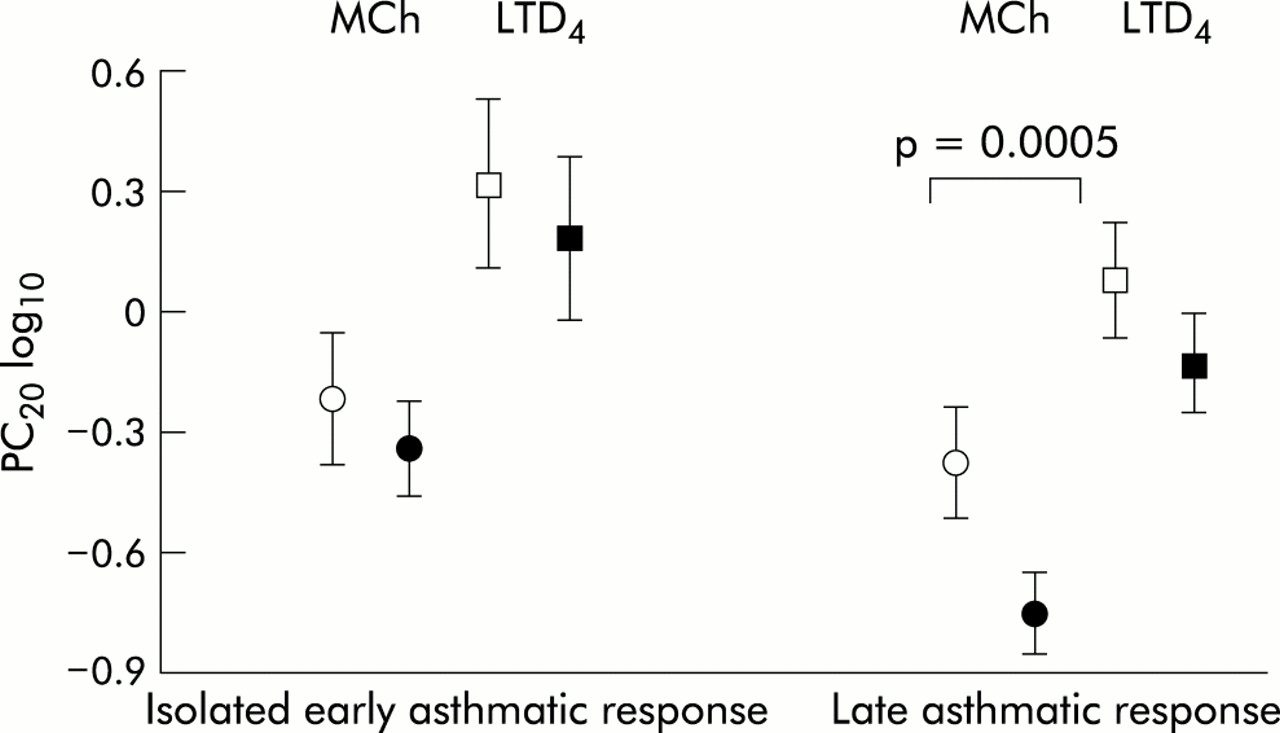
The mean PC20 following control and allergen challenges in subjects with an isolated EAR was 0.61 and 0.46 mg/ml, respectively for MCh and 2.09 and 1.54 μg/ml for LTD4 (geometric mean (SE) log PC20 shown in fig 1). These differences are equivalent to a non-significant increase in AR following allergen challenge of 0.4 (0.4) doubling doses (DD) for MCh and 0.4 (0.5) DD for LTD4 (fig 2).
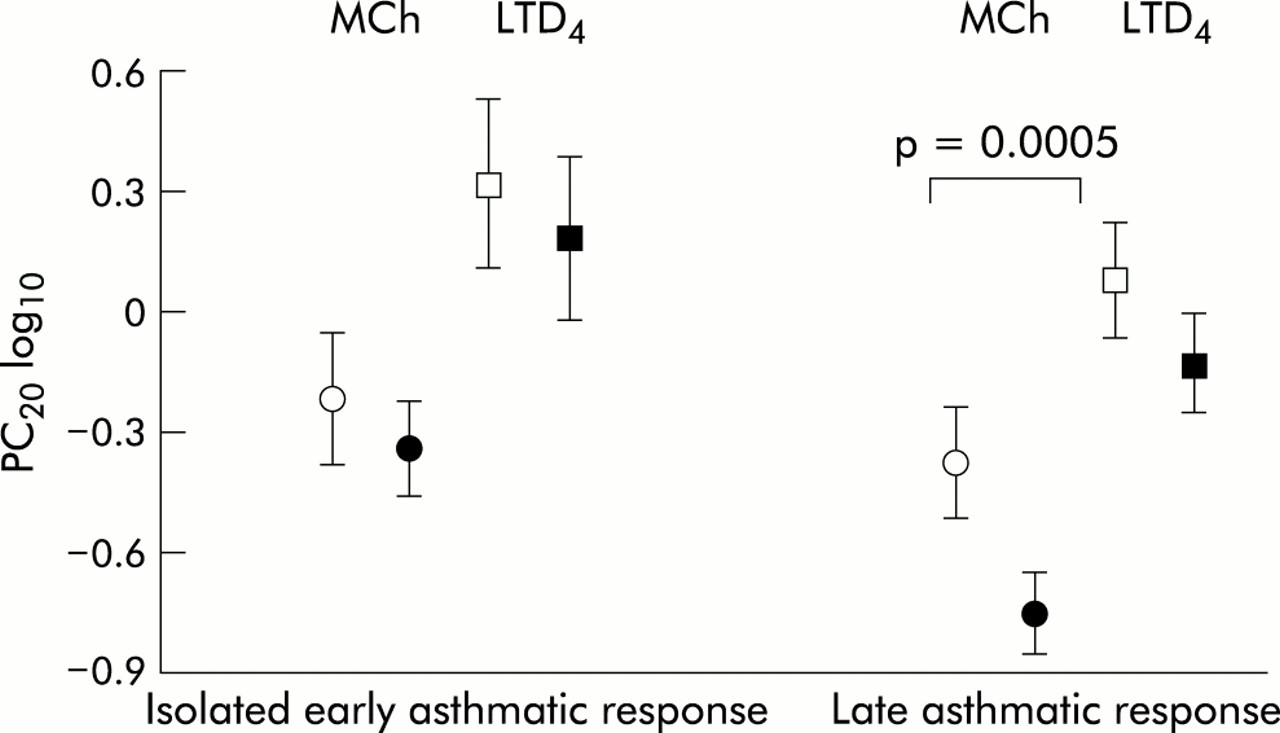
Airway responsiveness to methacholine (MCh) and leukotriene D4 (LTD4) in subjects with an isolated early asthmatic response and subjects with an additional late asthmatic response following control (open symbols) and allergen challenge (closed symbols). There was no significant change in airway responsiveness to either MCh or LTD4 in subjects with an isolated early asthmatic response, but a significant increase in airway responsiveness was observed to MCh but not to LTD4 in subjects with a late asthmatic response (p=0.0005).

Individual and mean doubling dose change in airway responsiveness to methacholine (MCh) and leukotriene D4 (LTD4) in subjects with an isolated early asthmatic response and subjects with an additional late asthmatic response following allergen challenge compared with control.
There was a significant correlation between AR to MCh and LTD4 following both control (r=0.91; 95% CI 0.67 to 0.98; p=0.0002) and allergen challenge (r=0.79; 95% CI 0.32 to 0.95; p=0.0063; fig 3).

Pearson correlations between airway responsiveness to leukotriene D4 (LTD4) and methacholine (MCh) in (A) subjects with an isolated early asthmatic response and (B) those with an additional late asthmatic response following control (open symbols) and allergen (closed symbols) challenges.
On a μmol to μmol basis, there was no change in the relative potency of LTD4 to MCh following allergen challenge in subjects with an isolated EAR. LTD4 was 735 times more potent than MCh at inducing bronchoconstriction following the control challenge and 755 times more potent following allergen challenge. There was no linear relationship between AR to MCh and the relative potency of LTD4 when compared with MCh (as indicated by the dose ratio of MCh to LTD4) following either control (r=–0.34, p=0.33) or following allergen (r=–0.34, p=0.34).
Dual asthmatic responders
The mean PC20 following control and allergen challenges in LAR subjects was 0.43 mg/ml and 0.18 mg/ml, respectively, for MCh and 1.2 μg/ml and 0.75 μg/ml for LTD4 (geometric mean (SE) log PC20 shown in fig 1). These differences are equivalent to a significant increase in AR to MCh of 1.2 (0.3) DD, p=0.0005, in contrast to a non-significant increase in AR to LTD4 of 0.69 (0.4) DD, p=0.11, following allergen challenge (fig 2).
There was a significant correlation between AR to MCh and LTD4 following control (r=0.70; 95% CI 0.38 to 0.87; p=0.0004) which was reduced but remained significant following allergen challenge (r=0.48; 95% CI 0.063 to 0.76; p=0.027; fig 3).
There was a fall in the relative potency of LTD4 to MCh following allergen challenge in LAR subjects with LTD4 890 times more potent than MCh following the control and 605 times more potent following allergen challenge. There was no linear relationship between AR to MCh and the relative potency of LTD4 when compared with MCh (as indicated by the dose ratio of MCh to LTD4) following control in either subjects with an LAR (r=0.34, p=0.14) or the study group as a whole (r=0.2, p=0.27). There was a tendency to such a relationship following allergen challenge but this did not reach statistical significance (r=0.38, p=0.09; fig 4).
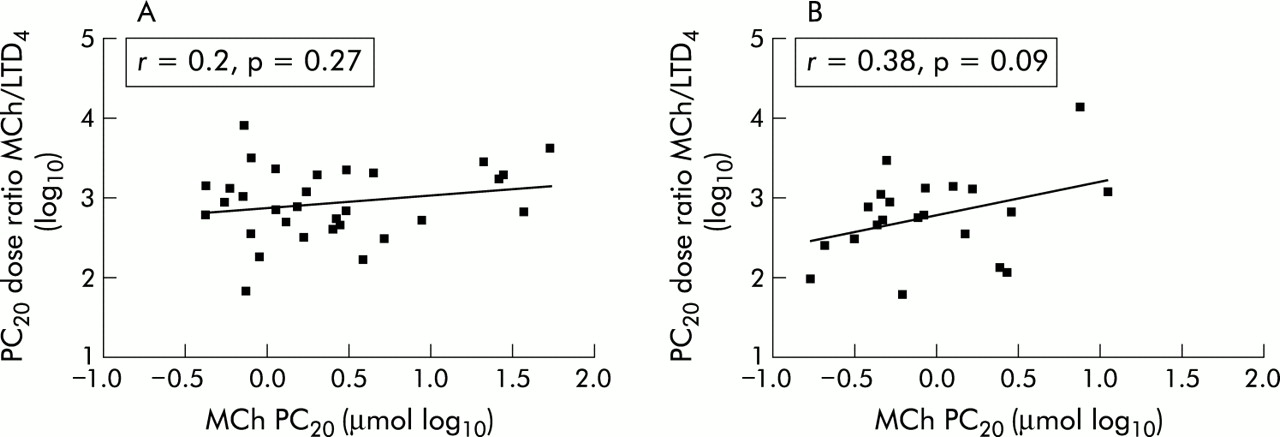
Relationship between airway responsiveness to MCh (PC20 μmol) and the relative potency of LTD4 as measured by the PC20 dose ratio of MCh to LTD4 in (A) all subjects following control and (B) in subjects with a late asthmatic response following allergen challenge.
LTD4 reproducibility
A high degree of reproducibility was seen in LTD4 sensitivity with a mean LTD4 PC20 on the two study days of 0.89 μg/ml and 1.02 μg/ml, equivalent to a difference of 0.2 (0.3) DD (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
LTD4 reproducibility in eight subjects. Standard LTD4 provocation challenge on two separate study days at least 2 weeks apart. Individual LTD4PC20 (log10) (open circles) and geometric mean (SE) (closed circles). There was a non-significant difference in airway responsiveness to LTD4 of 0.2 (0.3) doubling doses between visits.
DISCUSSION
This is the first study to show the differential effect of allergen challenge on AR to inhaled MCh and LTD4 in subjects with a dual asthmatic response. A significant increase in AR to MCh was observed 22 hours after allergen challenge. In contrast, no change in LTD4 responsiveness was observed at 24 hours. There was no change in AR to either spasmogen in subjects with an isolated EAR.
Augmentation of underlying AR to the “direct acting” smooth muscle spasmogens such as MCh and histamine is associated with an allergen induced LAR.6 This follows airway recruitment and activation of eosinophils, metachromatic cells, and CD4+ T lymphocytes with consequent cytokine and chemokine release and associated disruption of airway epithelium.14,15
In comparing AR to each spasmogen following the control challenge, we have confirmed that inhaled LTD4 is almost 1000 times more potent than inhaled MCh at inducing bronchoconstriction in subjects with an LAR. As cysteinyl-LTs also have a “direct” smooth muscle action, we may have expected an increase in AR to inhaled LTD4 following the LAR.
The dissociation in response to inhaled LTD4 and MCh after the LAR is surprising and warrants further explanation. The mechanisms underlying increased AR following allergen challenge are not fully understood and are likely to be complex in nature.4,5 It is possible that generation of cysteinyl-LTs following allergen challenge may lead to an increase in AR to Mch,16,17 but it could also lead to desensitisation of cysteinyl-LT receptors on airway smooth muscle. A reduction in the potency of LTD4 relative to MCh may therefore suggest partial tachyphylaxis to LTD4. Tachyphylaxis to the effects of LTD4 has been reported following repeated inhaled LTD4 challenges.17,18
As previously shown, we found a highly significant linear correlation between AR to MCh and LTD4 following control challenge.19–21 This relationship is somewhat reduced but remains significant in subjects with an LAR following allergen challenge (fig 3). In many ways our data on AR following allergen challenge resembles the original findings of Adelroth et al20 who showed that subjects with increased AR to MCh had least sensitivity to LTD4. Like Adelroth et al, we also examined the relationship between AR to MCh and the relative potency of LTD4 compared with MCh as indicated by the dose ratio of MCh to LTD4 (fig 4). For our study subjects there was no linear relationship before the allergen challenge. Following allergen, subjects with an LAR showed a tendency for such a relationship. The results of our study therefore lend some support to the original observation of Adelroth who studied a more heterogenous group including normal volunteers. Generation of cysteinyl-LTs during the LAR is only one possible explanation for our results, and this remains speculative as we are unable to determine the mechanism based on the current data.
Cysteinyl-LT levels are increased in both urine and BAL fluid during the EAR,3,11 but there has been debate as to their involvement in the LAR with some studies unable to detect any change in cysteinyl-LT levels.10,22 However, recruited and activated eosinophils and metachromatic cells are a likely source of continued cysteinyl-LT production and more recent reports have shown increased urinary levels during the LAR.11,23 Sputum eosinophilia has also been shown to correlate with increased sputum cysteinyl-LT levels in subjects with an LAR.24
In contrast to the effect on AR to MCh, histamine, and bradykinin, there is no effect on AR to the “indirect” acting spasmogen AMP 24 hours after allergen challenge.7,8 As adenosine induces mast cells to release cysteinyl-LTs, tachyphylaxis to inhaled AMP at 24 hours may result from both endogenously produced adenosine and cysteinyl-LTs during the LAR and is consistent with our findings.25
We chose to perform MCh and LTD4 challenges at 22 and 24 hours after allergen challenge, respectively. The LTD4 challenge always followed the MCh challenge. This may have been a confounding factor in the study design, as it is possible that prior bronchoconstriction with MCh could have altered the AR to LTD4. However, in contrast to the effect of cysteinyl-LT inhalation, several published studies have shown that provoked bronchoconstriction with the “direct” spasmogens MCh and histamine does not alter AR16,17,26,27 and does not induce airway inflammation.28–30 We could not have performed the LTD4 challenge first as the acute effects of cysteinyl-LT inhalation on AR and airway inflammation are clearly documented.16,17,26,27,30
Bronchoconstriction per se cannot explain the differences in AR following the LAR. All subjects underwent biphasic bronchoconstriction with inhaled MCh to a ≥30% fall in FEV1 to mimic the dual asthmatic response before control MCh and LTD4 challenges the following day. We were also careful to minimise the effect of altered airway calibre on AR by ensuring that FEV1 had recovered to within 10% of the baseline value before each challenge. There were no differences in baseline characteristics between those subjects with an isolated EAR and those with an additional LAR. However, subjects achieving a dual asthmatic response required on average <50% of the cumulative dose of inhaled allergen to achieve the initial 15% fall in FEV1 compared with EAR subjects, despite both achieving equivalent maximal falls in FEV1 within the first hour (table 1). This would imply that dual asthmatic responders are more likely to have “twitchy” airways than those with an isolated EAR.
Although there was no overall statistical change in AR to LTD4 following the LAR, a surprisingly disparate range of individual responses was observed. Five of the 21 subjects had a dramatic increase in AR of 3–5 DD while the remainder had either a decrease or minimal change (fig 2). Subject numbers are too small to make any conclusions on the distribution of this response. However, as the eight subjects who underwent repeat inhaled LTD4 challenges had a geometric mean difference of 0.2 DD between visits (fig 5), poor reproducibility is unlikely to explain our results. It is interesting to speculate whether phenotypically similar asthmatic subjects show heterogeneity in endogenous cysteinyl-LT production and therefore tachyphylaxis at the cysteinyl-LT receptor following allergen challenge. This could explain the range of individual responses in our study and the conflicting reports on cysteinyl-LT production during the LAR, especially in studies which have only evaluated mean responses in small numbers of subjects.10,11,22,23 Whether or not anti-leukotrienes are more effective in asthmatic subjects with a greater propensity to produce endogenous cysteinyl-LTs and thereby demonstrate tachyphylaxis remains to be determined.
This study shows that allergen challenge has a differential effect on AR to inhaled LTD4 and MCh in subjects with an LAR. Generation of endogenous cysteinyl-LTs following allergen exposure may account for our results, either by increasing AR to MCh or by inducing partial tachyphylaxis to inhaled LTD4. The mechanisms underlying the LAR are likely to be multifactorial in nature and there is no clearcut explanation for our observations. Further study of the heterogeneity of AR following allergen challenge is required.