Article Text

Abstract
BACKGROUND A study was undertaken to determine whether swimming training improved aerobic capacity, exercise induced bronchoconstriction (EIB), and bronchial responsiveness to inhaled histamine in children with asthma.
METHODS Eight children with mild or moderate asthma participated in swimming training every day for six weeks. The intensity of training was individually determined and set at 125% of the child’s lactate threshold (LT), measured using a swimming ergometer. Another group of eight asthmatic children served as control subjects. Aerobic capacity and the degree of EIB were assessed by both cycle ergometer and swimming ergometer before and after swimming training.
RESULTS The mean (SD) aerobic capacity at LT increased by 0.26 (0.11) kp after training when assessed with the swimming ergometer and by 10.6 (4.5) W when assessed with the cycle ergometer, and these changes were significantly different from the control group. The mean (SD) maximum % fall in forced expiratory volume in one second (FEV1) to an exercise challenge (cycle ergometer) set at 175% of LT decreased from 38.7 (15.4)% before training to 17.9 (17.6)% after training, but with no significant difference from the control group. There was, however, no difference in histamine responsiveness when compared before and after the training period.
CONCLUSION A six week swimming training programme has a beneficial effect on aerobic capacity but not on histamine responsiveness in children with asthma.
- asthma
- swimming training
- exercise training
- children
- lactate threshold
- bronchial responsiveness
Statistics from Altmetric.com
Several studies have shown that asthmatic patients can improve their exercise performance after participating in one of a number of physical conditioning programmes.1-7 The role of swimming training is well accepted amongst the asthma community and is the form of exercise frequently prescribed for asthmatic children because it seems to precipitate asthma less than land based exercise.7-9 Although training programmes have been advocated to improve the physical working capacity and clinical symptoms of patients, the effect on exercise induced bronchoconstriction (EIB) remains controversial.10-13 The major problem with most previous studies has been the lack of individualisation of training,1 ,2 ,5 ,10 ,11 ,13 the same training being prescribed for all subjects. Thus, some subjects may have been understressed while others may have been exhausted. In addition, the training effect of the exercise programme has generally been assessed using an exercise test of the same intensity (absolute load) as that used before training. An exercise challenge is usually graded to produce an increase in heart rate to approximately 80% of the subject’s predicted maximum. If the training programme was successful and cardiorespiratory fitness was increased, one might expect that the same exercise load may have less effect on heart rate and on ventilation, which might translate into less EIB.3Thus, any true effect of exercise training on EIB may be masked.
The present study was undertaken to determine whether individualised swimming training improves aerobic capacity and whether this truly results in less EIB or whether the apparent protection from EIB is simply due to an increased exercise capacity. To individualise the training programme and to use the same load before and after training, each subject’s aerobic capacity was defined by calculating the work load at which lactic acid production increased (lactate threshold; LT). This LT was used to individualise the training programme and to determine the work loads used in the exercise challenges. To determine the specificity of the type of training programme each subject’s aerobic capacity was determined using both a swimming ergometer and a cycle ergometer before and after the swimming training programme. The effects of the swimming training programme were determined by exercise challenge tests using both the swimming and cyclic ergometers and a histamine challenge test.
Methods
SUBJECTS
Sixteen children with asthma diagnosed according to the ATS criteria14 who had been admitted to hospital for treatment participated in the study. All had severe asthma when admitted and the asthma attacks were controlled by treatment as an inpatient. None were prescribed oral steroids. The characteristics of the children are shown in table 1. They were randomly allocated to either a training group (n = 8) or a control group (n = 8). The two groups did not differ with respect to age, height, pulmonary function, or frequency of acute attacks of asthma. Asthma medication (disodium cromoglycate, β2 agonists, theophylline, beclomethasone dipropionate) was not modified during the study period. The study was performed during late autumn when allergic stimuli were minimal. All studies were performed when the children were free from symptoms of asthma or respiratory infections.
Demographic data and baseline pulmonary function of 16 asthmatic children
BASELINE ASSESSMENTS
Determination of aerobic capacity
To determine each child’s aerobic capacity, exercise tests were performed using a cyclic ergometer (Bosch Co.) and swimming ergometer (Ezaki Co. Japan) with an interval of one day between the tests. The incremental cyclic ergometer test started with 10–15 W for four minutes. The work load was then increased by 5–10 W every four minutes until exhaustion. The incremental swimming ergometer test was performed using a tethered swimming method in a heated (30°C) indoor pool. Subjects swam “crawl” for two minutes while their position was kept constant and a load was applied with a rope attached around their waist (fig 1). The work load was 0.1–0.2 kp initially and was increased gradually by 0.2 kp every two minutes until exhaustion. During both exercise tests the heart rate was monitored continuously by radiotelemetry.

Scheme of the swimming ergometer. Subjects swam “crawl” for two minutes while their position was kept constant and a load was applied with a rope attached around their waist.
To measure blood lactate concentrations 20 μl blood samples were obtained from an ear lobe at rest and immediately after each exercise increment. Blood was immediately haemolysed, diluted 10 times with 0.1 mM phosphate buffer (pH 7.3), and frozen. The concentration of lactate in these samples was determined using a commercial lactate analyser (Roche 646). The lactate threshold (LT) was calculated for each subject from a plot of blood lactate against work load (in watts). The initial break point in blood lactate concentration was determined by visual inspection. The mean value of the points determined by three observers was defined as the lactate threshold (fig 2). Aerobic capacity was defined as the work load at LT.
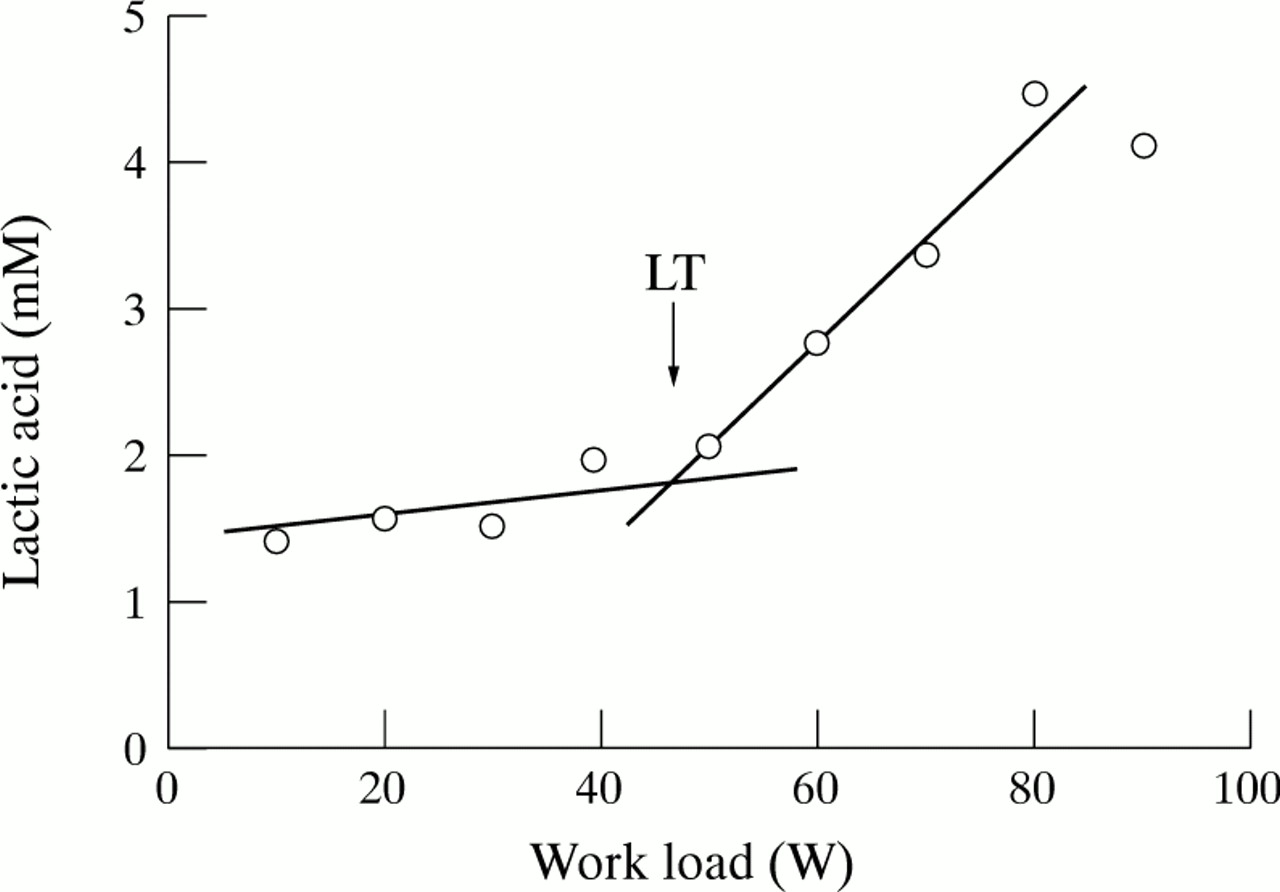
Determination of lactate threshold (LT) in a single subject from a plot of blood lactate levels against work load (in watts). The initial break point in blood lactate concentration was determined by visual inspection. The mean value of the points determined by three observers was defined as the LT.
Evaluation of exercise induced bronchoconstriction (EIB)
Exercise challenge tests were performed on consecutive days on both the cycle ergometer and the swimming ergometer using six minute challenge protocols. Work loads were set at 100% and 175% of the LT, determined as described above. There was an interval of at least 24 hours between each exercise test so as not to influence the refractory period of EIB. With the cycle ergometer subjects inhaled dry air at room temperature through a two way valve and mask. Challenge tests using the swimming ergometer were performed in a heated (30°C) indoor pool. Forced expiratory volume in one second (FEV1) was measured with an AS 300 spirometer (Minato Medical Science Co.) immediately before exercise and five and 15 minutes afterwards. EIB was expressed as the percentage fall from the pre-exercise value ((pre-exercise—lowest post-exercise/pre-exercise) × 100). Heart rate was monitored throughout the study. All medication was withheld for 12 hours before the investigation.
Histamine challenge test
To evaluate bronchial responsiveness a histamine challenge test was performed. Histamine aerosols were generated using a DeVilbiss 646 nebuliser. Following inhalation of phosphate buffer saline, doubling concentrations of histamine (from 20 μg/ml to 10 000 μg/ml) were inhaled. The challenge test was discontinued when FEV1 had fallen to 20% or more below the initial value. The provocative concentration (PC20) was calculated from the log concentration-response curve by linear interpolation of the last two points.
SWIMMING TRAINING PROGRAMME
Before commencing the training programme the work rate and corresponding heart rate at 125% of LT were assessed in each subject using the swimming ergometer. The heart rate was continuously monitored by radiometry and the swimming speed was regularly noted at this intensity in a series of 25 m “crawls”. It was therefore possible for subjects to control their swimming speed by being informed of the time taken to swim every 25 m. The training intensity was thus set to 125% of LT for each subject individually. During the six week training period the training group swam in a heated indoor pool (30°C) for two 15 minute periods on six days of the week. A 10 minute break was taken between the two periods. Once a week blood lactate concentrations and heart rate were measured in each subject after the first 15 minute period to ensure that the training intensity remained at 125% of the subject’s LT. The training intensity was increased where necessary.
POST-TRAINING EVALUATION
After the training period the aerobic capacity of the subjects in both the training and control groups was reassessed with both the cycle and swimming ergometers and LT was recalculated. Exercise challenge tests were then performed with loads of 100% and 175% of the original LT (designated as absolute load) and at 100% and 175% of the new LT (designated as relative load) using both the cycle and swimming ergometers. As there were no changes in the aerobic capacity of the subjects in the control group (see later), they performed tests at 100% and 175% of the original LT (absolute load) only. Histamine responsiveness was reassessed using a protocol identical to that used at baseline.
STATISTICAL ANALYSIS
All values are reported as group mean (SD). Pairedt tests were used to detect differences within a group—for example, pre-training and post-training effects. Unpaired t tests were used to detect differences between groups. Statistical significance was accepted at p<0.05.
Results
The duration of swimming training, the total distance achieved during swimming training, and the mean swimming distance per day for each subject in the training group are shown in table 2.
Duration of swimming training and distance achieved by subjects in the training group
EFFECT OF SWIMMING TRAINING ON AEROBIC CAPACITY
The swimming training programmes improved the aerobic capacity significantly in all subjects in the training group. In the training group the mean (SD) work load at LT assessed by the swimming ergometer increased by 0.26 (0.11) kp after training (p<0.001). In the control group the change in work load was 0.04 (0.14) kp, so the change was significantly higher in the training group than in the control group (mean difference 0.22 kp, 95% CI 0.085 to 0.355, p<0.005; fig 3). Similarly, the mean aerobic capacity by cycle ergometer increased significantly by 10.6 (4.5) W in the training group (p<0.001) and by 3.8 (5.2) W in the control group. The change was significantly higher in the training group than in the control group (mean difference 6.8 W, 95% CI 1.59 to 12.02, p<0.01; fig 4).

Mean (SD) changes in work load by swimming ergometer before and after training in training group (n = 8) and control group (n = 8).

Mean (SD) changes in work load by cycle ergometer before and after training in training group (n = 8) and control group (n = 8).
EFFECT OF SWIMMING TRAINING ON EIB
The degree of EIB was reduced in the training group after the training period when challenge tests were performed using the same relative load after training as before training (fig 5). The mean maximal percentage fall in FEV1 induced with the swimming ergometer work load set to 175% LT on the relative load decreased significantly in the training group from 15.4 (12.1)% before training to 4.1 (4.8)% after training (p<0.01). A similar pattern was observed at a work load of 100% LT but these changes did not reach significance. However, there were no significant differences between the change in the mean maximal percentage fall in FEV1 in the training and control groups by absolute load at 100% LT (p = 0.07) or at 175% LT (p = 0.20).

Mean (SD) changes in maximum % fall in forced expiratory volume in one second (FEV1) at 100% and 175% of lactate threshold (LT) by swimming ergometer before and after training in the training group (n = 8) and control group (n = 8).
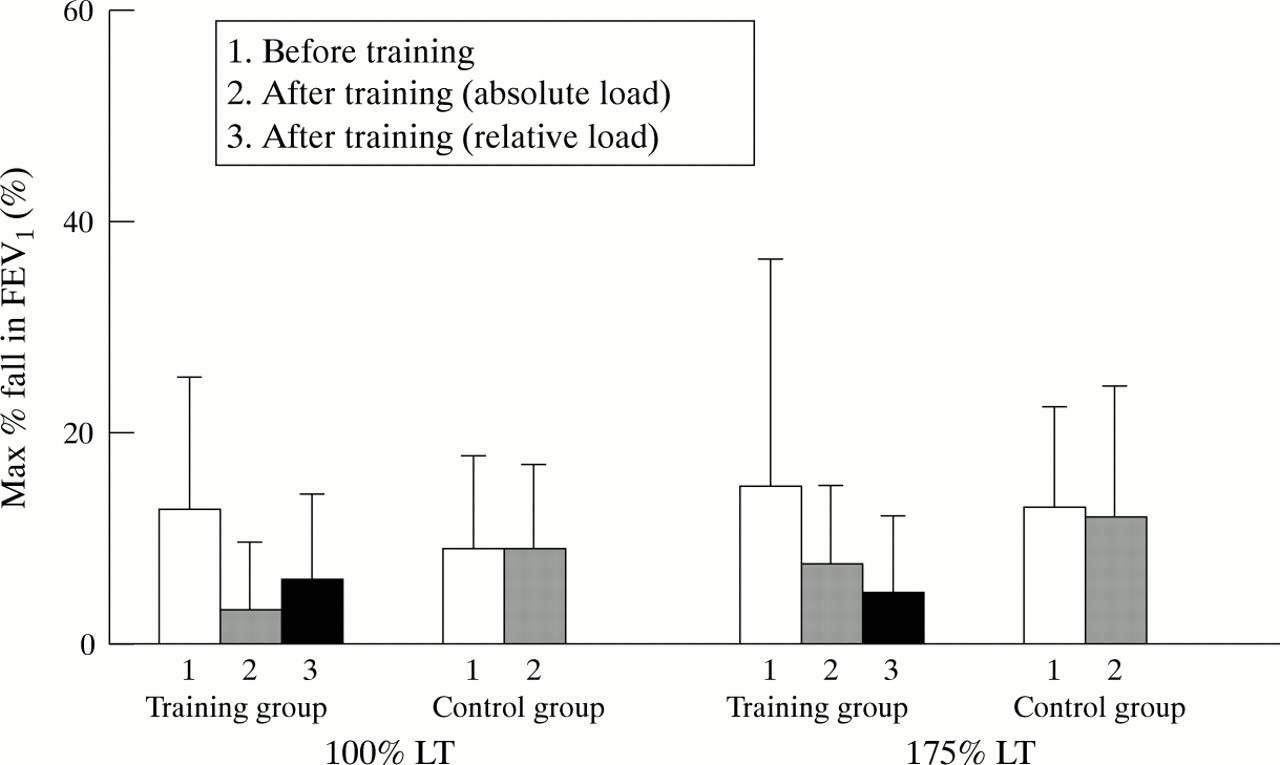
The falls in FEV1 induced by the cycle ergometer were greater than those induced by the swimming ergometer at both work loads. A greater fall in lung function was also induced by the higher work load (fig 6). The protective effects of training on EIB were evident when assessed with a relative load of 175% LT (38.7 (13.4)% fall in FEV1 before training vs 22.5 (14.7)% after training; p<0.05). When using the pre-training absolute load protective effects were seen at both 100% LT (p<0.05) and 175% LT (p<0.01). However, there were no significant differences between the change in the mean maximal percentage fall in FEV1 in either group when assessed by absolute load at 100% LT (p = 0.14) or 175% LT (p = 0.22).

Mean (SD) changes in maximum % fall in forced expiratory volume in one second (FEV1) at 100% and 175% of lactate threshold (LT) by cycle ergometer before and after training in the training group (n = 8) and control group (n = 8).
EFFECT OF SWIMMING TRAINING ON HISTAMINE RESPONSIVENESS
No changes were seen in histamine PC20 during the training period in either the training group or the control group (fig7). The difference between the mean change in PC20 in the training and control groups was not statistically significant (p = 0.16).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in individual concentrations of histamine required to provoke a fall in forced expiratory volume in one second of 20% or more (PC20) before and after training in training and control groups. No significant differences were found before and after training in the two groups.
Discussion
The results of this study show the benefits that can be achieved by an individualised training programme in asthmatic children. By setting training intensity to 125% of each child’s aerobic capacity and increasing the intensity weekly to ensure that it remained at this level, we have been able to increase each subject’s aerobic capacity. This resulted in a decrease in EIB when assessed at the same relative load before and after the training period. The benefits of swimming training were not confined to swimming exercise but were also seen when exercising on a cycle ergometer. However, increasing aerobic capacity by training did not decrease histamine responsiveness.
Several previous studies have attempted to address the benefits of training on asthmatic children. Some of these showed an increased aerobic capacity, whereas the reported effects on EIB have been more variable.10-13 The differences between the clear cut results of the present study and the variable results reported previously may be explained by methodological differences including differences in the selection of patients, the lack of a control group, differences in the training programme, and differences in the evaluation of EIB. No study has previously used an individualised training programme, nor continually reassessed the training intensity during the programme. We used the individual’s LT to determine an individualised work intensity as this has previously been reported to be a useful parameter for determining exercise intensity.15 ,16 Some previous studies have used heart rate to determine the work intensity used.4 ,6 ,12However, heart rate has been reported to have a large inter-individual variability, especially in children,17 making it unsuitable for individualising a training programme. Varrayet al reported the use of a ventilatory threshold to individualise training intensity for a swimming programme for asthmatic children.3 However, their protocol is time consuming and needs special apparatus and techniques which may limit its general applicability.16
We set the intensity of our training programme at 125% of LT, determined from an incremental swimming ergometer test. A work load of 125% LT was chosen for the following reasons. The degree of EIB depends upon the quantity of water loss from the airways as a result of the hyperventilation induced by exercise.18 ,19 High intensity training is therefore likely to induce EIB, especially in severe or unstable asthmatic subjects. A training intensity of 125% LT is less likely to induce significant EIB yet, as shown by our results, it is sufficient to achieve increases in aerobic capacity. Our subjects did not use premedication before training and could do the swimming training without the appearance of EIB.
Swimming is a recommended sport for asthmatic children because it does not induce as much EIB as other forms of exercise. However, there are few reports on the effects of endurance swimming training on EIB. In 1976 Fitch et al 13 reported that the subjective symptoms of asthma in children improved after one year of swimming training even though lung function and EIB did not improve. Svenonius et al 11reported that EIB was significantly improved after endurance swimming training in asthmatic patients. They used the same absolute exercise challenge intensity before and after training. Thus, the reports of an improvement in EIB may be due to the reduction in minute ventilation in response to a standard work load following a training programme which increased cardiorespiratory fitness. As the degree of EIB depends upon the minute ventilation achieved during exercise, less EIB would result. In the present study it may not be sufficient to use the LT to express the cardiopulmonary fitness rather than the minute ventilation to evaluate the degree of EIB. We showed that EIB decreased not only when assessed using the same absolute load before and after training, but also when the same relative loads were used. The benefits of training are therefore not simply due to an increase in cardiorespiratory fitness.
In an attempt to investigate the mechanism by which swimming training protected against EIB, we performed histamine challenge tests before and after training. Anderton et al 20 showed the close correlation between the PC20 by histamine challenge test and exercise challenge test. However, no significant changes in histamine PC20were seen in either the training or control groups in this study. The possibility exists that the true result was missed because of the small sample size. Martin et al 21have reported that the children who lose their asthma symptoms and no longer exhibit EIB often retain their bronchial hypersensitivity to histamine. There is generally a closer relationship between clinical asthma and EIB than between clinical asthma and the results of a histamine challenge.
The mechanism by which swimming training protects against EIB is not clear. While EIB is thought to be triggered by a change in the osmolarity of the airway lining fluid brought about by loss of heat and water to the inspired air,18 ,19 ,22 the exact mechanism remains unknown. The release of mediators from mucosal mast cells is thought to be involved,23 ,24 and leukotrienes may also play a part.25 ,26 Whether long term training can influence the release of these mediators is not known. However, short term anaerobic exercise has been reported to induce a rapid increase in plasma catecholamine levels and an increase in the density of lymphocytic adrenoreceptors.27 The β adrenoreceptor system has been shown to be activated in lymphocytes during prolonged aerobic exercise.28 Although these mechanisms may be important, we did not have the opportunity to study them in our study population.
In conclusion, the individualised swimming training used in the present study resulted in improved aerobic capacity and protected against EIB. This was true whether assessed with a swimming ergometer or a cycle ergometer. This protection against EIB was not accompanied by a decrease in histamine responsiveness. The use of an individualised training programme should prove to be a useful addition to treatment in asthmatic children.
Acknowledgments
This study was supported by the Pollution-related Health Damage Compensation and Prevention Association of Japan.