Article Text

Abstract
BACKGROUND Steroid resistant asthma (SRA) represents a small subgroup of those patients who have asthma and who are difficult to manage. Two patients with apparent SRA are described, and 12 additional cases who were admitted to the same hospital are reviewed.
METHODS The subjects were selected from a tertiary hospital setting by review of all asthma patients admitted over a two year period. Subjects were defined as those who failed to respond to high doses of bronchodilators and oral glucocorticosteroids, as judged by subjective assessment, audible wheeze on examination, and serial peak flow measurements.
RESULTS In 11 of the 14 patients identified there was little to substantiate the diagnosis of severe or steroid resistant asthma apart from symptoms and upper respiratory wheeze. Useful tests to differentiate this group of patients from those with severe asthma appear to be: the inability to perform reproducible forced expiratory manoeuvres, normal airway resistance, and a concentration of histamine causing a 20% fall in the forced expiratory volume (FEV1) being within the range for normal subjects (PC20). Of the 14 subjects, four were health care staff and two reported childhood sexual abuse.
CONCLUSION Such patients are important to identify as they require supportive treatment which should not consist of high doses of glucocorticosteroids and β2 adrenergic agonists. Diagnoses other than asthma, such as gastro-oesophageal reflux, hyperventilation, vocal cord dysfunction and sleep apnoea, should be sought as these may be a cause of glucocorticosteroid treatment failure and pseudo-SRA, and may respond to alternative treatment.
- asthma
- corticosteroids
- hyperventilation
- gastro-oesophageal reflux
Statistics from Altmetric.com
Most patients with asthma are well controlled on inhaled treatment alone. Patients with very severe asthma often require long term oral glucocorticosteroids, but a few appear to be resistant to this form of treatment. Cases of steroid resistant asthma (SRA) have been well described but have been defined by different criteria.1-4 In general, SRA is defined by a failure of asthmatic symptoms and airway obstruction to improve if oral prednisolone is given for 14–28 days in a dose of 0.25–0.5 mg/kg/day. The degree of objective airway response has been defined as <15% improvement in baseline forced expiratory volume in one second (FEV1) for steroid resistant subjects, and >30% for steroid sensitive subjects,5 although a response is often not defined. Rarely, some patients with true SRA are thought to have an abnormal binding of the glucocorticoid receptor to its DNA binding site or other transcription factors.6
The patients we report were all referred to the Royal Brompton Hospital for assessment and treatment as they appeared to have asthma that was difficult to manage. All patients had symptoms of episodic breathlessness and wheeze, and showed variability in their peak expiratory flow (PEF) readings, which conform to the ATS definition of asthma.7
We present two cases and retrospectively studied a group of patients identified as having SRA and reviewed the features of their illness. The aim of the study was to identify investigations which suggested that a diagnosis of SRA was unlikely and would help prevent the administration of inappropriate oral glucocorticosteroids.
Case reports
CASE 1
A 38 year old woman presented with difficulty in breathing for 17 years. She had had asthma as a child until the age of seven. She had been symptom free until the age of 21 when she was treated for breathlessness with an inhaled β2 agonist as required, but due to increasing symptoms a gradual escalation in anti-asthma treatment occurred, including the administration of high dose inhaled corticosteroids. Over the previous two years she had been admitted to hospital on five occasions for breathlessness and was once admitted to the intensive care unit but was not ventilated. Her past history included pulmonary emboli treated by long term warfarin, and hysterectomy for carcinoma of the cervix. Continuous oral prednisolone had been prescribed for three years in varying doses and she had developed hypertension, diabetes mellitus, and back pain thought to be due to osteoporosis. On presentation her prednisolone had been increased to 40 mg orally and she was taking nebulised budesonide (1 mg twice daily), salbutamol 5 mg and ipratropium 500 μg six times a day, bendrofluazide 5 mg, enalapril 20 mg, and insulin in a total dose of 38 units per day. Positive features on examination were expiratory wheezes over the upper thorax. She weighed 96.5 kg (BMI 36.8). Routine clinical investigations showed no abnormalities except an elevated random glucose and glycosylated haemoglobin (table 1). The chest radiograph, ECG and skin prick tests were all normal. Serial twice daily spirometric tests showed poor reproducibility but no significant variability if poor effort was excluded. Formal lung function testing showed a slight decrease from predicted spirometric and lung volumes, but no evidence of obstruction. Flow loop demonstrated poor reproducibility and an upper airway type of obstruction pattern (fig 1, no. 1). Airway resistance by body plethysmography was normal, as were histamine PC20 and arterial blood gas tensions. Bronchoscopic examination showed that the vocal cords adducted during forced expiration and during inspiration, no endobronchial lesion was seen, and no significant eosinophilia was present in the bronchoalveolar lavage. An oesophageal pH monitor indicated that 14.2% of a 24 hour period was spent at a pH <4.0 (normal <4%).
Patient characteristics and indicators of atopy

{kind=link}
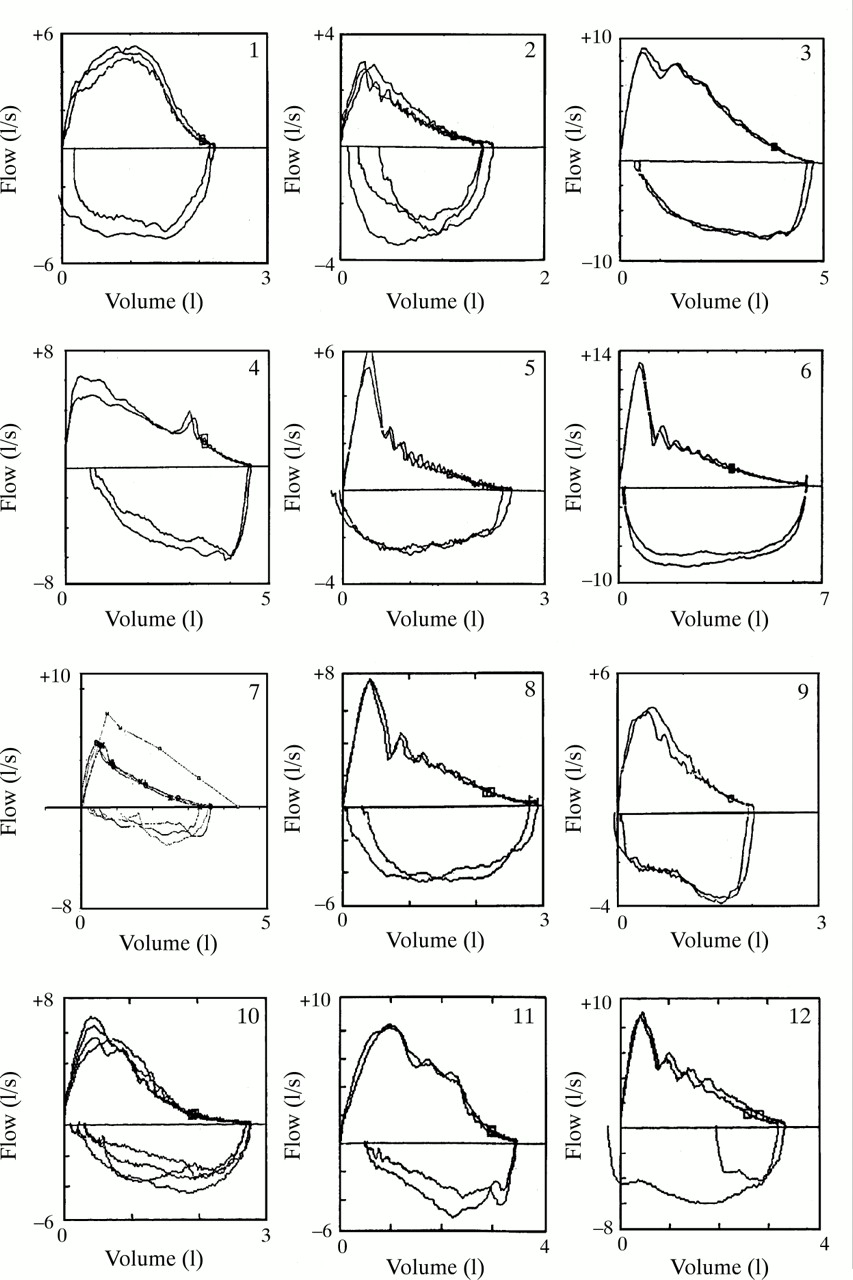
Original flow-volume curves from 11 subjects (see table 2, column 1 for subject identity). Curves were transferred from the original using a digital scanner. Many subjects show transient obstruction during expiration.
We concluded that the evidence for asthma was not convincing and that both vocal cord dysfunction and gastro-oesophageal reflux were more likely. As an inpatient she was weaned from all glucocorticosteroids. She was able to leave hospital on no regular anti-asthma medication without change in her spirometric values and with improved control of her diabetes and hypertension. Her gastro-oesophageal reflux was treated by dietary advice and initially omeprazole, but this was associated with a rash and cimetidine was substituted. She remained on no regular inhaled medication six months after withdrawal of her prednisolone.
CASE 2
A 31 year old woman presented with a diagnosis of asthma which had been made at the age of 17 years when she developed symptoms of cough, wheeze and shortness of breath. She had been given inhaled salbutamol and beclomethasone, but in the last five years had been admitted to hospital for asthma several times each year. Her asthma had been treated by long term prednisolone for the last three years, taking 20–60 mg per day, and she had been tried on cyclophosphamide, methotrexate, and triamcinolone. Drugs on admission were prednisolone 35 mg, terbutaline by continuous subcutaneous infusion 5 mg/day, salmeterol 50 μg inhaled/day, salbutamol 5 mg, and ipratropium 500 μg nebulised six times per day. She weighed 86 kg (BMI 37.2) and appeared cushingoid, but no other abnormalities were noted. Routine laboratory tests showed no abnormalities, but her IgE was raised at 391 IU/ml (table 1) and a pregnancy test was positive. The chest radiograph and ECG were normal. Twice daily spirometric tests showed poor repeatability. Lung function tests were remarkable for poor repeatability of the flow-volume loop and slight reduction in the lung volumes (fig 1, no. 2). Airway resistance was normal. There was no response to bronchodilator and she had a normal histamine PC20. A hyperventilation test was strongly positive with resting arterial blood gas tensions also indicating alkalosis (hydrogen ion concentration 33.4 mmol, Paco 2 3.7 kPa, Pao 2 13.95 kPa, HCO3 20.5 mmol, base excess 0.7). Oesophageal studies showed a pH of <4.0 for 11.2%/24 hours. Bronchoscopy was not performed as the patient was pregnant.
It was considered that hyperventilation syndrome with some gastro-oesophageal reflux was the likely diagnosis, with little to substantiate asthma. Prednisolone was reduced gradually to zero over a three week inpatient stay, and likewise β2 agonists were reduced to inhaled salbutamol by aerosol as required (<800 μg/day). Alginates and simple mechanical measures were suggested for the oesophageal reflux, with the advice that she lose more weight after her pregnancy. She was advised by the physiotherapists on measures to control her breathing to counteract hyperventilation episodes.
Methods
PATIENTS
Twelve more patients were identified from all the admissions for asthma over a 24 month period as having possible SRA from the case records of the Royal Brompton Hospital. SRA was defined by failure to respond to 20 mg or more of oral prednisolone after 14 days of treatment. Their case notes were studied and evidence for and against the diagnosis of asthma collected. Smoking history, occupation, other illnesses, weight and evidence of glucocorticosteroid side effects were also noted as a crude indicator of both compliance and steroid responsiveness outside the airway.
The following tests were attempted in all patients.
Indices of atopy
Subjects were assessed by total serum IgE, peripheral blood eosinophil count, and skin prick tests to four commonly encountered allergens (Felix domesticus,Dermatophagoides pteronyssinus,Aspergillus fumigatus, and mixed grasses (Soluprick, Allerologisk Laboratorium, Hørsholm, Denmark).
Spirometry
This was performed using a dry wedge spirometer (Vitalograph, Buckingham, UK). Individual traces were assessed where available.
Lung function tests
Formal lung function tests were carried out for spirometry, lung volumes, transfer factor, flow-volume loop, and body plethysmography. Bronchodilatation was assessed by the response of the FEV1to 200 μg of inhaled salbutamol, and the provocative concentration of histamine causing a 20% fall in baseline FEV1(histamine PC20) was determined.8 Variability of peak expiratory flow rate (PEF) was performed using a Wright mini-peak flow meter.
The following tests were also performed: arterial blood gas analysis; 24 hour oesophageal pH monitoring; hyperventilation test; psychiatric assessment; sleep studies of arterial oxygen saturation and transcutaneous CO2 monitoring (see table 1).
Results
All subjects were invited back for review of their asthma to complete the above list of investigations, but not all agreed to attend despite repeated requests. Table 1 lists the patient details. The subjects were more likely to be female (13:1), four were health care workers, and 11 reported multiple diseases, particularly dysmenorrhoea. Two reported a past history of sexual abuse. Nine were obese (BMI >25), two had morbid obesity, while eight had smoked and at least nine had atopy. A mean of 6.9 admissions per year had occurred over the preceding two years with one individual being admitted over 44 times/year.
Table 2 lists the relevant investigations. All showed PEF variability, but only five had an obstructive pattern on spirometric testing (most showing a reduction in both FEV1 and FVC, data not shown). Only two patients had a bronchodilatation of ⩾20% to β2 agonists and, of the seven tested by plethysmography, all had normal airway conductance (sGaw). Both patients 1 and 2 had a histamine PC20 within the normal range, but unfortunately most of the others did not have this test performed.
Results of the patients’ investigations and final diagnosis
Figure 1 shows the flow loops available on these patients. Those depicted are the most consistent of many attempts. It can be seen that there is often transient expiratory obstruction which could lead to a decrease in the value of the FEV1. The most common expiratory pattern seen has the appearance of rhythmic closure and opening of the vocal cords in expiration (nos 2, 5, 6, 8, and 12 in fig1). These are suggestive of transient obstruction followed by expiratory overshoot. This can be a feature of vocal cord dysfunction. Table 2 also lists the other tests which led to diagnoses other than asthma.
Discussion
It is evident that the patients described above belong to a heterogeneous group. The majority do not, however, have typical features of asthma. Some evidently have hyperventilation, others have gastro-oesophageal reflux or sleep apnoea, while some have psychiatric disease. A number of the patients had undergone intubation and ventilation, which in most cases was associated with a low Paco 2, perhaps representing hyperventilation and vocal cord dysfunction, while one ventilated individual was hypoxaemic and had sleep apnoea.
On the basis of their symptoms and PEF measurements, all of these patients described would fit the diagnosis of asthma according to the criteria of the American Thoracic Society,7 in as much as they exhibited variable airways obstruction, sometimes improving after β2 agonists, particularly when PEF alone was used. Nine of the 14 did not have airway obstruction from their FEV1:FVC ratio, while of seven tested for airway conductance, none had objective lower airway obstruction. Some had upper airway obstruction at the level of the larynx as judged by observation of the vocal cords or the pattern of the flow-volume loop. The inability to perform spirometric tests reproducibly, either on a simple dry wedge spirometer or as a flow-loop procedure, would suggest that upper airway closure could be the problem, indicating vocal cord dysfunction. In contrast, it is difficult to assess PEF effort and it is easy to manipulate the readings to either under or over-read and, in addition, variable effort may be mistaken for true PEF variability. Asthmatic subjects are, however, able to give consistent PEF and spirometric readings even in the presence of relatively severe obstruction.
Psychological aspects of asthma have attracted attention over the years, with some studies suggesting that asthmatic patients may have more personality problems than normal subjects, while other studies have implied that psychological disorders are no more common than would be expected for those suffering from a chronic disease.9It has become apparent, however, that a small number of patients have upper airway wheezing which is unrelated to asthma, and appears to be paradoxical laryngeal adduction during both expiration and inspiration. This vocal cord dysfunction may be associated with psychological disturbance and multiple diseases.10 ,11
Patients with SRA appear to have marginal therapeutic gain from treatment with steroids, but nonetheless are often given high doses of oral glucocorticoids to counteract their symptoms. It is therefore essential that patients who either have asthma that is difficult to manage, or require frequent and high doses of steroids or frequent hospital admission, have a critical reassessment of their diagnosis and review of their investigations. As experienced by the referring physicians, we found these patients difficult to manage and to assess, as can be seen by the tentative diagnoses in table 2. Some patients may appear to satisfy the definition of SRA but, upon review, probably do not have severe asthma at all. It is essential to identify patients with both true SRA and those with “pseudo-SRA” as the latter may mask a treatable disorder which is not asthma.
While our patients were not assessed by a protocol, having reviewed the above cases we would suggest the following as an assessment for those with difficult to manage or apparent “steroid resistant asthma” (see also Woolcock4):
- (1)
- does the patient definitely have asthma?—reproducible expiratory manoeuvre and FEV1 /FVC ratio of <70% or flow-volume curves and appropriate airway obstruction (not PEF measurements);
- (2)
- 20% reversibility of FEV1 (not PEF) to 200 μg salbutamol;
- (3)
- airway conductance/resistance;
- (4)
- histamine or methacholine challenge with PC20 result in appropriate range for asthma;
- (5)
- assessment of delivery of inhaled drugs and compliance;
- (6)
- bronchoscopy: assess movement of vocal cords on inspiration and expiration, bronchoalveolar lavage for eosinophils and differential cytology, biopsy for submucosal basement membrane thickening and to exclude endobronchial tumour;
- (7)
- three week 0.5 mg/kg prednisolone trial with repeated measures of FEV1, bronchial hyperreactivity and drug compliance;
- (8)
- investigations to exclude other treatable diseases: sleep study, 24 hour pH monitoring, hyperventilation test, psychological testing, etc.
Acknowledgments
We thank the physicians who referred these patients to The Royal Brompton Hospital, Derek Cramer for technical comments, and Sacha Sadler for computing excellence.