Article Text

Abstract
BACKGROUND A systematic literature review was conducted to assess the effect of treating reflux oesophagitis on asthma outcomes.
METHODS Randomised controlled trials of reflux oesophagitis treatment in adults or children that reported asthma health outcomes were included and assessed in accordance with the standard Cochrane systematic review process. Patients were typically adults with asthma and concurrent symptomatic gastro-oesophageal reflux who received interventions that included pharmacological therapy, conservative management, and surgery. The following outcome measures were assessed: lung function, peak expiratory flow, asthma symptoms, asthma medications, and nocturnal asthma.
RESULTS From 22 potentially relevant published and unpublished randomised controlled trials, 12 were included. Treatment duration ranged from 1 week to 6 months. Eight trials reported that treatment improved at least one asthma outcome, but these outcomes differed between trials. Overall, treatment of reflux oesophagitis did not consistently improve forced expiratory volume in one second (FEV1), peak expiratory flow rate, asthma symptoms, nocturnal asthma symptoms, or use of asthma medications in asthmatic subjects. Significant improvement in wheeze was reported in two studies.
CONCLUSIONS The published literature does not consistently support treatment of reflux oesophagitis as a means of controlling asthma. Further large randomised controlled trials in subjects with a demonstrated temporal relationship between gastro-oesophageal reflux and asthma are needed. These trials should be conducted over at least 6 months to allow adequate time to observe a treatment effect.
- asthma
- gastro-oesophageal reflux
- systematic review
Statistics from Altmetric.com
Gastro-oesophageal reflux occurs frequently in adults and children with asthma1-3 and is reported to be a trigger for difficult to control asthma.4 Gastro-oesophageal reflux, the passage of gastric contents through the gastric cardia into the oesophagus, can be a physiological event that occurs mainly after meals in healthy people. Abnormal reflux is defined as significant acid exposure (pH <4.0) to the distal oesophagus for more than 1.2 hours (cumulative time >5%) over a 24 hour period as established by intra-oesophageal pH monitoring.5 ,6Mechanisms by which oesophageal reflux may trigger asthma include acid aspiration,7 ,8 direct acid stimulation of the oesophagus, or stimulation of vagal nerves which heightens bronchial responsiveness to extrinsic allergens.9 ,10
Clinicians are advised to elucidate gastro-oesophageal reflux as a potential trigger in asthma and when gastro-oesophageal reflux is present, to consider treatment to improve asthma control.4 ,11 There are several approaches to treating gastro-oesophageal reflux: conservative anti-reflux measures; H2 antagonists either in standard dose or high dose; proton pump inhibitors; cisapride; and surgery including Nissen fundoplication and partial posterior hemi-fundoplication (Toupet and Lind techniques). Narrative reviews have identified that randomised trials have been conducted on each form of treatment with conflicting results.12-15 We have conducted a systematic review of the literature and meta-analysis to establish whether treatment of gastro-oesophageal reflux has beneficial effects on asthma outcomes.
Methods
This paper reports the results from a systematic review produced for the Cochrane Airways Group in 199816 that has been updated for this publication. A protocol was developed, reviewed by the Cochrane Airways Group, and published on the Cochrane database of systematic reviews prior to conducting the review. All randomised controlled trials of gastro-oesophageal reflux therapy published in any language and which reported at least one relevant asthma health outcome were included.
IDENTIFICATION OF RELEVANT STUDIES
An electronic search was undertaken of the Cochrane controlled clinical trials register (CCTR/Central) for papers published between the years 1966 and April 2000. The register is a combination of Medline, Embase, CINAHL, hand searched journals, and abstracts of meetings. The Cochrane Airways Groups clinical trials register was also searched and pharmaceutical companies were contacted to obtain results of unpublished trials. The following search strategy was employed: “asthma” or “wheez*”and “gastro-oesophageal reflux”or “gastro-esophageal reflux”or “reflux”or “ger” or“gerd” or “acid”or “oesophagus”or “gastrooesophageal reflux”and “cimetidine”or “ranitidine”or “famotidine”or “nizatidine”or “omeprazole”or “pantoprazole”or “lansoprazole”or “surgery”or “Nissen”. The titles, abstracts, and keywords of identified articles were screened for relevance and the reference lists of relevant articles were hand searched for additional articles. The authors of included studies were contacted in order to identify any additional published or unpublished studies. We included randomised controlled trials and controlled studies of any gastro-oesophageal reflux treatment in patients with asthma.
ASSESSMENT OF VALIDITY
To minimise bias, two reviewers independently assessed the full text version of the trials for inclusion/exclusion, methodological quality, and data extraction using standardised forms. The percentage agreement for inclusion/exclusion was 100%. Methodological quality was assessed using two instruments. The first, the Jadad system,17 scores the quality of the paper based on descriptions of inclusion criteria (1 point), randomisation (stated, and appropriate; 2 points), adverse effects (1 point), blinding (described and appropriate; 2 points), description of withdrawals and dropouts (1 point), and statistical analysis (1 point). Each criterion was scored and summed to give a maximum score of 8. Studies were further assessed as “adequate”, “inadequate”, or “unclear” according to the actual methods used for randomisation and concealment of allocation. Authors were contacted to verify data and provide further information about methodological approaches and outcomes.
ANALYSIS
For continuous outcomes that were the same unit of measure, a weighted mean difference (WMD) and 95% confidence interval was calculated.18 Fixed effects models were used and significance accepted at p<0.05. For dichotomous outcomes the relative risk was calculated with 95% confidence intervals. The relative risk is the risk of experiencing an outcome when treated compared with the risk of experiencing that outcome if untreated. Values of <1 indicate a favourable treatment effect. Heterogeneity of the pooled trial results was calculated using a χ2 test with appropriate degrees of freedom. Where the heterogeneity exceeded the expected 90% level, the results were not pooled and subgroup analysis was carried out to try to explain the source of the heterogeneity.
Outcomes were analysed according to the type of intervention the subjects received—that is, medical or surgical treatment. Medical interventions were subgrouped according to the type of treatment: (1) H2 antagonist; (2) proton pump inhibitor; or (3) conservative treatment
Results
INCLUDED STUDIES
The search strategy yielded 259 abstracts of which 21 full text versions of papers and one abstract were retrieved. Of these, 12 randomised controlled trials19-30 were included. Nine were crossover trials and three used a parallel design. Four trials investigated H2 antagonists,19 ,21 ,22 ,26 six investigated proton pump inhibitors,20 ,25 ,27-30 one assessed conservative treatment of gastro-oesophageal reflux,23 and one had three arms which included a surgical approach, an H2 antagonist, and a placebo control.24 The characteristics of the included studies are described in table 1. Ten studies were excluded because the subjects did not have asthma,31-35 the trials were not randomised36 or not controlled,37 the interventions did not treat reflux,38 ,39 or the subjects did not have reflux.40
Characteristics of included studies
METHODOLOGICAL QUALITY
All studies were appropriately randomised except that by Kjellenet al 23 which used alternation to allocate subjects into treatment or control groups. Nine of the 12 studies used blinded allocation procedures. The range of study quality ratings was 4–7, the mode 7 and the mean 6.2 indicating only minimal opportunity for bias among these studies.
SUBJECT CHARACTERISTICS
Characteristics of the subjects are summarised in table 2. They were typically adults with symptomatic reflux. Asthma was diagnosed most commonly in accordance with the American Thoracic Society guidelines or a doctor's diagnosis. The severity of asthma varied from mild to severe. Gastro-oesophageal reflux was confirmed by one or more of the following methods: history of symptoms, endoscopy, manometry, acid perfusion test, 24 hour pH monitoring, and/or measurement of oesophageal motility. Reporting of gastro-oesophageal reflux severity tended to be more explicit than reporting of asthma severity. A clinical relationship between asthma and gastro-oesophageal reflux was reported in four studies,19 ,21 ,25 ,26 one of which excluded subjects that could not demonstrate this relationship.26
Summary of subject characteristics of included studies
OUTCOMES
Twelve randomised controlled trials investigated the treatment of gastro-oesophageal reflux on asthma in 432 subjects of whom 396 completed the studies. Asthma outcomes were reported inconsistently among the studies and this limited quantitative data synthesis (meta-analysis). No studies reported hospital admissions or emergency room visits resulting from asthma. The study results are summarised in table 3.
Summary of results of gastro-oesophageal reflux treatment on asthma outcomes
LUNG FUNCTION
Overall, there was no clear and consistent benefit of anti-reflux treatment on lung function in asthmatic patients with gastro-oesophageal reflux. Ten trials of 11 interventions reported forced expiratory volume in one second (FEV1). Of these, one omeprazole and one cimetidine intervention reported a small but significant improvement in FEV1,24 ,25 whereas the remaining studies found no benefit of gastro-oesophageal reflux treatment on FEV1.
An improvement in morning peak expiratory flow (PEF) was reported in only one of the six studies that reported this variable.29A meta-analysis of these studies indicated no effect of anti-reflux therapy on morning peak flow (fig 1). A significant improvement in evening PEF, measured as percentage of predicted, was reported after treatment with omeprazole 40 mg/day for 4 weeks27 and after treatment with cimetidine 1000 mg/day for 6 weeks.21 However, no effect of treatment on evening PEF was reported in five other studies.19 ,20 ,26 ,28 ,29Similarly, our unpaired analysis of three studies19-27using the PEF end point in l/min showed no significant treatment effect on evening PEF (fig 2). Daytime PEF was not reported to be improved with treatment for reflux oesophagitis.20-22 ,25 Airway hyperresponsiveness was not affected by treatment with omeprazole27 ,28 or with an H2antagonist.19 ,22

Effect of medical treatment for gastro-oesophageal reflux versus placebo on morning peak expiratory flow. Weighted mean difference (WMD) for individual trials. χ2 refers to test for heterogeneity across different trials. Z is the test statistic for weighted mean difference. WMD for individual trials (area of the square proportional to amount of information contributed) and for total (diamond = WMD and 95% CI). The convention of favourable results being displayed to the left hand side of null effect warrants negative signs being placed before results. Results are reported as l/min.

Effect of medical treatment for gastro-oesophageal reflux versus placebo on evening peak expiratory flow. Weighted mean difference (WMD) for individual trials. Results are reported as l/min.
SYMPTOMS
Asthma symptoms were measured and reported in all of the included studies but in so many different ways that a meaningful combination of the data was not possible.
Of the 12 trials, three reported a significant improvement in symptoms. Kjellen et al 23 reported a significant reduction in the proportion of subjects experiencing respiratory symptoms including dyspnoea, cough, wheeze, and expectoration after conservative treatment for gastro-oesophageal reflux. This study had significant potential for bias as allocation to treatment groups was by alternation. Larrain et al 24 found significant improvement in both treatment groups (cimetidine and surgical) as well as in the placebo group when comparing the change in asthma symptoms from baseline to follow up. The cimetidine and surgical groups showed significant improvement in asthma symptoms over the placebo group after 6 months. Levin et al 29 reported an improvement in asthma related quality of life with omeprazole. The remaining nine trials found no significant treatment benefit.
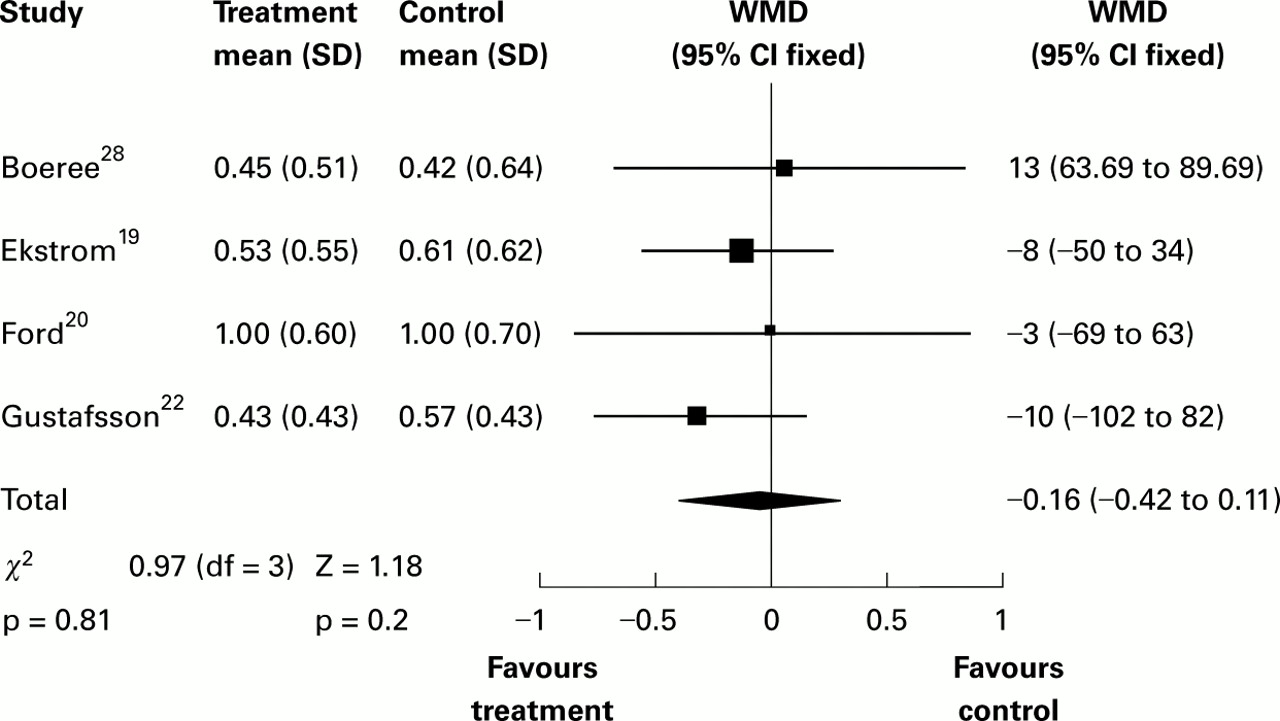
Three out of six studies which measured and reported nocturnal asthma symptoms found a treatment related improvement. Ekstromet al 19 reported a significant but clinically modest improvement in nocturnal asthma symptom scores after treatment with an H2 antagonist. In this study, subjects who had a history of reflux associated respiratory symptoms showed a greater improvement with ranitidine. Goodallet al 21 also demonstrated a positive effect of an H2 antagonist on nocturnal asthma. Kiljander et al 30 reported fewer nocturnal symptoms with high dose omeprazole, whereas Boereeet al 28 found no such effect. Gustafsson et al 22 reported significant positive correlations between the improvement in nocturnal, morning, and total asthma symptoms and the degree of pathological gastro-oesophageal reflux at oesophageal pH monitoring in children and adolescents. However, the overall results from Gustafssonet al 22 and Fordet al 20 did not demonstrate a benefit on nocturnal asthma symptoms from gastro-oesophageal reflux treatment (fig 3).

{kind=link}
{kind=link}
{kind=link}
Effect of medical treatment for gastro-oesophageal reflux versus placebo on nocturnal asthma symptom scores. Standardised mean difference (SMD) for individual trials (area of the square proportional to amount of information contributed) and for total (diamond = SMD and 95% CI).
Three of seven studies reported a significant reduction in β agonist use and this effect was greatest in those subjects who had a history of reflux associated respiratory symptoms. The reduction was from 5.9 (0.92) to 5.2 (0.88) puffs of β2 agonist per day and is of doubtful clinical significance. Kjellen et al 23 also reported a significant reduction in the consumption of β-adrenergic sprays in the treatment group (4.4 to 3.8 doses/day). Larrain et al 24recorded a total medication score and found a significant reduction from baseline to follow up at 6 months in patients treated with cimetidine and those who underwent surgery, and a non-significant increase in the placebo group. Five other trials did not find a treatment related improvement in consumption of rescue medication20 ,21 ,25 ,26 ,30 despite having adequate power to do so.
GASTRO-OESOPHAGEAL REFLUX INDUCED ASTHMA
Four studies identified subjects in whom reflux appeared to trigger asthma. In these subjects, although gastro-oesophageal reflux was temporally associated with asthma,19 ,21 ,25 ,26 no consistent benefit of gastro-oesophageal reflux therapy was demonstrated on asthma outcomes (tables 2 and 3).
EFFECT OF TREATMENT ON GASTRO-OESOPHAGEAL REFLUX
The effect of study treatment on gastro-oesophageal reflux was reported in 11 of the 12 trials. Symptoms were assessed in 10 studies and study treatment improved reflux symptoms in only five of them. The effect of treatment on oesophageal pH was assessed in three studies and was improved by high dose omeprazole28 and surgery24 but not by H2antagonists24 or by low dose omeprazole.27
Discussion
In this systematic review of 12 randomised controlled clinical trials the treatment of gastro-oesophageal reflux did not reveal a consistent benefit on asthma. There was no clear effect on lung function, airway responsiveness, or asthma symptoms. Although nine of the 12 trials reported at least one significant outcome, there was no consistency in these effects.
In general, the participants in these studies were selected on the basis of having a diagnosis of asthma and gastro-oesophageal reflux. Gastro-oesophageal reflux was diagnosed by various methods including oesophageal pH monitoring (distal and proximal), endoscopy, history of symptoms, and acid perfusion test. Not all subjects had symptomatic gastro-oesophageal reflux during the study period. Furthermore, a requirement to show that gastro-oesophageal reflux precipitated asthma was an entry criterion in only two studies.25 ,26FEV1 improved in one of these studies but other outcomes were negative. An association was found to be present in a subset of subjects in two further trials. Ekstrom et al 19 reported an improvement in nocturnal asthma and use of rescue medications. Goodall et al 21 also reported an improvement in nocturnal asthma symptoms and an improvement in evening PEF.
The lack of consistently convincing evidence among the randomised controlled trials contrasts with prior uncontrolled studies41 which reported a good response of gastro-oesophageal reflux treatment in some asthmatic subjects. The underlying reasons for the inconsistent results are not clear. The effect of bias may have contributed to the different findings since non-randomised study designs have the potential to overestimate treatment effects. Non-publication of negative observational trials may be a further reason for the difference in findings between the two study designs. It is also interesting to compare our observations with those of Field and Sutherland who analysed combined data from multiple studies of anti-reflux therapy in asthma.42 Although they included all the studies that we did, they also used three trials with open design.3 ,36 ,41 These three uncontrolled studies all had positive outcomes with reduced asthma symptoms (all three studies), less medication use (one study), and improved spirometric parameters (one study). Their overall conclusion from analysis of their combined data was favourable, reinforcing the belief that inclusion of studies with poor quality design will overestimate the benefits of treatment.
We found an insufficient sample size in the pooled studies to detect a clinically significant treatment effect in PEF. It is therefore possible that current studies are negative because of a type 2 error. Using the estimates of sample variance from the meta-analysis of PEF data, a sample size of 506 subjects would be required to detect a difference in PEF of 20 l/min with α at 0.05 and power of 80%. The pooled sample size of studies reporting evening PEF as an outcome was 184 (fig 1). The review by Field and Sutherland42 also concluded that medical anti-reflux treatment has minimal or no effect on lung function.
The duration of drug treatment used in the studies included in our systematic review was often short. It might be argued that a longer period of treatment would be necessary before improved control of gastro-oesophageal reflux resulted in benefits for asthma. Indeed, when treatment was given for 6 months,24 asthma symptoms and use of medications were improved. Studies consistently averaged the results over the entire treatment period for symptom scores, PEF, and medication use. If the effect of treatment was delayed or required time to be manifest, then averaging results over the entire treatment period would bias against finding a treatment effect. The likely implication is that these studies might underestimate the response to gastro-oesophageal reflux therapy.
Our original intention had been to look at the effect of treatment of gastro-oesophageal reflux in both adults and children with asthma. The paucity of appropriate paediatric studies limited the scope of the final review, with the study by Gustafsson et al 22 being the only randomised controlled trial to include children (age range for patients in this study 10–20 years, mean age 14.2 years). There is therefore no way of determining whether the observations made in this systematic review are generalisable to children with asthma and gastro-oesophageal reflux.
The relationships between asthma and gastro-oesophageal reflux have been well recognised. Both conditions are common and would be expected to coexist, purely on the basis of chance. Studies in children2 ,3 ,43 and adults1 have found a high prevalence of gastro-oesophageal reflux in patients with asthma, which suggests that the relationship may be causal rather than casual. A number of mechanisms could explain how gastro-oesophageal reflux would trigger asthma. Aspiration of gastric contents into the airways is an obvious possibility. Similarly, acid stimulation of vagal nerve fibres in the mid oesophagus can result in wheeze. On the other hand, the large swings in intrathoracic pressure associated with acute exacerbations of asthma might result in asthma promoting reflux. Clinical observation suggests that there are individuals in whom gastro-oesophageal reflux is an important trigger to asthma. However, it is unclear whether or not this is a common phenomenon.
Medical treatment of gastro-oesophageal reflux for asthma relies on the assumption that it is the acidity of the refluxed material that induces respiratory symptoms, not the presence of the material (acidic or not) in the lower oesophagus. It is not clear if those individuals who respond to treatment do so because of an improvement in lower oesophageal pH and a consequent reduction in oesophagitis, or because of a reduction in the quantity of refluxed material into the lower oesophagus, or both. There appears to be little evidence to indicate that acid perfusion has a significant adverse effect on lung function.44 To have the greatest chance of finding an improvement in asthma symptoms and lung function, the treatment needs to be effective in controlling reflux as well as reducing acidity. This review found a variety of treatments for reflux, with surgical, medical and non-pharmacological therapies. An obvious question to ask is whether the therapies used were successful in treating the reflux and/or the reflux oesophagitis. This was only objectively confirmed in two studies using high dose omeprazole28 and surgery.24 An optimal study design would establish that the reflux oesophagitis was adequately treated as a prerequisite to an assessment of the effect on the asthma.
Future research is warranted to examine the effects of treatment for gastro-oesophageal reflux on asthma control. A parallel group, randomised, placebo controlled trial with a surgical arm versus high dose proton pump inhibitor for up to 6 months would be appropriate. Subjects with symptomatic asthma and symptomatic gastro-oesophageal reflux in whom gastro-oesophageal reflux was shown to precipitate episodes of asthma should be studied, with assessment of day and night asthma symptoms, quality of life, lung function, and PEF, and an assessment of the effects of treatment on gastro-oesophageal reflux. The data should be evaluated as change from baseline, or data during the last few weeks of treatment should be compared between groups. A large sample size would be required, and pooled variance estimates from this review indicate the need to include 250 subjects in each treatment arm.
In conclusion, control of asthma was not consistently improved when asthmatic subjects were treated for gastro-oesophageal reflux. A subgroup of patients were reported to gain benefit but it appears difficult to predict responders. An improvement in symptoms was more likely to be observed than an improvement in lung function. At present it is not possible to recommend the general application of medical treatment of reflux oesophagitis as a means of controlling asthma. Further research is required in selected subgroups treated either surgically or medically for a prolonged period.
Acknowledgments
The authors would like to thank NSW Health and National Asthma Campaign for their financial and administrative support respectively. We would also like to thank Dr T Ekstrom, Dr P M Gustafsson, Dr A Larrain, and Dr H Teichtahl for responding to our request for further information about their studies.