Article Text

Abstract
Background: Universal testing for HIV in patients with tuberculosis (TB) has been advocated for over a decade. The aim of this study was to describe the prevalence and testing practices of HIV in TB centres in London.
Methods: A cohort study was undertaken of all patients with TB in Greater London in 2003–4 (n = 1941). Logistic regression was used to assess factors affecting being offered and accepting testing and having a positive HIV result.
Results: The overall known prevalence of HIV was 9.9% (193/1941). In those with a test result (including those diagnosed previously) it was 25.6%. Overall, 50.8% of patients aged ⩾20 years without previous testing were offered HIV testing and, of these, 73% accepted. In multivariable analysis, factors associated with being HIV positive were age 20–49 years, black ethnicity and being born overseas. Those with smear-negative disease and with a poor understanding of English were significantly less likely to be offered HIV testing. Factors associated with refusal of an offered test were female gender or age >49 years. HIV status was not associated with smear status, drug resistance or death, but was associated with CNS disease (OR 1.8, 95% CI 1.0 to 3.0, p = 0.003).
Conclusions: Nearly half the patients with TB in London in 2003–4 were not offered HIV testing. In those offered testing, uptake was high. Patients in higher risk groups were more likely to be offered testing but, even within the highest risk groups, testing was not universally offered. This represents a missed opportunity for diagnosing HIV in patients with TB in London.
Statistics from Altmetric.com
The natural histories of HIV and Mycobacterium tuberculosis (TB) infection are interlinked, and the global HIV epidemic has had a dramatic impact on rates of TB infection.1 2 3 In HIV-infected individuals, active TB is caused by reactivation of endogenous latent disease as well as re-infection with a new strain and is estimated to account for 9% of all new cases of TB worldwide.1 HIV is the strongest known risk factor for reactivation of latent TB to active disease with a risk of reactivation of approximately 10% per year.4 In 2004, 15% of deaths that occurred as a result of TB were in HIV-infected individuals.1
The incidence of TB in London has doubled over the past decade and was estimated at 41.3/100 000 in 2003.5 Much of the increase is thought to be fuelled by migration from areas of high prevalence for HIV and TB, and the burden of disease remains concentrated in urban areas and in high-risk groups. Previous linkage of TB and HIV databases estimated that 5.7% of TB cases in England and Wales in 2003 were co-infected with HIV;6 however, the true prevalence of HIV/TB co-infection is unknown.
TB is an AIDS-defining illness and often occurs at higher levels of immune functioning in HIV-positive patients than other AIDS-defining illnesses.3 Any patient with TB not offered an HIV test is a missed opportunity for testing undiagnosed HIV-infected patients, but there are few non-surveillance data on the proportion of patients with TB who are offered an HIV test in low prevalence countries and the factors associated with being offered and accepting an HIV test.
The aim of our study was to measure the prevalence of HIV in patients with TB in London in 2003–4, the proportion of patients with TB offered a test and the factors associated with accepting an HIV test if offered.
Methods
The methods of this study have been published previously.7 A cohort study was undertaken in patients with TB known to TB services on 1 July 2003 in Greater London (n = 1995). Eligible patients were identified from the London TB register and local clinic records. Data were collected for 97% of eligible patients (1941/1995) from case notes and other clinical records by case managers for patients on TB treatment or who should have been on TB treatment at baseline and then 12 months later on 1 July 2004. Cases subsequently found not to have TB were excluded from the analysis. Only anonymised information left the TB clinics.
Data collected at baseline and at 12 months included information on risk factors for TB, age, sex, ethnicity, clinical presentation of disease, resistance data (rifampicin or isoniazid resistance), compliance with treatment, date of arrival in UK, country of birth, level of spoken English, socioeconomic data (housing status) and whether directly observed therapy was required. Information on HIV testing was obtained from the case notes and TB records on whether an HIV test was offered, whether the offered HIV test was accepted, the HIV test result if known and whether the patient had been previously diagnosed with HIV before the TB diagnosis and whether he/she was on antiretroviral therapy (ART) at the time of TB diagnosis.
Denominator data on size of UK populations at risk were obtained from published sources.7 In the case of HIV this was from the Survey of Prevalent HIV Infections Diagnosed (SOPHID) database which is a cross-sectional survey of all individuals with diagnosed HIV infection who attend for HIV-related care within the NHS in England, Wales and Northern Ireland within a calendar year.
Poisson distribution was used to calculate TB prevalence and 95% confidence intervals per 100 000 population on 1 July 2003 for HIV-positive populations and other risk groups. Logistic regression analyses were used to assess factors associated with being HIV positive, factors associated with being offered an HIV test and, in those who were offered a test, factors associated with accepting the test. Unadjusted and multivariable analyses were performed where all variables were included in the multivariable models. Statistical analyses were performed using Stata statistical software Version 10.0 (StataCorp, College Station, Texas, USA). All reported p values are two-sided and a p value <0.05 was considered to be significant.
Results
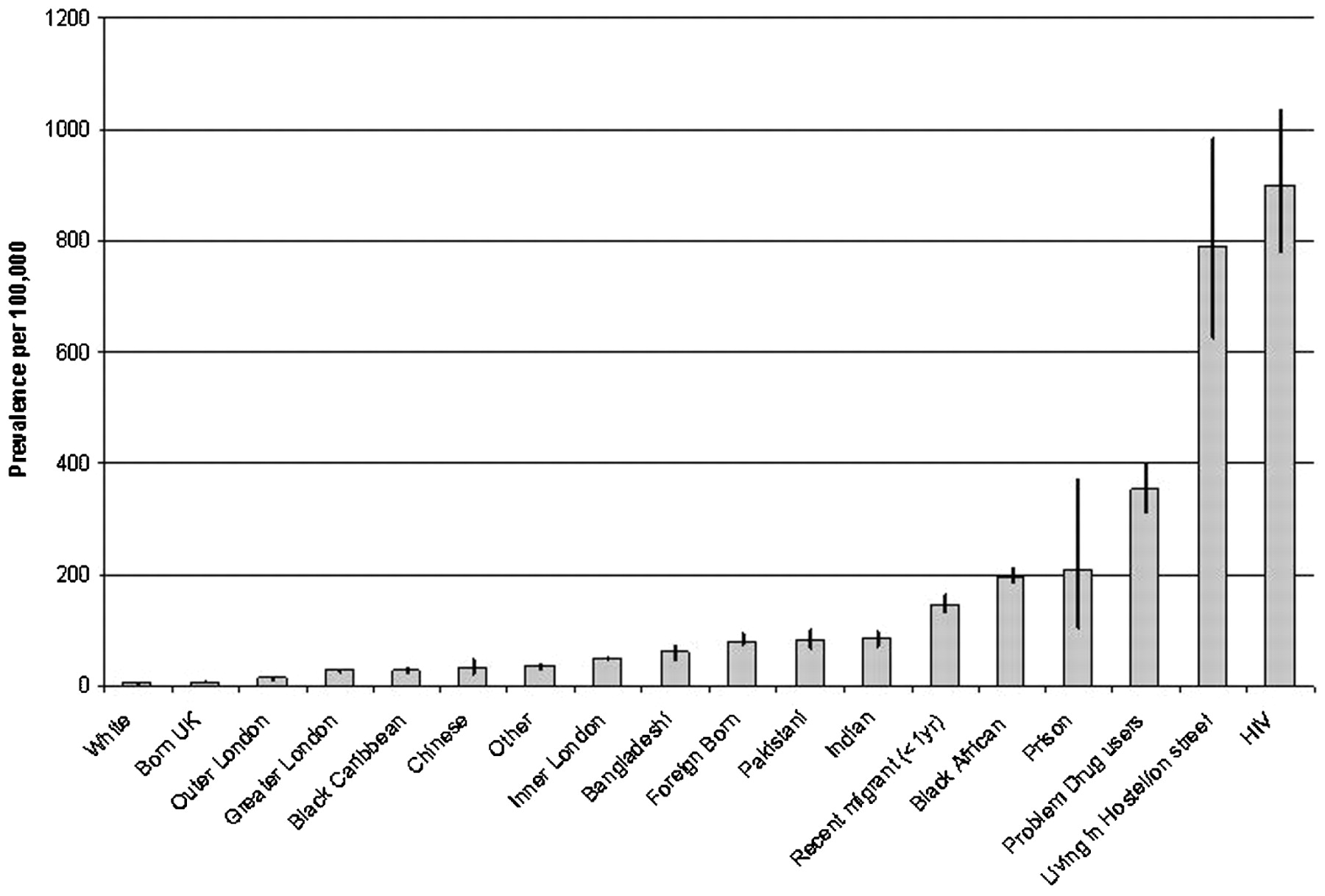
A total of 1995 patients were identified giving an overall prevalence of TB of 27.1 per 100 000; however, this varied considerably by risk group. The highest observed prevalence was in those who were HIV positive (877.8 per 100 000 (95% CI 756.8 to 1012.6); fig 1). The prevalence of TB per 100 000 and 95% CI for other population groups are shown for comparison and were published in the original study paper.7

Prevalence of tuberculosis in different groups in London (95% confidence intervals).
From the 1941 eligible patients for whom data were available, 193 (9.9%) were identified as HIV-positive (88 had a positive test at the time of TB diagnosis and 87 had a previously positive test without a repeat test; 18 patients tested positive at the time of TB diagnosis even though they had tested positive previously). This is likely to be an underestimate of the number of HIV-positive individuals as, of those unaware of their HIV status at TB diagnosis (n = 1836), only 48.2% (n = 884) were offered HIV testing. The prevalence of HIV in those with a test result (including those with a previous diagnosis) was 25.6% (193/755).
In unadjusted analysis, TB/HIV co-infected patients were significantly younger than those who were not co-infected (93% of co-infected patients were aged 20–49 years compared with 68% of those not co-infected; p<0.0001). Co-infected patients were more likely to be female (52% vs 43% (OR 1.43, 95% CI 1.06 to 1.94, p = 0.02)) and more likely to have been born overseas (90% vs 77% HIV-negative (OR 2.65, 95% CI 2.60 to 4.38, p<0.0001)) than patients who were not co-infected, with 80% born in subSaharan Africa compared with 49% HIV-negative individuals (OR 7.57, 95% CI 4.8 to 11.8, p<0.001), reflecting the epidemiology of HIV and TB in their countries of birth. They were also a vulnerable population with 15% having active asylum applications compared with 7% of those who were HIV-negative and were more likely to be unemployed (OR 1.78, 95% CI 1.29 to 2.39, p<0.001). In terms of disease presentation, co-infected patients were more likely to present with CNS disease (OR 1.75, 95% CI 1.02 to 3.02, p = 0.003), but were not more likely to have sputum smear-positive pulmonary disease (20.7% vs 19.5%, p = 0.69), drug-resistant disease (9.7% vs 11.9%, p = 0.403), require DOT (4.5% vs 7.3%, p = 0.09) or have poorer outcomes including death (1.7% vs 0.93%, p = 0.334) than those who were HIV-negative.
After adjustments in a multivariable analysis, factors significantly associated with being HIV positive were age (OR 2.29; 95% CI 1.48 to 3.54 for those aged 30–39 years compared with age 20–29 years and OR 2.30; 95% CI 1.34 to 3.95 for those aged 40–49 years compared with 20–29 years), black African ethnicity and being born overseas (table 1).
Characteristics of all 1941 patients with tuberculosis (TB) in London according to HIV status
In spite of current guidance, not all patients were offered an HIV test at the time of their TB diagnosis or within 12 months of follow-up. In those unaware of their HIV status at TB diagnosis (n = 1836), only 48.2% (n = 884) were offered HIV testing. On multivariable analysis the following were significantly more likely to be offered HIV testing: those aged 20–49 years (OR 0.49, 95% CI 0.32 to 0.74 for those aged 50–59 years compared with 20–29 years and OR 0.35, 95% CI 0.23 to 0.53 for those aged ⩾60 years compared with 20–29 years), of black ethnic group (OR 2.76, 95% CI 2.08 to 3.67 for blacks vs Indian/Sri Lankan/Bangladeshi or Pakistan, p<0.001), with smear-positive pulmonary TB (OR 1.45, 95% CI 1.08 to 1.96, p = 0.01) and with a good understanding of English (OR 2.03, 95% CI 1.37 to 3.02 for good English reading vs no English reading, p = 0.005; table 2).
Factors associated with being offered an HIV test among those who had not tested positive previously (all 1836 patients who did not know they were HIV-positive prior to the diagnosis of tuberculosis (TB))
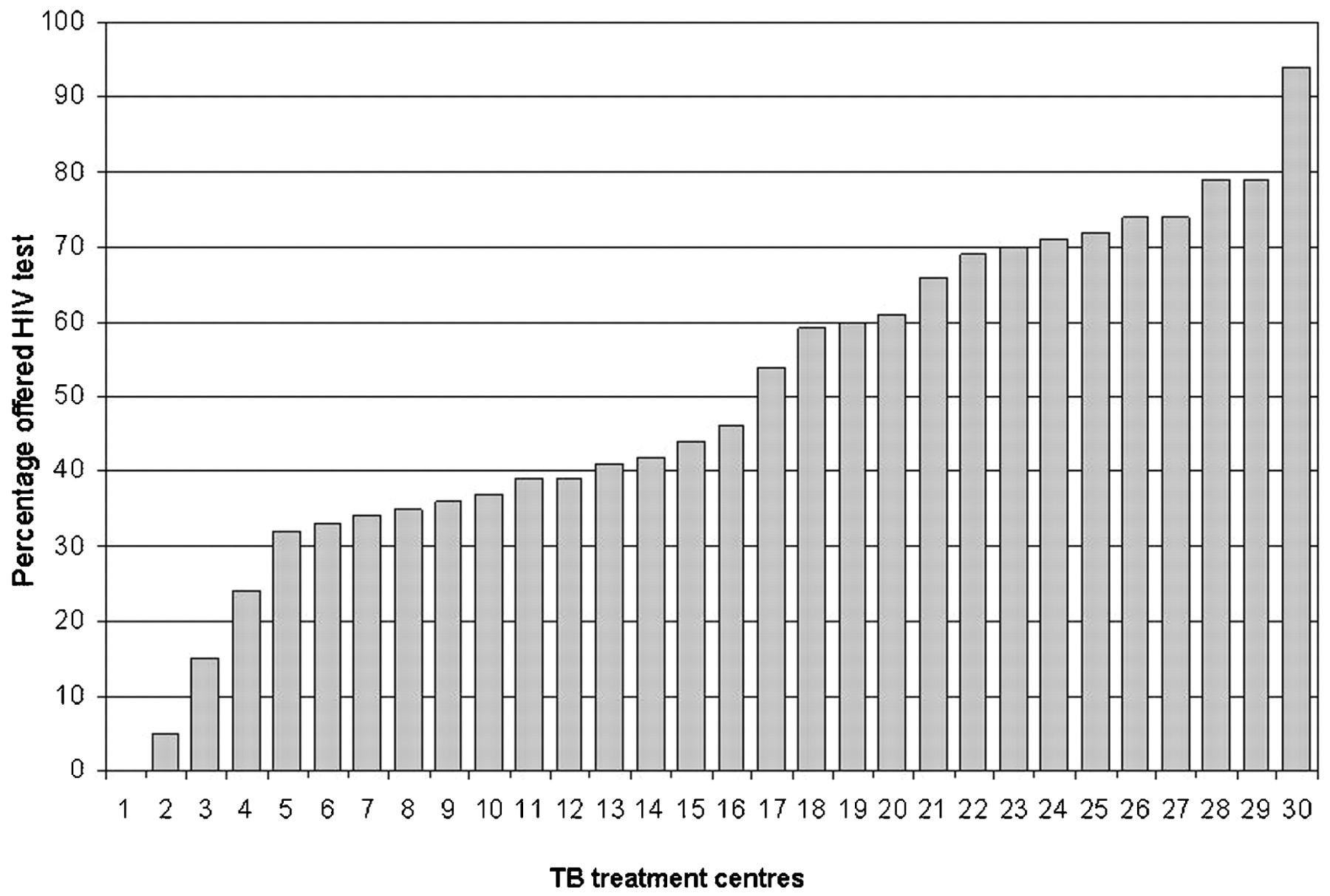
There was considerable variation between TB centres in terms of offering HIV testing, with only one centre offering HIV tests to over 80% of patients with TB. More than half of TB treatment centres offered HIV testing to less than half of their TB patients (fig 2).

{kind=link}
{kind=link}
Percentage of patients with tuberculosis (TB) offered HIV testing by a TB centre in London.
Among those who were aged ⩾20 years who were unaware of their HIV status at the time of TB diagnosis, 72.9% (603/827) of patients accepted HIV testing if offered. The prevalence of HIV among those previously unaware of their HIV status who accepted an HIV test was 14.3% (86/603). There was no difference between ethnic groups in acceptance of an HIV test if offered. The only factors associated with refusal of an offered test were being female (OR 2.1, 95% CI 1.4 to 3.0) or age >49 years (OR 2.3, 95% CI 1.2 to 4.5 for those aged 50–59 years compared with 20–29 years and OR 3.8, 95% CI 1.9 to 7.7 for those aged ⩾60 years compared with 20–29 years; table 3).
Factors associated with refusing an HIV test (among the 827 patients who were aged >20 years without a previous HIV diagnosis and offered an HIV test)
With regard to the timing of the HIV diagnosis in relation to the TB diagnosis, approximately half (99/193, 51.3%) of patients co-infected with HIV/TB had been tested previously for HIV and were aware of their HIV status at the time of the TB diagnosis; 42% (81/193) were tested and diagnosed with HIV at the time of their TB diagnosis; and the remaining 16.7% (13/193) patients had an unknown time of HIV diagnosis in relation to their TB diagnosis.
Discussion
The HIV epidemic is likely to have contributed heavily to the rise in TB cases observed in London over the past decade.5 This study reports that the prevalence of HIV co-infection in patients with TB in London in 2003/4 was high at 10% overall, although this is likely to be an underestimate as over half of the patients with TB in our study were not offered HIV testing. In those with an HIV test result, the prevalence of HIV was 25.6%. We found that HIV infection in those tested was generally concentrated in expected at-risk groups, with the highest prevalence of HIV found in those of black African ethnicity, reflecting the epidemiology of TB and HIV in those countries.
Studies linking TB and HIV surveillance databases estimated the proportion of adults with HIV and TB co-infection in the UK as 3.3% in 19985 and 5.7% between 1999 and 2003.6 Studies in other low prevalence countries have estimated HIV/TB co-infection of 4.4% in 1999–2001 in a study of surveillance data in the Netherlands,8 8% in surveillance data in the USA in 20049 and 3% in a Canadian study of all TB notifications in 1997/8.10 The use of routine surveillance to report rates of HIV co-infection in patients with TB is limited, however, by the inherent restrictions in all surveillance systems. In addition, it is also likely that low HIV testing rates in patients with TB resulted in an underestimate of the prevalence rates of HIV in these patients. HIV/TB co-infection rates of 11.4% were found in an unlinked anonymous survey of patients with TB in south London in 1999,11 which more closely reflect our findings.
HIV infection is the strongest known risk factor for reactivation of latent TB, and a number of guidelines in the UK and internationally recommend universal HIV testing for all patients with TB.12 13 14 Despite this, we found that only half of patients diagnosed with TB in our study were offered HIV testing, indicating a gap between national guidance in this area and practice. A small study in two centres in London in 2002 identified low rates of testing with only just over half (131/236, 56%) of patients with TB being offered HIV testing.15 This observation has also been noted in other studies from countries with a low prevalence of TB where suboptimal HIV testing rates in patients with TB were also reported. Over three-quarters of patients with TB in a Canadian study of all cases of TB in Canada from 1997 to 1998 were not tested for HIV.10
We found in our study that patients in recognised higher risk groups for HIV—such as individuals of black African origin, those born overseas and those aged 20–49 years—were significantly more likely to be offered testing but, even within the highest risk groups, testing was not universally offered and varied considerably by TB centre from 0% of patients with TB offered HIV testing in one centre to 94% offered testing in another. This implies that testing practices are highly dependent on the local culture of the clinics and the individual practices of healthcare workers.
Encouragingly, in those offered HIV testing the uptake was high. This implies that barriers to HIV testing may rest with healthcare staff, possibly because of a lack of confidence in offering an HIV test or because of preconceived ideas about the likelihood of patients to accept the test. Stigma related to HIV infection is thought likely to reduce the uptake of HIV testing in some communities, particularly those of African origin, and that this stigma is the greatest deterrent to HIV testing even when offered at the time of a TB diagnosis.16 17 However, we found no association between ethnicity and acceptance of HIV testing if offered, and those of black African ethnicity were no less likely to accept testing than those of white ethnicity with approximately three-quarters in both groups accepting testing if offered.
One barrier that we identified to being offered an HIV test was a patient’s level of spoken English. Patients with TB who had poor spoken English skills were significantly less likely to be offered an HIV test than those with good spoken English, yet this group is likely to be at high risk of HIV infection. Staff may have found the need to find interpreting services independent of the patient’s family and friends too much of a barrier to offering testing for HIV in a busy clinical setting. TB centres should ensure that staff have access to adequate interpreting facilities to enable HIV testing in all patients. Further work is required to address attitudes and practice of healthcare staff towards universal HIV testing and to determine barriers behind failure to comply with guidance. There is also a need to identify barriers to acceptance of testing, especially in women.
It is estimated that approximately 30% of HIV-infected individuals in the UK are unaware of their infection and so are unable to benefit from access to antiretroviral therapy or prevent further transmission of HIV by protecting others from infection.18 19 20 21 Late diagnosis is also associated with increased mortality, with 24% of deaths in HIV-positive adults attributable to late HIV diagnosis in a UK audit in 2005.22 It has been shown in a number of studies that people presenting with severe HIV-related disease frequently have a history of repeated previous contacts with medical services, both in primary and secondary care, but were not tested for HIV.22 23 24 25 Clinical judgement alone cannot be relied upon to ensure that individuals at risk of HIV infection are correctly identified.26 As TB occurs at relatively preserved levels of immune function, it may be the presenting feature of patients with HIV and TB in this study not offered HIV testing represents a missed opportunity. In addition, a recent review of patients with TB in one London centre noted that HIV co-infection in patients with TB appeared to affect the incidence of hepatotoxicity, suggesting that routine testing for HIV is also required to identify patients at risk of hepatic complications of TB treatment.27
In line with international initiatives, the UK Chief Medical Officer recently called upon doctors in the UK to increase uptake of HIV testing.12 28 One approach advocated is the use of universal opt-out testing where HIV testing is considered to be part of routine medical care and offered routinely to all or selected patient populations. The British HIV Association (BHIVA) guidelines for HIV testing published in 2008 recommend routine opt-out testing in certain patient groups who are identified by risk or clinical indicators including all patients with TB.13
Opt-out testing is currently used successfully in the UK in genitourinary medicine clinics where uptake rates of >85% have been reported.29 In the antenatal setting in the late 1990s, uptake of HIV testing was highly variable and dependent upon the practice of the individual healthcare worker.13 In 2000, Health Authorities were asked to put arrangements in place for universal opt-out testing in antenatal care as an integral part of care. This led to a dramatic increase in testing rates to 93.2% in 2007 with a corresponding reduction in babies born with HIV.30 Similar approaches through the commissioning process could be used to establish universal opt-out HIV testing in TB clinics.
This study has considerable strengths, being a large, highly complete and representative sample of patients with TB in London. The information was obtained directly from case managers so is likely to be of high quality and avoids the limitations of matching based estimates and enables collection of detailed risk factor information.
Our study also has some limitations. The data are 5 years old, but the recommendation to test patients with TB for HIV were already in place at the time of the study.14 31 It is unclear whether recent guidance from the Chief Medical Officer and the BHIVA to improve HIV testing has had an impact on improved testing rates for HIV in patients with TB. It is also possible that patients were asked to undergo HIV testing by different clinical staff who did not record this information in the clinical records. We were unable to determine possible reasons for staff not offering the test and for patients’ refusal if offered, and further qualitative work is required in this area.
In summary, our study shows that TB centres in London failed to offer HIV testing to half the patients diagnosed with TB, indicating multiple missed opportunities for testing those with potentially undiagnosed HIV. Those who were offered HIV testing had high uptake rates. To reduce avoidable HIV-related morbidity and mortality, universal opt-out HIV testing in patients with TB should be a key quality indicator for TB services and greater interaction between TB and HIV services encouraged. The manner of offering HIV testing to patients with TB—by whom and when in the diagnostic and treatment process to achieve best uptake of HIV testing—also needs to be explored.
Acknowledgments
The authors thank all the TB nurses, allied professionals and other staff in London who contributed data.
REFERENCES
Footnotes
Competing interests None.
Ethics approval The study was approved by the London Metropolitan Research Ethics Committee.
Provenance and Peer review Not commissioned; externally peer reviewed.