Article Text

Abstract
BACKGROUND Although many asthmatic patients are treated with a combination of β2 agonist and corticosteroid inhalers, the clinical effects of combining the drugs are unknown. Studies on the early asthmatic response to allergen suggest that β2 agonists may reduce the benefit of inhaled corticosteroids. A study of the effects of combining the drugs on asthma control was undertaken.
METHODS Sixty one subjects with mild to moderate asthma were randomised to a double blind crossover comparison of inhaled budesonide (200–400 μg twice daily), terbutaline (500–1000 μg four times daily), combined treatment, and placebo. Each treatment was given for six weeks following a four week washout period. Ipratropium was used for symptom relief. Treatments were ranked from worst (1) to best (4) based on need for oral steroid, mean morning peak flow, nocturnal awakening, ipratropium use, and asthma symptoms. Lung function and bronchial hyperresponsiveness were measured before and after each treatment.
RESULTS Evaluable data for all four treatments were obtained from 47 subjects. The mean rank of each treatment was: placebo = 2.05; terbutaline = 2.13; budesonide = 2.48; combined treatment = 3.34. Combined treatment was ranked significantly better than any other treatment (p<0.01). Mean (95% CI) morning and evening peak flows were 14 (5 to 23) and 24 (15 to 34) l/min higher, respectively, during combined treatment than during budesonide, and 27 (17 to 37) and 15 (7 to 23) l/min higher than during terbutaline. Asthma symptoms tended to be least frequent during combined treatment but were not significantly different from budesonide alone. There was no significant difference between combined treatment and budesonide alone for lung function and bronchial hyperresponsiveness.
CONCLUSIONS In this group of mild to moderate asthmatic subjects the combination of β2 agonist and corticosteroid gave better asthma control than either treatment alone. There was no evidence that regular β2 agonist treatment impaired the beneficial effect of inhaled corticosteroid.
- asthma
- inhaled β2 agonists
- inhaled corticosteroids
Statistics from Altmetric.com
Inhaled corticosteroids are the most effective medication for long term control of asthma while short acting inhaled β2agonists are the treatment of choice for asthma symptoms.1 ,2 Although many patients use both drugs, there is little information on the effects of their combination. Two studies have shown that the addition of regular inhaled β2agonist to inhaled corticosteroid treatment reduces the protective effect of the corticosteroid against allergen challenge, suggesting that there may be a negative interaction between the two drugs.3 ,4 There is also in vitro evidence of a mutual inhibition between β2 agonists and corticosteroids on transcription factor binding in lung tissue.5 These findings have generated the hypothesis that β2 agonists antagonise the effects of corticosteroids.6
A negative interaction between corticosteroids and β2agonists could explain why regular inhaled β2 agonist treatment was associated with a deterioration in asthma control in an earlier investigation in which the majority of subjects were receiving inhaled corticosteroid treatment,7 but not in another study in which subjects receiving corticosteroids were excluded.8
The regular use of short acting β2 agonists is no longer recommended for maintenance therapy.1 ,2 However, in practice many asthmatic subjects continue to use these agents several times a day, and most will do so if their asthma is deteriorating. Thus, any impairment of corticosteroid action is most likely to occur in the setting of poorly controlled asthma when their anti-inflammatory effects are most needed. While combinations of the long acting β2 agonists salmeterol and formoterol with inhaled corticosteroids have been found to be superior to high dose inhaled corticosteroids alone,9-11 the prolonged bronchodilator action of these drugs might mask an adverse effect on airway inflammation. A negative effect would be more apparent during treatment with short acting β2 agonists but this has not been systematically investigated.
This study was designed to assess the interaction between inhaled β2 agonists and inhaled corticosteroids on asthma control. We performed a double blind, placebo controlled, random order, crossover trial comparing the effects of budesonide, terbutaline, and their combination in subjects with mild to moderate asthma.
Methods
SUBJECTS
Volunteers aged 9–64 with mild to moderate atopic asthma were recruited. All had bronchial hyperresponsiveness to methacholine (PC20 <8 mg/ml).12 Exclusion criteria were use of high dose inhaled corticosteroids (>1500 μg/day in adults, >800 μg/day in children aged <13); oral steroid treatment within the previous three months; current or ex-cigarette smokers (>5 pack years).
Asthma control was carefully monitored throughout the study. Each subject had an action plan, a supply of prednisone, a β2agonist inhaler, and 24 hour access to one of the investigators in case of an exacerbation. The study was approved by the Otago ethics committee. Each subject (or their parent/guardian) gave written informed consent to the study.
STUDY DESIGN
The study was a randomised four way crossover comparison of budesonide (Pulmicort, Astra Draco, Lund, Sweden) 400 μg twice daily, terbutaline (Bricanyl, Astra Draco) 1000 μg four times daily, both drugs (combined treatment), and placebo. Doses were halved for children under 13. The drugs were administered by dry powder inhaler (Turbuhaler, Astra Draco) with the use of dummy inhalers containing lactose to maintain blinding. Each treatment was given for six weeks preceded by a four week single blind washout period during which two placebo inhalers were used (fig 1). Throughout the treatment and washout periods subjects used ipratropium bromide (Atrovent, Boehringer Ingelheim, Germany) for symptom relief. No other asthma treatment was permitted except in the event of an exacerbation.

Study design. A = prednisone use during treatment period (“treatment failure”), study restarted at next washout when asthma stability restored; B = prednisone use during washout period, washout restarted when stable.
At the start of the study each subject discontinued all asthma treatment other than as required bronchodilator for two weeks. Thereafter, as required β2 agonists were replaced by ipratropium and subjects commenced the first washout. At the end of the first washout subjects were allocated to a double blind random sequence of the study treatments. Subjects were only randomised if they had been able to follow the study protocol and if their asthma control remained satisfactory. The first washout period was repeated if necessary. Subjects unable to tolerate the withdrawal of their maintenance asthma treatment were withdrawn from the study.
Each subject was given an action plan based on their previous “best” peak flow. If their peak flow fell to 60% of this value, or if severe asthma symptoms unresponsive to ipratropium occurred, they were instructed to take inhaled β2 agonist, oral prednisone (40 mg daily), and to contact the investigators. At randomisation the action plan was modified according to the highest morning peak flow during the last 14 days of the first washout. Thereafter, an exacerbation requiring prednisone use was regarded as “treatment failure” and participation in the study was temporarily discontinued. Providing asthma stability had been re-established, subjects re-entered the study at the next washout a minimum of four weeks after the corticosteroid had been discontinued (fig 1). If prednisone was required during a washout, the washout period was re-started four weeks after the last dose of corticosteroid. Subjects were requested not to use their β2 agonist inhaler during the study except in the event of an exacerbation.
MEASUREMENTS
Subjects kept a twice daily diary throughout the study. The best of three peak flows was recorded before taking the morning and evening study inhalers. Symptoms of nocturnal wheeze and cough, daytime wheeze and cough, exercise related asthma, and sputum production were scored on a scale of 0–3 (0 = none, 1 = mild, 2 = moderate, 3 = severe). The use of emergency asthma treatment (β2 agonist or corticosteroid) and compliance with the study inhalers was also recorded. Diary data from the first seven days of each treatment period were excluded from analysis.
At the beginning and end of each treatment subjects attended the research clinic for spirometric measurement of the forced expiratory volume in one second (FEV1). Methacholine challenges were performed at the same times using a modified version of the rapid challenge procedure13 in which increasing doses of methacholine (0.044–45 μmol) were delivered from a Hudson Updraft nebuliser (Temecula, California, USA) controlled by a Morgan Nebicheck dosimeter (Gillingham, UK). The provocative dose causing a 20% fall in FEV1 (PD20) was calculated by linear interpolation. Study inhalers and ipratropium were withheld for at least six hours before the spirometric tests and challenge procedures.
ANALYSIS OF RESULTS
The primary analysis was to construct a rank order of treatments from the worst (1) to the best (4) period of asthma control for each subject who started all four treatments. The rank order was established before the study was unblinded. Ranks were assigned using the diary data according to a hierarchy of criteria: if prednisone had been used in one of the treatment periods (“treatment failure”), that period was ranked worst. Morning peak flows were then compared between the remaining treatment periods. If there were significant differences in mean morning peak flow, these were used to assign ranks, the lowest being ranked worst. Remaining unranked treatment periods were then compared for the frequency of nocturnal wakening, followed by ipratropium use, then asthma score (see below). Duncan’s multiple range test (SPSS) was used to determine the significance of differences in morning peak flow. χ2 and Fisher exact tests were used for wakening, ipratropium use, and asthma score. A p value of <0.05 was considered significant using the Bonferroni correction to allow for multiple testing. Wilcoxon matched pair signed rank tests were used to calculate the statistical significance of differences in mean rank between treatments. To allow for multiple testing between pairs of treatments, significance was accepted at the p<0.01 level.
A composite asthma score was calculated for each day in the treatment periods according to change from baseline. The baseline was calculated as the mean morning peak flow, asthma symptoms, and ipratropium use during the last 14 days of each washout period. Scores were assigned according to the following criteria: 1 = morning peak flow ⩽90% of baseline plus an increase in any asthma symptom or an increase in more than one asthma symptom, or morning peak flow ⩽75% without an increase in symptoms; 2 = morning peak flow ⩽75%plus an increase in more than one asthma symptom, or morning peak flow ⩽60% without an increase in symptoms; 3 = morning peak flow ⩽60%plus an increase in more than one asthma symptom. Score 0 applied by default if none of the above applied. Days with insufficient data were not scored.
The results for all randomised subjects were also analysed on an intention-to-treat basis regardless of whether the subject completed the study: morning peak flow, evening peak flow, asthma scores, asthma symptoms, ipratropium use, FEV1, and PD20 were compared using a repeated measures analysis of variance (LSmeans statement of the SAS GLM procedure). PD20 values were log transformed before analysis. Where a 20% fall in FEV1 was not achieved after the maximum dose of methacholine, an arbitrary PD20 value of 64.0 μmol was assigned (halfway between the maximum dose delivered and the next theoretical doubling dose on a log scale).
Results
SUBJECTS
Of 104 volunteers recruited to the study, 61 started the randomised sequence of treatments (table 1). The most common reason for withdrawal before randomisation was a deterioration in asthma control (22 subjects, table 2). Of these, 20 had been using inhaled steroids before entering the study. The subjects who withdrew before randomisation had worse bronchial responsiveness to methacholine at enrolment (p = 0.03) and lower FEV1/FVC ratios (p<0.02) than those who were randomised. Following randomisation a further 12 subjects withdrew but only two because of poor asthma control. There were no significant differences in the baseline characteristics between those who completed the study and those who withdrew after randomisation. The diary data from five subjects (three of whom withdrew before completing the study) were excluded from analysis before the study was unblinded because of poor compliance with the recording of data. An analysis which included all the data from the five excluded subjects yielded similar results. Thus, 47 subjects were included in the analysis of worst/best treatment. FEV1 and PD20 data from all subjects were retained.
Baseline characteristics of the study volunteers
Reasons for withdrawal from the study
COMPLIANCE
The mean self-recorded compliance with the four times daily (terbutaline or placebo) and twice daily (budesonide or placebo) study inhalers was 90.4% and 94.4%, respectively. There was no significant difference in compliance between treatment periods.
TREATMENT FAILURES
Eleven treatment periods were terminated by the use of prednisone. This occurred twice during placebo, four times each during budesonide and terbutaline, and once during combined treatment.
WORST AND BEST TREATMENT
The mean treatment ranks (worst = 1, best = 4) were: placebo = 2.05; terbutaline = 2.13; budesonide = 2.48; combined treatment = 3.34. Combined treatment was ranked significantly higher than placebo, terbutaline, and budesonide (p<0.0001, p<0.0001, and p<0.01, respectively). Budesonide had a higher ranking than placebo (p = 0.025). There was no significant difference in rank between budesonide and terbutaline (p = 0.12), or between terbutaline and placebo (p = 0.46). The frequency with which each treatment was ranked from worst to best is shown in fig 2.

Frequency with which each treatment was ranked from worst to best. Tied ranks are represented as a half frequency in each column.
PEAK FLOW RATES
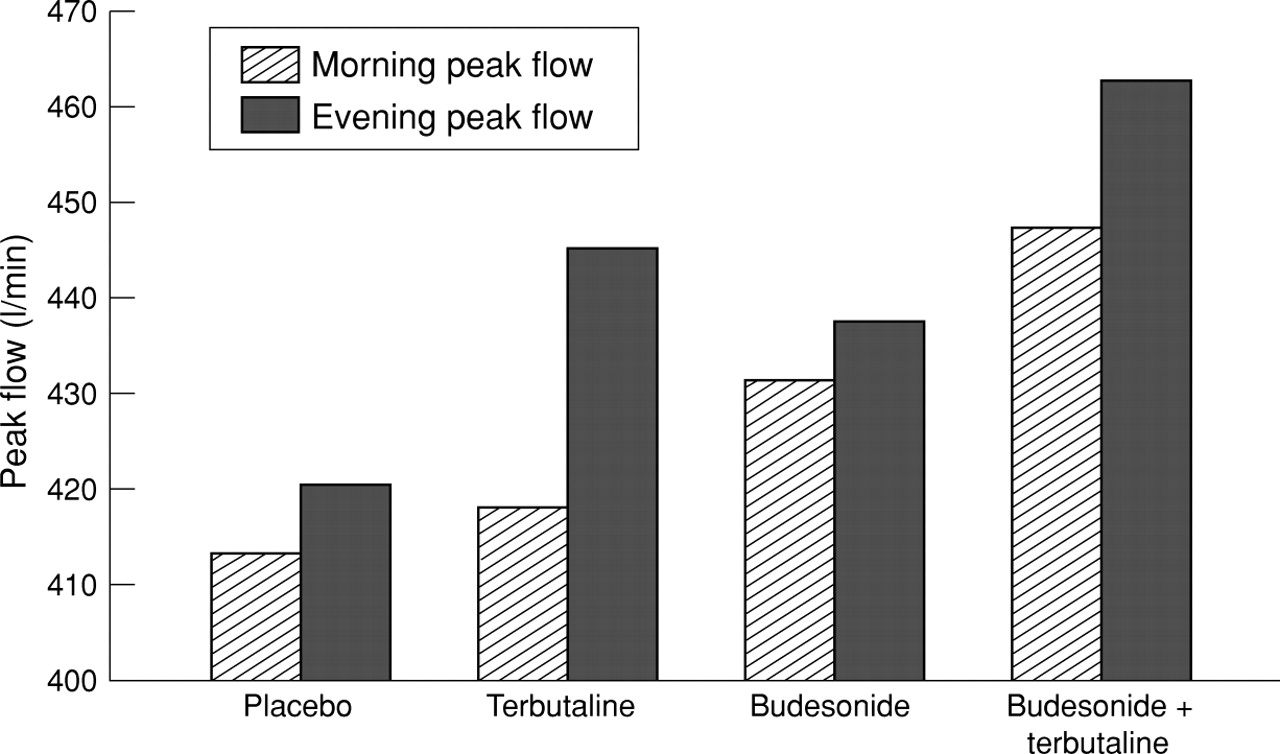
Mean morning peak flow was higher during both budesonide and combined treatment than during either placebo or terbutaline (p<0.01). Mean morning peak flow was higher during combined treatment than during budesonide (p<0.002) (table 3, fig 3). Terbutaline did not alter the morning peak flow when compared with placebo. The mean (95% CI) increases in morning peak flow compared with placebo were 33 (24 to 42), 19 (9 to 29), and 6 (–3 to 15) l/min for combined treatment, budesonide, and terbutaline, respectively. The increases in morning peak flow for combined treatment compared with budesonide or terbutaline alone were 14 (5 to 23) and 27 (17 to 37) l/min, respectively.
Mean peak flow (PF), asthma symptoms, lung function, and bronchial hyperresponsiveness
{kind=link}
{kind=link}
{kind=link}
Mean morning and evening peak flows with each treatment.
Mean evening peak flow was higher with all treatments than with placebo (p<0.0003; (table 3, fig 3), and was higher with combined treatment than with either budesonide or terbutaline alone (p<0.0002; table 3, fig 3). The difference between terbutaline and budesonide was not statistically significant. The mean (95% CI) increases in evening peak flow compared with placebo were 41 (31 to 51), 17 (9 to 24), and 26 (16 to 35) l/min for combined treatment, budesonide, and terbutaline, respectively. The increases in evening peak flow for combined treatment compared with budesonide or terbutaline alone were 24 (15 to 34) and 15 (7 to 23) l/min, respectively.
ASTHMA SYMPTOMS
Nocturnal wakening was significantly reduced with all active treatments compared with placebo (p<0.01), but there were no significant differences between the active treatments (table 3). The percentage of nights during which wheeze or chest tightness were reported was lower during budesonide and combined treatment than during placebo (p = 0.01) or terbutaline (p<0.001). The percentage of days during which wheeze was reported was reduced for all active treatments compared with placebo (p<0.001). The incidence of nocturnal cough, daytime cough, exercise induced asthma symptoms and sputum production was not significantly different between treatments (data not shown).
ADDITIONAL BRONCHODILATOR USE
Ipratropium use was reduced during all active treatment periods compared with placebo (p<0.001; table 3). There were no significant differences between active treatments.
ASTHMA SCORES
The percentage of days for which the asthma score was 1 or more was lower during budesonide and combined treatment than with placebo (p = 0.002 and p = 0.001, respectively; table 3). There was no difference between placebo and terbutaline. There were no significant differences between active treatments, although there was a trend for reduced scores with combined treatment compared with terbutaline (p = 0.03).
LUNG FUNCTION AND BRONCHIAL HYPERRESPONSIVENESS
Both budesonide and combined treatment improved FEV1compared with placebo or terbutaline (p<0.004; table 3). There was no significant difference between budesonide and combined treatment. Terbutaline alone had no significant effect on FEV1. PD20 values were higher after budesonide and combined treatment than after placebo or terbutaline (p<0.002), but there was no significant difference between budesonide and combined treatment. The PD20 after terbutaline was not significantly different from placebo. The change in PD20 (from before treatment to after treatment) during combined treatment was greater than during either placebo or terbutaline (p<0.001). The change in PD20 during budesonide was smaller than during combined treatment (not significant) and did not reach statistical significance compared with placebo or terbutaline (p = 0.10 and p = 0.06, respectively).
Discussion
In this study the combination of regular inhaled budesonide and terbutaline provided better asthma control than either drug alone. In more than half of the subjects who took all four treatments the combination was judged to have provided the best or equal best asthma control. The combination also provided the greatest increase in morning and evening peak flows. Although the mean FEV1 was not significantly different after the combination from after budesonide alone, there were trends towards an improvement in asthma symptoms and bronchial hyperresponsiveness.
We have previously shown that regular β2 agonist treatment resulted in a deterioration of asthma control and was associated with negative changes in lung function and bronchial hyperresponsiveness.7 ,14 Although a number of hypotheses have been suggested, the mechanism for these adverse outcomes has never been adequately explained.15 None of the observations in the present study supports the hypothesis that they were due to a negative interaction between β2 agonists and corticosteroids. In fact, a positive interaction was observed. There was a marked increase in morning peak flow during combined treatment compared with budesonide alone, an effect which is unlikely to be due to sustained bronchodilation after terbutaline since terbutaline alone had no effect on morning peak flow. This suggests that the addition of a β2 agonist in some way enhances the anti-inflammatory effects of inhaled corticosteroids. The mechanism for this is unclear. A simple explanation would be that bronchodilation due to β2 agonists improves the deposition of inhaled corticosteroids in the airways. Our findings extend the observations of recent studies which have shown that combinations of long acting β2 agonists and inhaled corticosteroids provide better asthma control and lung function than high dose inhaled corticosteroids alone.9-11 These benefits have previously been thought to be due to the sustained bronchodilator action of these drugs. However, the results of the present study suggest that they may, alternatively, be due to enhancement of the corticosteroid effect.
In contrast to our findings, two studies have demonstrated a reduced benefit from inhaled budesonide when combined with regular inhaled β2 agonist. Wong et alcompared treatment for 2–4 weeks with budesonide, terbutaline, both drugs, and placebo in a parallel group study of 41 asthmatic subjects and found that the protective effect of budesonide against allergen and histamine challenge was reduced in the group which had also received terbutaline.3 Cockcroft et alcompared budesonide, salbutamol, both drugs, and placebo for one week in a crossover study in 13 asthmatic subjects.4 They also found that the protective effect of budesonide against allergen challenge was reduced by the administration of salbutamol, but found no difference in bronchial hyperresponsiveness to methacholine. It is difficult to reconcile these findings with the results of the present study. However, they suggest that any impairment of the protective effect of inhaled corticosteroid against allergen by regular β2 agonist is unlikely to be important in the day-to-day management of asthma.
Few studies have investigated the clinical effects of combining inhaled corticosteroids with short acting β agonists. However, the available data appear to be consistent with our results. In a two week crossover study of 16 asthmatic subjects Wilding et alfound that treatment with combined budesonide and terbutaline was associated with higher morning and evening peak flows than budesonide alone, although the effect on morning peak flow was not statistically significant.16 Barnes and O’Connor also found that the addition of low dose terbutaline to inhalers containing budesonide was associated with higher morning and evening peak flows than either drug alone.17 However, the subjects used frequent inhalations of rescue β2 agonist throughout the study making the results difficult to interpret in terms of a possible drug interaction. A small study of salbutamol and beclomethasone in asthmatic children found no significant difference between the effects of combined treatment and beclomethasone alone on methacholine responsiveness although, as in the present study, there was a trend to greater benefit from the combination.18 In contrast, two earlier studies of regular β agonist treatment do not suggest a positive interaction with inhaled corticosteroids. Sears et al 7 found that fenoterol treatment caused a deterioration in asthma control regardless of whether the subjects were treated with inhaled corticosteroid. In a recent study regular salbutamol was found to have no effect on asthma control despite the fact that more than 90% of subjects were taking inhaled corticosteroids.19 These results suggest that there may be important differences between different β agonists, or that the relatively small number of patients in some studies and design differences may have influenced results.
Of necessity, the population that we studied tended to have mild to moderate rather than severe asthma. For ethical reasons the study was designed to identify those who were unable to tolerate the withdrawal of inhaled corticosteroid treatment before commencing the double blind treatments. Thus, 22 subjects withdrew before randomisation because of poor asthma control, whereas only two subsequently withdrew for asthma related reasons. This strategy may have led to a selection bias which would explain the initially surprising finding that budesonide alone was not ranked significantly higher than terbutaline or placebo. Notwithstanding this bias, there were significant improvements in peak flows, lung function, and bronchial hyperresponsiveness with budesonide alone, indicating that the study population was steroid responsive. The finding that asthma control was better with the combination of terbutaline and budesonide than with budesonide alone cannot be explained in terms of a selection bias. It is possible that subjects with more severe asthma would react differently to β agonists and their combination with an inhaled corticosteroid, although this seems unlikely.
In conclusion, in this prospective study we have found no evidence that β2 agonists impair the beneficial effects of inhaled corticosteroids in asthma. On the contrary, a positive interaction is suggested. In the past questions have been posed as to the mechanism by which the regular use of β2 agonists might cause worsening of asthma control.15 Our results provide reassurance that impairment of the action of corticosteroids is an unlikely explanation.
Acknowledgments
The authors thank the patients who participated in the study, Diana Gash and Astra Draco (New Zealand) for the study inhalers and randomisation sequence, and Boehringer Ingelheim for supplies of Atrovent. The study was funded by the Health Research Council of New Zealand and the New Zealand Lotteries Commission. RJH was a Glaxo-Wellcome Research Fellow.