Article Text

Abstract
Antileukotriene drugs are new therapeutic agents that have recently been approved for the treatment of asthma. Several cases of eosinophilic conditions including Churg-Strauss syndrome have been reported to be associated with zafirlukast, a cysteinyl leukotriene type 1 receptor antagonist. So far no other leukotriene modifier has been associated with the syndrome. The case history is presented of a man with allergic rhinitis and asthma who had received intermittent pulse therapy with oral corticosteroids. Pulmonary eosinophilia developed while he was receiving treatment with montelukast, a chemically distinct cysteinyl leukotriene type 1 receptor antagonist. After discontinuation of montelukast therapy and administration of systemic corticosteroids the patient’s symptoms reversed rapidly and there was prompt resolution of the pulmonary infiltrates. We believe that cysteinyl leukotriene type 1 receptor antagonists are safe and effective drugs for most patients with asthma but caution is needed for those with more severe disease who require systemic corticosteroids, especially if they show characteristics of the atypical allergic diathesis seen in the prodromal phase of Churg-Strauss syndrome.
- montelukast
- side effects
- pulmonary eosinophilia
Statistics from Altmetric.com
The antileukotriene drugs are new therapeutic agents which have recently been approved and are now available for the treatment of asthma in several countries. These drugs include one enzyme inhibitor of 5-lipoxygenase, zileuton, and three chemically distinct cysteinyl leukotriene type 1 receptor antagonists, zafirlukast, pranlukast and montelukast.1
Although clinical studies have shown that antileukotriene drugs are safe and effective, the results do not yet provide guidelines for their optimal clinical use in the treatment of asthma.1 As the use of these drugs increases, adverse events occurring at low frequency or in populations not examined in clinical trials may become manifest.2 Several cases of eosinophilic conditions including Churg-Strauss syndrome have been reported in patients who have been treated with zafirlukast.2-4 No other leukotriene modifier has yet been associated with the syndrome.
In this case report we describe an asthmatic patient in whom pulmonary eosinophilia developed while receiving montelukast therapy.
Case report
A 26 year old man with a three year history of asthma had received treatment with salbutamol, nedocromil, theophylline, and beclomethasone. There was a five year history of allergic rhinitis with positive skin tests for house dust mite and cat dander. Because asthma symptoms were not well controlled, treatment was started with fluticasone 1000 μg daily and salmeterol twice a day. Allergen immunotherapy was also prescribed. Nonetheless, short courses of oral prednisone 40 mg or deflazacort 60 mg daily were required on several occasions to control asthma exacerbations. A decision was made to initiate treatment with montelukast at a dose of 10 mg daily in the evening. Treatment with fluticasone was continued.
After approximately four months of treatment with montelukast the patient developed headache, malaise, myalgia, nasal congestion, and fever up to 39ºC. Oral cefuroxime and paracetamol were prescribed. Seven days later the patient developed dyspnoea and was admitted to our hospital.
On physical examination there were diffuse wheezes and ronchi. No cutaneous lesions or arthritis were found. A chest radiograph (fig 1) showed mixed alveolar-interstitial infiltrates in the upper lobes. Laboratory findings demonstrated a white blood cell count of 13.9 × 109/l with an eosinophil fraction of 0.14; the total IgE level was 527 IU/l and the results of an antineutrophil cytoplasmic antibody (ANCA) test were negative. A specimen of arterial blood, drawn while the patient was breathing room air, had a pH of 7.45 with oxygen tension (Pao 2) of 8.7 kPa and carbon dioxide tension (Paco 2) of 5.0 kPa. A fibreoptic bronchoscopic examination found no endobronchial lesions. Bronchoalveolar lavage fluid (fig 2) contained macrophages (10%), lymphocytes (10%), and eosinophils (80%). No acid-fast bacilli, fungi, or parasites were seen in the lavage fluid. Microscopic examination of a stool specimen disclosed no parasites.
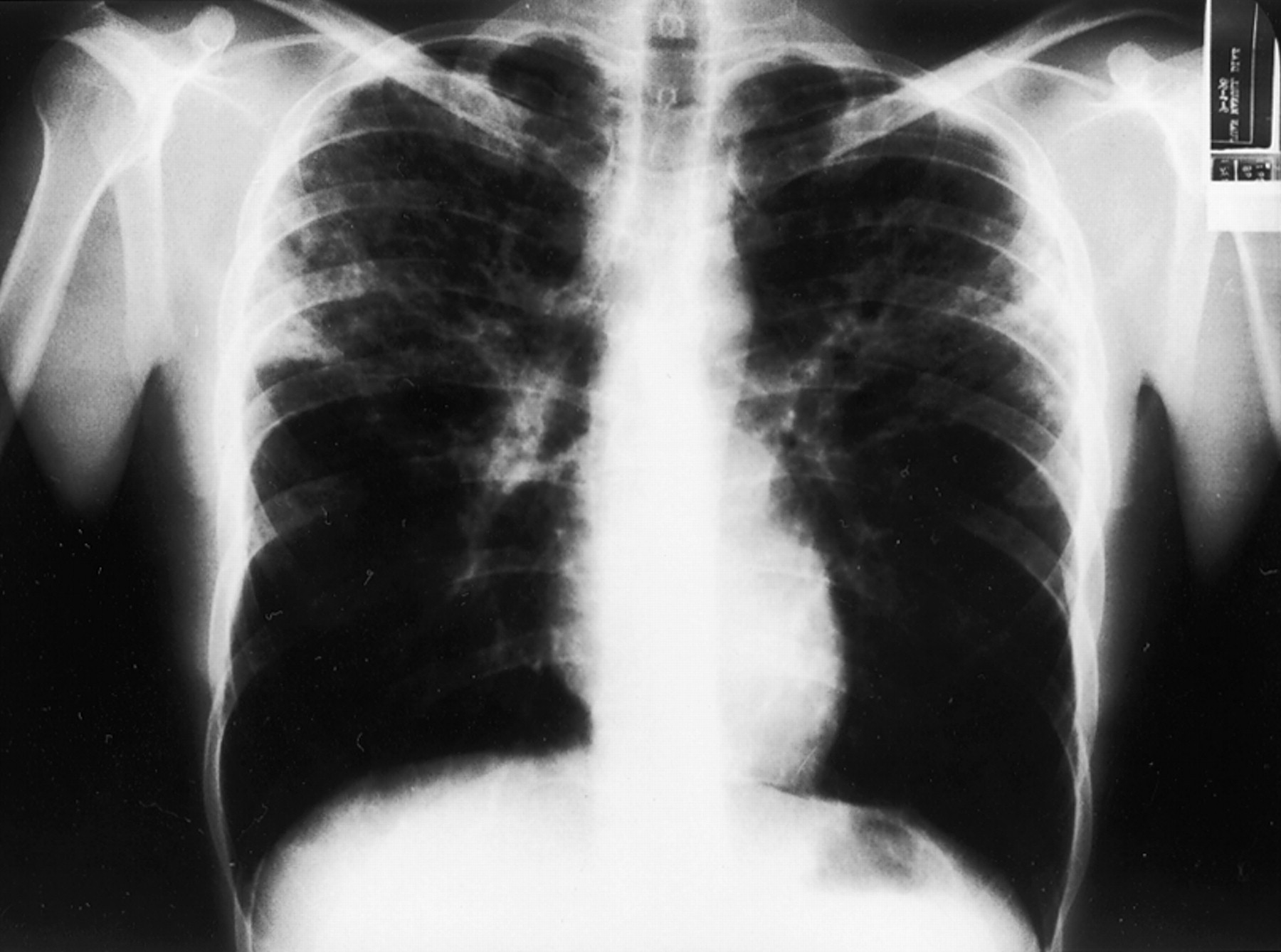
Posteroanterior radiograph of the chest showing mixed alveolar-interstitial infiltrates in both upper lobes.

{kind=link}
{kind=link}
Bronchoalveolar lavage fluid showing a large number of eosinophils as well as scant macrophages. Papanicolaou stain; ×40.
Montelukast treatment was discontinued and treatment with intravenous methylprednisolone at a dosage of 60 mg daily was begun. Both dyspnoea and constitutional symptoms improved within a short time. After nine days of treatment with high dose systemic corticosteroids a chest radiograph revealed resolution of pulmonary infiltrates.
Discussion
Montelukast is a potent and selective cysteinyl leukotriene type 1 receptor antagonist with potency and oral activity similar to those of zafirlukast.5 At a dosage of 10 mg montelukast inhibits bronchospasm after allergen or exercise challenge and causes clinically significant improvement in patients with asthma. The tolerability profile of montelukast was similar to that of placebo in placebo controlled clinical trials in adults and children, and the most common adverse effect reported was headache.6
In the case reported here the temporal relationship between montelukast treatment and the development of pulmonary eosinophilia suggests a causal association. However, we cannot exclude the possibility that the patient might have developed another eosinophilic condition such as allergic bronchopulmonary aspergillosis even without treatment with montelukast. The absence of parasites in the stools and the bronchoscopic specimens makes parasite induced eosinophilic lung disease unlikely. Despite the lack of systemic vasculitis and a negative ANCA, this patient with his five year history of allergic rhinitis, progressive airways symptoms, and intermittent treatment with oral corticosteroids could have a forme frustre of Churg-Strauss syndrome.
Wechsler et al 2 reported eight cases of Churg-Strauss syndrome following discontinuation of treatment with oral corticosteroids in patients with asthma receiving zafirlukast. The authors speculated that all these patients suffered from a primary eosinophilic infiltrative disorder that was unmasked when steroids were withdrawn. However, in two other cases of Churg-Strauss syndrome associated with zafirlukast therapy3 ,4 and in the case of pulmonary eosinophilia reported in this paper there was no association between corticosteroid withdrawal and the development of the syndrome. Because all these patients had moderate to severe asthma and had received intermittent or regular treatment with oral corticosteroids, they could have been formes frustres of Churg-Strauss syndrome whose manifestations were quelled by prior steroid treatment.7
As this syndrome has not yet been seen in patients treated with zileuton, a drug that inhibits leukotriene B4 (LTB4) and cysteinyl leukotrienes (LTC4, LTD4 and LTE4), an alternative explanation based on the imbalance in leukotriene receptor stimulation has been put forward.8 Cysteinyl leukotriene type 1 receptor antagonism may have led to increased circulating LTB4 which has been shown to be a chemoattractant for eosinophils as well as neutrophils.9
Pulmonary eosinophilia associated with a cysteinyl leukotriene type 1 receptor antagonist other than zafirlukast suggests that the syndrome may be related to the effect of antileukotriene drugs on leukotriene receptors.
Churg-Strauss syndrome is a disorder characterised by hypereosinophilia and systemic vasculitis which occurs in a subset of patients with asthma and allergic rhinitis whose allergic diathesis is atypical with respect to the late age of onset of symptoms, frequent absence of family history, severity of upper respiratory tract disease, and exaggerated eosinophil response.10 The patient described here and the cases of Churg-Strauss syndrome associated with zafirlukast previously reported could belong to this category of patients. We hypothesise that, in such individuals, cysteinyl leukotriene type 1 receptor antagonists can precipitate the phase of the illness characterised by eosinophilic tissue infiltrates or life threatening systemic vasculitis.
We believe that cysteinyl leukotriene type 1 receptor antagonists remain safe and effective drugs for most patients with mild to moderate asthma but, while the exact causes of the syndrome are not well understood, caution is needed for those with more severe disease who require systemic corticosteroids, especially if they show characteristics of the atypical allergic diathesis seen in the prodromal phase of Churg-Strauss syndrome.