Article Text

Abstract
Background: Immunological ex vivo assays to diagnose tuberculosis (TB) have great potential but have largely been blood-based and poorly evaluated in active TB. Lung sampling enables combined microbiological and immunological testing and uses higher frequency antigen-specific responses than in blood.
Methods: A prospective evaluation was undertaken of a flow cytometric assay measuring the percentage of interferon-γ synthetic CD4+ lymphocytes following stimulation with purified protein derivative of Mycobacterium tuberculosis (PPD) in bronchoalveolar lavage fluid from 250 sputum smear-negative individuals with possible TB. A positive assay was defined as >1.5%.
Results: Of those who underwent lavage and were diagnosed with active TB, 95% (106/111) had a positive immunoassay (95% CI 89% to 98%). In 139 individuals deemed not to have active TB, 105 (76%) were immunoassay negative (95% CI 68% to 82%). Of the remaining 24% (34 cases) with a positive immunoassay, a substantial proportion had evidence of untreated TB; in two of these active TB was subsequently diagnosed. Assay performance was unaffected by HIV status, disease site or BCG vaccination. In culture-positive pulmonary cases, response to PPD was more sensitive than nucleic acid amplification testing (94% vs 73%). The use of early secretory antigen target-6 (ESAT-6) responses in 71 subjects was no better than PPD, and 19% of those with culture-confirmed TB and a positive PPD immunoassay had no detectable response to ESAT-6.
Conclusions: These findings suggest that lung-orientated immunological investigation is a potentially powerful tool in diagnosing individuals with sputum smear-negative active TB, regardless of HIV serostatus.
Statistics from Altmetric.com
Koch first used immune reactivity to aid tuberculosis (TB) diagnosis in the enduring form of the tuberculin skin test (TST).1 Assays measuring interferon-γ (IFNγ) production from blood in response to TB antigens have recently begun to supersede TST in diagnosing latent TB.2 3 Their value in advanced HIV and in unselected cases with active TB remains to be established.4 Furthermore, a blood-based approach cannot be combined with current microbiological techniques which require samples from the site of disease.
TB is spread primarily by inhalation of organisms into the lung, and this is reflected immunologically by the lung-compartmentalised TB antigen-specific responses that have been observed in TST-positive healthy household contacts of TB and individuals with active TB.5–7 Small clinical studies using bronchoalveolar lavage (BAL) have suggested that these phenomena may be used in a clinical setting to make a rapid diagnosis in cases of extrapulmonary and HIV-related TB with greater sensitivity than if blood was used.8–10 We therefore sought to determine the diagnostic utility of our approach in all patients at our centre in whom TB was felt to be a possible diagnosis and who were investigated by means of clinically indicated BAL.
METHODS
Patients and samples
The study was approved by the Royal Free Hospital ethics committee. All sputum smear-negative adults in whom TB was felt to be a possible diagnosis and who were undergoing a clinically indicated BAL were eligible for inclusion. No subject had commenced antituberculosis medication at the time of BAL. Subjects were recruited from outpatient clinics and inpatient wards of our urban teaching hospital between January 2001 and December 2005.
Historically, Bacillus Calmette Guerin (BCG) vaccination was routinely administered in the UK and the recorded rate among the combined native and foreign-born adult population seen in our service remains consistently around 80%.
BAL was performed on the basis of clinical indication as determined by the physician responsible for patient care. A standard technique was used in which a flexible bronchoscope was wedged into a subsegmental bronchus. Aliquots of normal saline to a total volume of 180 ml were introduced into an area of lung showing possible disease on radiological examination or the right middle lobe.
Immunological investigation
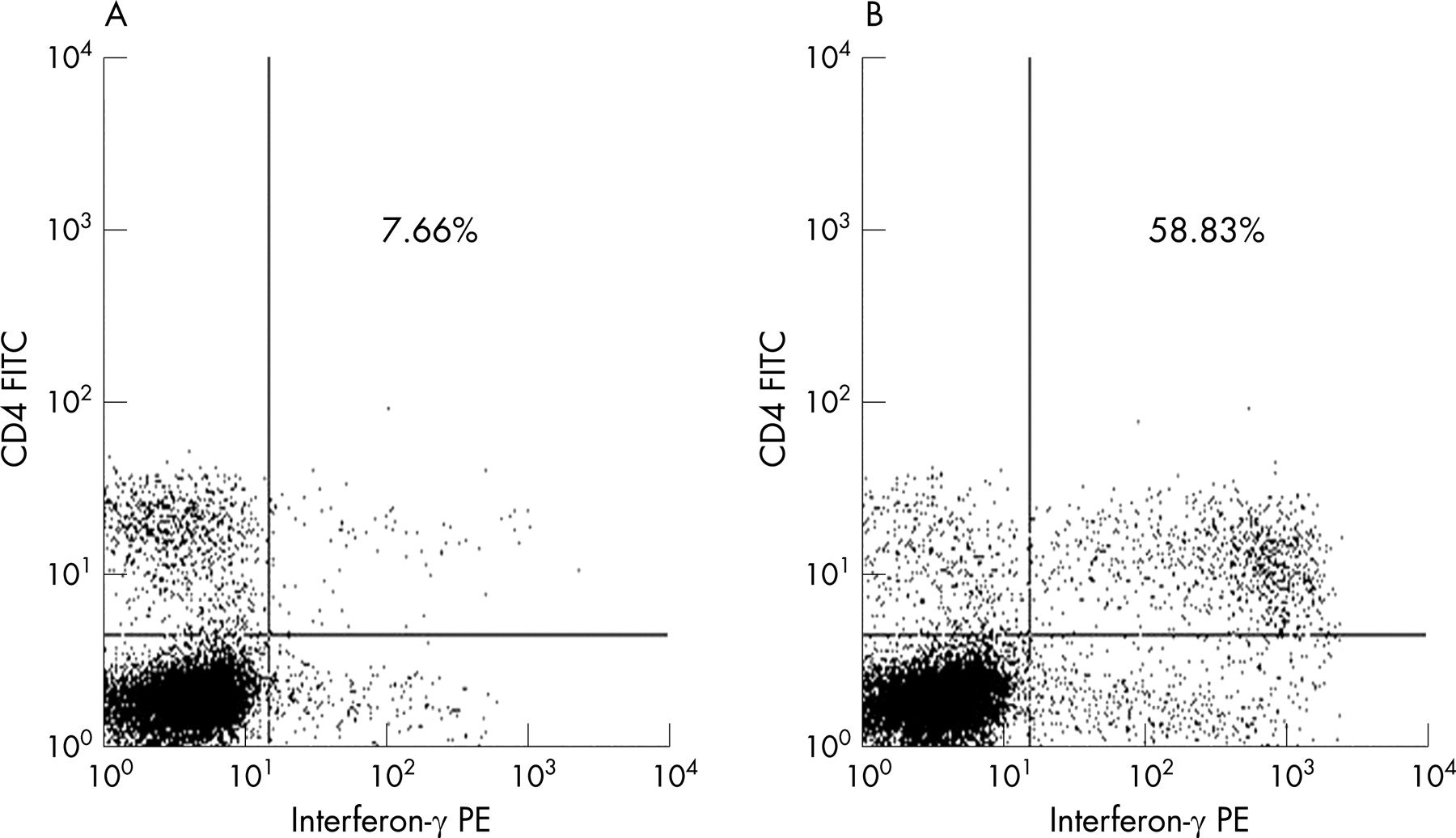
BAL fluid was processed within 2 h and aliquots sent for routine investigation; 10–20 ml were retained for this study. Absolute CD45+ leucocyte and lymphocyte numbers and the percentages of CD3+, CD4+ and CD8+ T cells were assessed by flow cytometry.11 Detection of antigen-specific IFNγ synthesis following incubation for 16 h (overnight) was performed as previously described.8 In brief, 5×104 CD4 lymphocytes were incubated with tissue culture medium (TCM) alone (negative control); TCM containing 10 μg purified protein derivative of Mycobacterium tuberculosis (PPD) (Mycos Research, Colorado, USA); or TCM containing 10 μg recombinant early secretory antigen target-6 (ESAT-6) (Colorado State University). Brefeldin A (Sigma) was added after 2 h. Harvested cells were fixed and permeabilised (Fix-and-Perm; An-der-Grub) and then stained for expression of CD3, CD4 and IFNγ at 4°C for 20 min. Stained lymphocytes, identified by flow cytometry scatter, were gated according to CD3 expression to produce a histogram of IFNγ producing CD4+ and CD4− T cells. The frequency of IFNγ+ CD4+ lymphocytes as a percentage of the total CD4+ T lymphocyte population (%CD4+IFNγ+) was determined (fig 1). The value observed in the negative control was subtracted from that in the PPD-stimulated culture to give a percentage value of PPD-specific CD4+ IFNγ+ lymphocytes (%PPD+CD4+IFNγ+).

Microbiological diagnosis
Following decontamination and concentration by centrifugation at 3000 g for 30 min, BAL specimens were divided. Aliquots were prepared for microscopy and direct nucleic acid amplification testing (NAAT) using the BD Probetec ctb assay (TB-SDA).12 The remainder was washed, centrifuged again and then inoculated into the MB BacT ALERT liquid culture system (bioMérieux UK, Hampshire, UK). Microscopy smears were stained with auramine-O and the positive smears were confirmed using a Ziehl-Neelsen stain. The isolate was confirmed as M tuberculosis by the regional Mycobacterial Reference Laboratory.
Diagnostic definition
A diagnosis of TB was accepted if (1) M tuberculosis was cultured or (2) if a clinical diagnosis was made, there was good evidence for this based on radiology or histology with an appropriate response to treatment. Diagnostic decisions were made without reference to immunological data.
Statistical assessment
Comparisons between groups were made using the Wilcoxon test; 95% confidence intervals (CI) were calculated using the exact Wilson method. The data were analysed using SAS Version 8.2 (SAS Institute Inc, Cary, NC, USA).
RESULTS
Patient information
Two hundred and fifty individuals of median age 40 years (range 19–64) underwent BAL; 41% were Black, 35% Caucasian, 21% Asian and 3% others. Sixty-three (25%) were HIV-infected with a median blood CD4 count of 153 cells/μl (range 5–1065).
In total, 111 of the 250 individuals (44%) had a diagnosis of active TB of whom 21% (n = 23) were co-infected with HIV (median blood CD4 count 153 cells/μl (range 10–1065)). Eighty-three of the 111 (75%) were culture positive (73 from the same sample as used for immunology; 10 from a sample other than BAL fluid) and 28 (25%) received a clinical diagnosis of active TB. Of the 139 (56%) in whom active TB was not diagnosed, the commonest alternative definitive diagnosis in those not infected with HIV was sarcoidosis (22/100), and in those infected with HIV Pneumocystis jirovecii pneumonia (12/39) was the most common alternative diagnosis.
In the total group, the median percentage of CD45+ BAL leucocytes that were lymphocytes was 23.2% (range 1.2–85.2). Among the CD3+ lymphocytes, the ratio of CD4+ to CD8+ lymphocytes (CD4:CD8) was 1.25 (range 0.01–44.10).
PPD-specific IFNγ responses in the lung compared with the final diagnosis
In the TB group the median percentage of PPD-specific CD4+IFNγ synthetic lymphocytes (%PPD+CD4+IFNγ+) was 14.63% (range 0–79.11) for those with culture-proven TB and 10.41% (range 0.19–70.50) for those with clinical diagnoses (p = 0.36) compared with 0.21% (range 0–27.10) in the non-TB group (p<0.001). HIV infection did not significantly alter these values (HIV/TB: 8.89% (range 0–61.04); TB alone: 14.63% (range 0.12–79.11), p = 0.24).
PPD-specific lung immunoassay as a diagnostic tool
Using a receiver operator characteristic (ROC) curve (area under the curve = 0.908), we assessed that a %PPD+CD4+IFNγ+ value of 1.5% would provide a simple and appropriate assay cut-off value (fig 2). The sensitivity of a %PPD+CD4+IFNγ+ value of ⩾1.5% for a diagnosis of active TB was 95% (95% CI 89% to 98%) and the specificity was 76% (95% CI 68% to 82%; table 1).

{kind=link}
{kind=link}
A %PPD+CD4+IFNγ+ value of ⩾1.5% was observed in 95% (79/83) with culture-positive TB and 93% (26/28) who received a clinical diagnosis of active TB. These values were 95% (90/95) in subjects with pulmonary TB and 100% (16/16) in whom the active disease site was felt in the end to be non-pulmonary.
PPD-specific immunoassay versus nucleic acid amplification test (NAAT) in BAL
The immunoassay was compared with a NAAT in 67 cases in which M tuberculosis was grown from BAL fluid. This ensured that TB DNA was present for amplification. Both the TB-SDA and the immune-based test were highly sensitive in smear-positive BAL fluid (table 2). However, unlike the TB-SDA, the performance of the immune test was maintained when the smear was negative. The results of this comparison and further analysis according to whether the BAL fluid was acid and alcohol fast bacilli (AAFB) smear negative or positive are also shown in table 2.
PPD-specific IFNγ responses in the lung discordant with final diagnosis
Six of 111 individuals (5%) who received a final diagnosis of TB had an observed %PPD+CD4+IFNγ+ value of <1.5%. No consistent pattern of disease was observed in this group; and one had a %PPD+CD4+IFNγ+ value of 12.25% observed in pleural fluid.
Thirty-four of 139 individuals (24%) not diagnosed with TB had a positive immunoassay. Of these 11 were of Asian ethnicity (all born outside the UK), 11 were Black (all born outside the UK), 12 were Caucasian (8 with risk factors for TB due to either drug or alcohol use, occupation, country of birth or known contact with an index case). Four of 34 had mycobacteria other than tuberculosis (MOTT) cultured from BAL fluid (1 grew M fortuitum but with a positive NAAT for M tuberculosis; 1 grew M kansasii; 2 grew M avium complex, 1 with a positive NAAT for M tuberculosis). Only 1 individual had definitely received a previous course of antituberculosis therapy. During a median follow-up period of 33 months (range 12–67), 2/34 subjects (6%) developed active TB (diagnosed 12 and 23 months after initial BAL, respectively). These subjects are further described in table 3.
ESAT-6-specific IFNγ responses in the lung versus final diagnosis
Seventy-one consecutive individuals from the BAL study population had samples stimulated with recombinant ESAT-6 in addition to PPD. Of these, 32 (45%) were diagnosed with active TB (27 culture proven and 5 clinical). The median (range) percentage of ESAT-6-specific CD4+IFNγ synthetic lymphocytes in these 32 subjects was 1.02% (0–12.39). No significant difference was seen between individuals with culture proven or clinically diagnosed TB and those who had a positive PPD immunoassay but were not diagnosed with TB (1.28% (0–12.39) vs 0.78% (0.19–6.24) vs 0.72% (0–3.88), respectively). In the TB culture positive group, 5/27 (19%) had no measurable response to ESAT-6 despite all 5 having a positive PPD immunoassay.
DISCUSSION
These results demonstrate the potential of a lung-orientated immunological approach to the diagnosis of active TB using BAL and flow cytometry in a large unselected series. Unlike current blood-based immunoassays, BAL may also provide microbiological confirmation of the rapid immunological test results. In 250 sputum smear-negative individuals in whom TB was considered to be a possible diagnosis, the PPD-based IFNγ immune assay had a sensitivity of 95% and specificity of 76%, with comparable utility in subjects with and without HIV infection and in those with pulmonary and non-pulmonary TB.
Our immunological approach had markedly superior overall sensitivity compared with a commercially available NAAT representative of current rapid microbiological diagnostics. In particular, our immunoassay showed no diminution in performance with BAL smear-negative culture-positive cases, suggesting significant advantages for immunological assays when there is a lower mycobacterial burden or minimal pulmonary disease. This agrees with the limited data available on the value of molecular techniques in such cases.13 14
A significant drawback of the tuberculin skin test is that positive responses are often generated by Bacille-Calmette-Guerin (BCG) vaccinated individuals with no exposure to M tuberculosis.15 This has prompted the use of antigens encoded in the region of difference 1 (RD1) portion of the genome of M tuberculosis such as ESAT-6 which are absent in BCG strains.16 17 We found that ESAT-6 provided no further information than PPD lymphocyte stimulation. Furthermore, in our largely BCG-vaccinated population, responses to PPD in the lung due to BCG were not detectable. The most plausible explanation is that BCG-specific memory lymphocytes traffic through blood and home to the skin while avoiding the lung.18
We did observe a significant number of positive tests in subjects not clinically felt to have active TB. We believe that a substantial proportion of these subjects in fact had good evidence for TB infection (as detailed in table 3), if not current active disease. Given the similar finding with both PPD and ESAT-6, it is probable that all of the current mycobacterial antigens used in TB diagnostics will exhibit these characteristics.10 Do these responses therefore have clinical value? It is likely that they are genuinely directed against mycobacteria, some of which are perhaps environmental. However, they may also signify the presence of undetected TB infection with viable organisms, and therefore a risk of later reactivation.19 It is noteworthy that, during follow-up of the 34 individuals with such positive results, 2 have developed active TB. The reported poor specificity of immune-based methods must therefore be judged against the inadequacies of both clinical evaluation and other diagnostic techniques.20
An important feature of our approach is that the assay had comparable performance in patients with and without HIV co-infection, as well as those with non-pulmonary or pulmonary disease. Lymphocyte recirculation to the original site of TB infection (usually the lung), regardless of subsequent disease manifestation, may explain why we can detect non-pulmonary TB using lung-based assays. Given the difficulties that exist in diagnosing TB outside the lung, we feel that this test with its high sensitivity, if used within a suitable clinical pathway, might reduce the need for multiple investigative procedures by “ruling out” TB at an early stage.
Our data strongly suggest that immunological assays, which can be combined with conventional culture and NAAT in BAL samples, have the potential to improve the diagnosis of patients with suspected TB. Simplification of sample collection and processing would enable this technique to be applied beyond its current research setting.
Acknowledgments
Recombinant ESAT-6 was kindly provided as part of NIH NIAID Contract No. HHSN266200400091C entitled “Tuberculosis Vaccine Testing and Research Materials” which was awarded to Colorado State University.
REFERENCES
Footnotes
Funding: None
Competing interests: None