Article Text

Abstract
BACKGROUND The pathogenesis of non-asthmatic chronic dry cough remains unclear.
METHODS A study was undertaken to determine whether airway inflammation could be a contributing factor by analysing inflammatory cells and cytokines in induced sputum from 19 patients with chronic dry cough of varying aetiology, excluding asthma and bronchiectasis, and from 10 normal controls. The associated causes for the chronic cough were post-nasal drip (n = 5), gastro-oesophageal reflux (n = 4), and idiopathic (n = 10). All patients had an enhanced cough reflex to capsaicin.
RESULTS Sputum neutrophilia (median (interquartile range)) was found in the patients with chronic cough (59.4 (27.1)%) compared with the normal controls (28.4 (22.0)%; p<0.01, 95% CI 11.3 to 42.2). Sputum levels of interleukin-8 (IL-8) and tumour necrosis factor-α (TNF-α) were also significantly increased compared with normal controls (0.57 (1.08) and 0.25 (0.72) ng/ml; p<0.05 (95% CI 0.05 to 1.75) for IL-8; 48.3 (34.4) and 12.6 (33.6) pg/ml, p<0.01 (95% CI 8.8 to 69.8) for TNF-α).
CONCLUSION Neutrophils and cytokines associated with neutrophil chemotaxis and activation may contribute to the pathogenesis of non-asthmatic chronic dry cough.
- cough
- induced sputum
- neutrophils
Statistics from Altmetric.com
Chronic dry cough is a common clinical problem.1 ,2 Many investigators have identified asthma, rhinitis (or post-nasal drip), and gastro-oesophageal reflux as the clinical conditions most commonly associated with chronic cough.1 ,3 In many patients, however, no associated clinical conditions are present and this group is usually labelled as chronic idiopathic cough.2 ,4 Patients with chronic dry cough usually have an enhanced cough response to inhalation of tussive agents such as capsaicin or citric acid.5 The underlying mechanisms of this increased cough response are not known. Because the cough response to capsaicin can be enhanced by substances released during inflammation such as prostaglandins (particularly PGE2 and PGF2α) and bradykinin,6-8 it is possible that chronic airway inflammatory mechanisms may underlie chronic dry cough. Indeed, analysis of bronchoalveolar lavage fluid and biopsy specimens of the airway of patients with chronic dry cough not associated with asthma shows an increase in inflammatory cells with epithelial cell desquamation.9
Analysis of sputum induced by inhalation of hypertonic saline has recently been established as a useful non-invasive technique for measuring airway inflammation in patients with asthma and chronic obstructive pulmonary disease.10 ,11 We therefore used this technique to evaluate the presence of airway inflammation in patients with chronic dry cough.
Methods
PATIENTS
Consecutive non-smoking adult patients referred to the Cough Clinic of the Royal Brompton Hospital during a period of six months were enrolled into the study. Patients complained of a chronic dry cough defined as a persistent cough of at least three months’ duration. They underwent a protocol of diagnostic and therapeutic procedures in order to determine the cause of the chronic cough.2 Investigations included chest radiograph, bronchial provocation test with methacholine, 24 hour oesophageal acid monitoring, and a therapeutic trial of treatment for post-nasal drip. Patients who demonstrated bronchial hyperresponsiveness with a methacholine PC20 of less than 4 mg/ml or diurnal variation of peak flow of greater than 20% and whose cough had been controlled by inhaled corticosteroid therapy were diagnosed as having asthma as the cause of chronic cough. These patients were excluded from analysis. Cough associated with acid reflux was controlled by a four week course of omeprazole, and that deemed to be associated with post-nasal drip by topical nasal steroids. Those with idiopathic cough had no identifiable cause following additional investigations including a high resolution computed tomographic scan of the chest and fibreoptic bronchoscopy, and failure to respond to conventional therapy for gastro-oesophageal reflux and post-nasal drip. In all, we assessed 22 patients with a chronic cough and 10 normal volunteers who had no history suggestive of asthma or other airway disease, and a PC20 of >16 mg/ml.
The study was approved by the ethics committee of the Royal Brompton Hospital and all subjects gave informed consent to participate in the study.
STUDY DESIGN
This was a cross-sectional study. After clinical evaluation, spirometric testing, and chest radiography, induced sputum was collected before the investigative protocol to determine the cause of their dry cough was undertaken. At the time of sputum induction patients had been free of any respiratory tract infection for two months and had received no specific treatment for cough for at least six weeks.
SPUTUM INDUCTION AND PROCESSING
Sputum was induced and collected using the method previously described by Keatings et al.10Two ml of Hank’s balanced salt solution (HBSS) containing 1% dithiothreitol (DTT) (Sigma Chemicals, Poole, UK) were added to the sputum and the samples were vortexed and repeatedly aspirated through a small bore pipette until they were completely homogenised. The sputum volume was then recorded and further diluted with HBSS up to 10 ml, vortexed briefly, left at room temperature for five minutes, and centrifuged at 400g for 10 minutes at 4°C. The final concentration of DTT was 0.2%.
The sputum supernatants were kept at –70°C for subsequent cytokine assays and the cell pellets were resuspended. Total cell counts were performed on a haemocytometer using Kimura stain. Slides were then prepared using cytospin (Shandon, Runcorn, UK) and stained with a May-Grunwald-Giemsa stain for differential cell counts which were performed by an observer unaware of the clinical characteristics of the subjects. Specimens containing squamous epithelial cells of less than 50% of the total inflammatory cell number were considered adequate. At least 600 inflammatory cells were counted for each specimen. The reproducibility of the differential cell count in our laboratory showed an intra-class correlation coefficient of 0.75 for eosinophils, 0.78 for neutrophils, 0.76 for macrophages, and 0.56 for lymphocytes.
TNF-α ASSAY
Concentrations of TNF-α in the sputum supernatant were measured using an amplified sandwich enzyme linked immunosorbent assay as described previously.10 The detection limit of the assay was >8 pg/ml with 0.2% DTT included with the standard curve. The reproducibility of the measurement was acceptable with an intra-class correlation coefficient of 0.81.
INTERLEUKIN-8 ASSAY
IL-8 assay was performed using a commercially available kit from R&D (Abingdon, UK). With 0.2% DTT included with the standard curve the sensitivity limit of the assay was 125 pg/ml.
ANALYSIS OF DATA
Patient characteristics at baseline are expressed as mean (SE), and sputum data are expressed as median (interquartile range). Comparisons between groups were made using the unpairedt test or Mann-Whitney U test, as appropriate. Two tailed tests were performed with a p value of <0.05 being considered significant.
Results
PROFILE OF PATIENTS WITH CHRONIC DRY COUGH
All patients had a normal chest radiograph. Three patients were found to have asthma and were excluded from the analysis. The characteristics before treatment of the 19 patients with non-asthmatic chronic dry cough and the 10 healthy controls are summarised in table1. Four patients were diagnosed as having acid reflux, five post-nasal drip, and 10 idiopathic cough. Measurement of the cough response with capsaicin and low chloride solutions demonstrated an enhanced cough reflex in these patients compared with the normal volunteers.12
Characteristics of patients and controls
SPUTUM CHARACTERISTICS
All subjects produced an adequate sputum specimen. The inflammatory cell and cytokine profiles of the sputum samples are summarised in table 2. As there was only a small number of patients with gastro-oesophageal reflux and post-nasal drip, comparisons with normal subjects have been made of the whole group of patients with chronic dry cough (n = 19) and those with idiopathic cough (n = 10). There were no significant differences in terms of sputum volume between those with chronic cough and normal subjects. Patients with non-asthmatic chronic dry cough and idiopathic cough had similar total cell numbers but had a significantly higher proportion of neutrophils in induced sputum than normal controls (p = 0.001 (95% CI 11.3 to 42.2) for non-asthmatic chronic dry cough; p = 0.01 (95% CI 9.0 to 46.9) for idiopathic cough). There was a corresponding reduction in the percentage of macrophages in those with chronic cough.
Sputum characteristics in patients with chronic cough and normal controls
IL-8 AND TNF-α CONCENTRATIONS
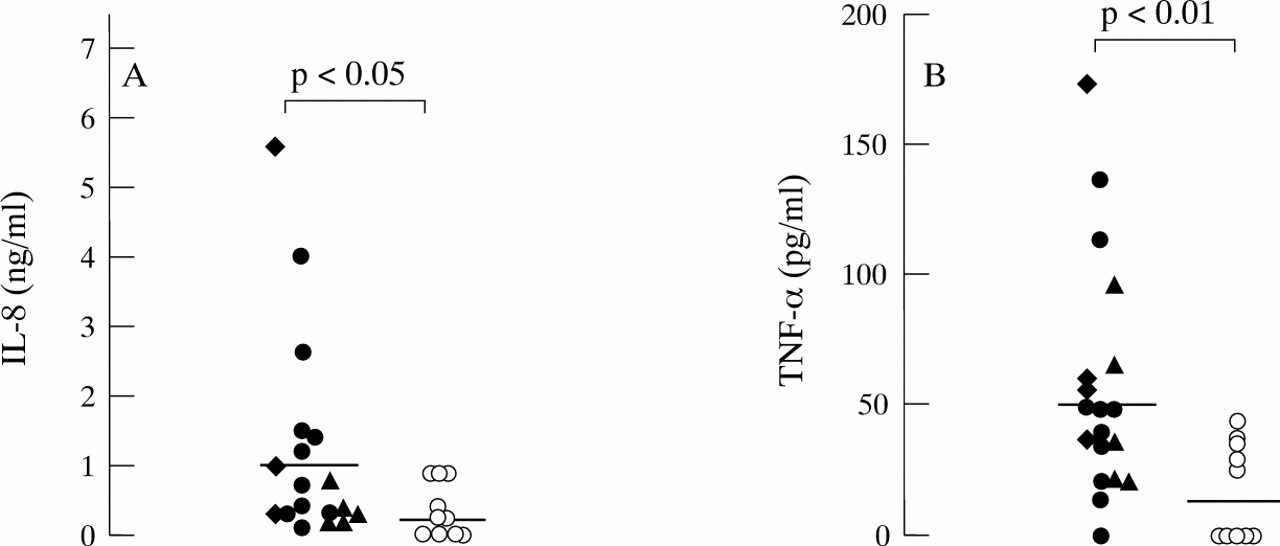
IL-8 and TNF-α concentrations were significantly increased in induced sputum samples from patients with non-asthmatic chronic dry cough compared with normal subjects (table 2, fig 1; p<0.05 (95% CI 0.05 to 1.60) for IL-8; p<0.01 (95% CI 8.8 to 69.8) for TNF-α). These increases were also seen in the patients with idiopathic cough (p<0.05 (95% CI 0.05 to 1.75) for IL-8; p<0.05 (95% CI 0.5 to 0.6) for TNF-α). There was no significant correlation between these cytokine levels and the percentage of neutrophils.

{kind=link}
Concentrations of (A) IL-8 and (B) TNF-α in induced sputum of patients with non-asthmatic chronic dry cough compared with normal controls. ● = idiopathic cough, ♦ = gastro-oesophageal reflux, ▴ = post-nasal drip, ○ = normal control. Horizontal bars represent median values.
Discussion
Analysis of induced sputum has revealed that there is an increase in the number of neutrophils of nearly twofold in patients with non-asthmatic chronic dry cough of all causes compared with normal subjects. In addition, the levels of TNF-α and IL-8, the two cytokines usually associated with neutrophils in terms of their production and effects, were significantly increased in induced sputum. This was also found in the subgroup of patients with idiopathic cough. Our results indicate that there is a predominant neutrophilic inflammation in the airways of patients with chronic dry cough, together with the release of neutrophil associated cytokines.
Evidence of airway inflammation in patients with a similar spectrum of cough has been previously reported.9 Bouletet al showed no consistent differences in the cellular constituents of bronchoalveolar lavage fluid in patients with non-asthmatic chronic dry cough but examination of bronchial biopsy specimens showed increased epithelial desquamation and mononuclear cells but no significant increase in neutrophils. The difference in the specimens studied may account for the discrepancy in the type of inflammatory cells found to be increased. For example, induced sputum may reflect events in the cellular and fluid phase portions of the proximal airways, while bronchoalveolar lavage fluid may reflect those of more peripheral airways and of the alveolar lining fluid and bronchial biopsy specimens may reflect the events in the bronchial mucosa of the larger airways. The sputum neutrophilia found in our patients with chronic cough is in agreement with the findings of a previous study.13
The profile of cells obtained in induced sputum from patients with chronic cough differs from that from patients with asthma in that there is an absence of eosinophilia. Smokers or patients with chronic obstructive pulmonary disease have an increased percentage of neutrophils in induced sputum10 but the patients in our study neither smoked nor had any evidence of airflow limitation.
The mechanism(s) underlying this inflammation are unclear. It is conceivable that acid reflux or post-nasal drip may induce neutrophilic inflammation of the airways by direct action of acid or inhaled sinonasal fluid into the airways. In an animal model sinusitis has been shown to cause hyperreactivity of the lower airways by post-nasal dripping of cells or cell products into the lower airway.14 It is not clear which mechanisms are responsible for the neutrophilia observed in idiopathic cough. We speculate that the act of repeated coughing itself may contribute to this inflammation, as sputum neutrophilia was consistently observed in all three sub-categories of patients with non-asthmatic cough. The mechanism for this potential effect, however, remains to be established. It may be postulated that epithelial damage induced by coughing may induce the release of inflammatory cytokines such as IL-8 and TNF-α. Both IL-8 and TNF-α can be produced by airway epithelial cells following inflammatory stimuli such as pro-inflammatory cytokines or exposure to allergen.15 ,16 Hypertonic saline to induce coughing and sputum itself may cause an increase in neutrophils in induced sputum.17 Furthermore, both cytokines when administered to the airways can induce neutrophilic inflammation.18 ,19 Neutrophils could also be important sources of IL-8 and TNF-α. Further studies are needed to determine the mechanism of neutrophilia in patients with chronic cough.
Irrespective of the mechanism of airway inflammation, it is possible that inflammation may perpetuate the dry cough by enhancing the cough reflex through the release of inflammatory mediators and cytokines. It is not known whether TNF-α or IL-8 can enhance cough reflex directly. However, other mediators that can be produced directly through the action of these cytokines, such as the release of prostaglandins (PGE2 or PGF2α) and bradykinin, can enhance the cough reflex,6-8
In summary, neutrophilic airway inflammation has been demonstrated in non-asthmatic patients with chronic dry cough, including those with idiopathic cough. It is not known whether the sputum neutrophilia observed in these patients will disappear with successful treatment. We conclude that sputum induction can be useful as a non-invasive method for studying airway inflammation in chronic dry cough. Neutrophils and associated cytokines may have a role in the pathogenesis of non-asthmatic chronic dry cough.
Acknowledgments
AJ was in receipt of a research fellowship from the Royal Thai Government, Thailand and UGL of a research fellowship from Boehringer Ingelheim, South Africa.