Article Text

Abstract
Background: Inhaled corticosteroids are widely used to treat asthma. There is a need to be able to compare different inhaled corticosteroids and different doses of an inhaled corticosteroid to determine potency and dose equivalence, but measuring efficacy in a dose related manner is difficult because of their slow onset of action. There is uncertainty about the role of sequential dosing regimens and the best end point for such studies. We have explored the use of sequential quadrupling dose regimens and a range of end points to assess the response to budesonide in subjects with asthma.
Methods: 21 subjects with mild asthma, aged 18–65, took part in a randomised three way crossover study comparing two sequential and one non-sequential regimen, separated by at least 3 weeks. The sequential regimens consisted of increasing doses of inhaled budesonide (100, 400 1600 μg/day) with each dose being given for 1 or 2 weeks; the non-sequential regimen consisted of 1600 μg/day for 2 weeks with end points measured after 1 and 2 weeks. The end points studied included the provocative dose of adenosine monophosphate causing a 20% fall in forced expiratory volume in 1 second (PD20AMP), lung function, symptoms, and bronchodilator use.
Results: There was a dose related increase in PD20AMP with both sequential dose regimens. The increase in PD20AMP ranged from 1.49 doubling doses (DD) following the lowest dose (100 μg/day) to 3.1 DD following the highest dose (1600 μg/day) in the 1 week sequential regimen and from 1.98 to 4.03 DD in the 2 week sequential regimen; standard deviations (SD) for the changes in PD20AMP ranged from 1.3 to 2.6 DD. Changes in forced expiratory volume in 1 second (FEV1) and morning peak expiratory flow rate (PEFR) were dose related but small and more variable (maximum change in FEV1 = 148 ml, SD 228 ml), while changes in evening PEFR, symptoms, and bronchodilator use were small and not dose related. Change in PD20AMP after budesonide 1600 μg did not differ significantly between regimens.
Conclusion: Combining PD20AMP measurements with a sequential regimen of three quadrupling doses of an inhaled corticosteroid given for 1 or 2 weeks provides clear dose-response curves for comparative studies. PD20AMP is a more sensitive end point for this purpose than FEV1, PEFR, symptoms, or relief inhaler use.
- asthma
- inhaled corticosteroid
- bronchial responsiveness
Statistics from Altmetric.com
Inhaled corticosteroids are a very effective treatment for asthma. There are marked differences in the pharmacokinetic profiles of the inhaled corticosteroids currently available,1,2 and these are likely to affect their systemic activity relative to their therapeutic airway effects. It is important to be able to compare the efficacy and adverse effects of different inhaled corticosteroids and different doses of an inhaled corticosteroid to determine their potency and dose equivalence.
Comparing the efficacy of two drugs should ideally involve a dose-response comparison but, because the response to an inhaled corticosteroid continues to improve for weeks or months after starting treatment,3–6 such studies are difficult. There is uncertainty about the optimal end point to use for such studies and whether sequential dosing regimens can overcome some of the problems. This study was therefore designed to explore the use of sequential dosing regimens in conjunction with various commonly used outcome measures.
We compared the magnitude and variability of change in bronchial responsiveness to adenosine monophosphate (AMP), forced expiratory volume in 1 second (FEV1), morning and evening peak expiratory flow rate (PEFR), symptoms, and bronchodilator use following two sequential quadrupling dose regimens with doses of budesonide increasing at 1 and 2 week intervals. Change in the provocative dose of AMP causing a 20% fall in FEV1 (PD20AMP) following the 1600 μg dose of budesonide was compared between the two sequential regimens and between these regimens and the first and second week, respectively, of the non-sequential regimen.
METHODS
Subjects
Subjects were included in the study if they were aged 18–65 years, had a diagnosis of asthma, symptoms consistent with asthma, and bronchial hyperresponsiveness to AMP (PD20AMP <29.5 μM at screening). Subjects were excluded if the FEV1 was less than 60% predicted or if they were a current smoker or had a smoking history of more than 10 pack years. Those taking asthma medication other than an inhaled short acting β agonist as required or sodium cromoglycate were excluded as were those who had taken an inhaled steroid in the previous 4 weeks or oral steroids in the previous 3 months or had had an exacerbation or chest infection within 6 weeks. Women of child bearing age had to be using adequate contraception.
The study was approved by the Nottingham City Hospital research ethics committee and subjects gave written informed consent.
Measurements
FEV1 was measured by dry bellows spirometer (Vitalograph, Buckingham, UK) as the larger of two values within 100 ml. The provocative dose of adenosine monophosphate causing a 20% fall in FEV1 (PD20AMP) was determined using a breath activated dosimeter (MEFAR, Brescia, Italy) set to nebulise for 1 second with a pause of 6 seconds at a pressure of 152 kPa. Adenosine monophosphate (Sigma, UK) was dissolved in 0.9% saline to give a doubling dose range from 0.115 to 472 μM. An initial inhalation of 0.9% saline was followed by doubling doses of AMP with FEV1 measured 2 minutes after each dose. The inhalation challenge was stopped once FEV1 had fallen by 20% from the post-saline value or the maximum dose of AMP had been inhaled. PD20 values were calculated by interpolation between the last two doses on the log dose-response scale; censored values above 472 μM were arbitrarily assigned double the maximum dose (944 μM) while a response to the initial saline inhalation was assigned the minimum dose (0.115 μM). Subjects kept diary cards, recording peak flow rate as the highest of three attempts (mini-Wright peak flow meter), symptoms, and use of relief inhaler twice daily. All subjects received training in spirometric testing and AMP challenge before entry into the study.
Study protocol
The study had a single blind crossover design in which patients took sequentially increasing doses of inhaled budesonide for 1 or 2 weeks or a course of high dose budesonide for 2 weeks. The doses given were as follows:
-
budesonide 100, 400 and 1600 μg/day for 1 week each;
-
budesonide 100, 400 and 1600 μg/day for 2 weeks each;
-
budesonide 1600 μg/day for 2 weeks.
The doses were divided and given twice daily apart from the 100 μg dose which had to be given once daily as there is no 50 μg Turbohaler; previous studies have shown no difference in efficacy between once and twice daily low dose budesonide.7,8 The three regimens were given in random order determined independently by computer generated code. There was a washout period of at least 3 weeks following each dosing regimen.
Subjects were taught to use the inhalers at the first visit. They were given four inhalers containing active drug or placebo at the start of each dose period, two labelled for morning use and two for evening use, and all were returned at the end of each dose period.
Subjects attended at the beginning of each treatment period and then weekly during the 1 week sequential regimen and the non-sequential regimen and 2 weekly during the 2 week sequential regimen; all visits were at the same time of day within 2 hours. At each visit diary cards were checked and use of medication confirmed followed by spirometric tests and an AMP challenge. Subjects were asked to withhold their inhaled β agonist for 6 hours before each visit and caffeine-containing food and drink from midnight. The main purpose of the study was to determine the magnitude and variability of change in PD20AMP, FEV1, peak flow rate, symptoms, and relief inhaler use in the two sequential regimens. We also set out to compare changes in PD20AMP after 1600 μg budesonide with all three regimens.
Analysis of data
PD20 values were log transformed before analysis and geometric mean values calculated; change in PD20AMP was measured in doubling doses. The percentage of days and nights without symptoms and use of relief inhaler and mean morning and evening PEFR were calculated for the 7 days before each visit. Maximum change in PD20AMP and FEV1 were analysed for period effects by two way analysis of variance (ANOVA). Mean dose-response slopes were calculated for the sequential regimens after fitting regression slopes for each end point against the log dose for each subject. Changes in PD20AMP after 1600 μg budesonide in the 1 and 2 week sequential dose regimens were compared with each other and with changes in PD20AMP after the first and second week, respectively, of the 1600 μg non-sequential regimen by paired t test.
RESULTS
Of 24 subjects randomised, two were excluded before study entry due to failure to attend and failure to bronchoconstrict with AMP; a third subject was withdrawn after one treatment period due to worsening asthma. Twenty one subjects were included in the analysis, one of whom completed two treatment periods but failed to develop a PD20AMP at the start of the third. All but five of 227 potential PD20AMP data points were available for analysis. Of the 17 PD20 measurements that were censored to 944 μM 16 were associated with the highest dose of budesonide and these were evenly distributed throughout the three treatment regimens.
The 21 subjects (13 men) had a mean age of 42 years; baseline demographic data are shown in table 1. There was no period effect for maximum change in PD20AMP or FEV1.
Baseline demographic details of patients included in the analysis
Dose-response changes with budesonide
PD20AMP
There was a dose related increase in PD20AMP with both sequential regimens. The change in PD20AMP ranged from 1.49 doubling doses (DD) following the lowest dose (100 μg/day) to 3.1 DD following the highest dose (1600 μg/day) for the 1 week regimen and from 1.98 DD to 4.03 DD for the 2 week regimen. The standard deviation of the measurements ranged from 1.3 DD to 2.6 DD AMP (fig 1, table 2). The dose-response relationship for budesonide was significant for both sequential regimens. The mean slope of change in PD20AMP was 1.43 (95% CI 0.64 to 2.22) DD per quadrupling dose of budesonide for the weekly regimen and 1.73 (95% CI 0.72 to 2.74) DD doses for the 2 weekly regimen.
Mean (SD) change in PD20AMP, FEV1, and morning and evening PEFR and median (interquartile range) days and nights free of symptoms and bronchodilator use for all three dosing regimens
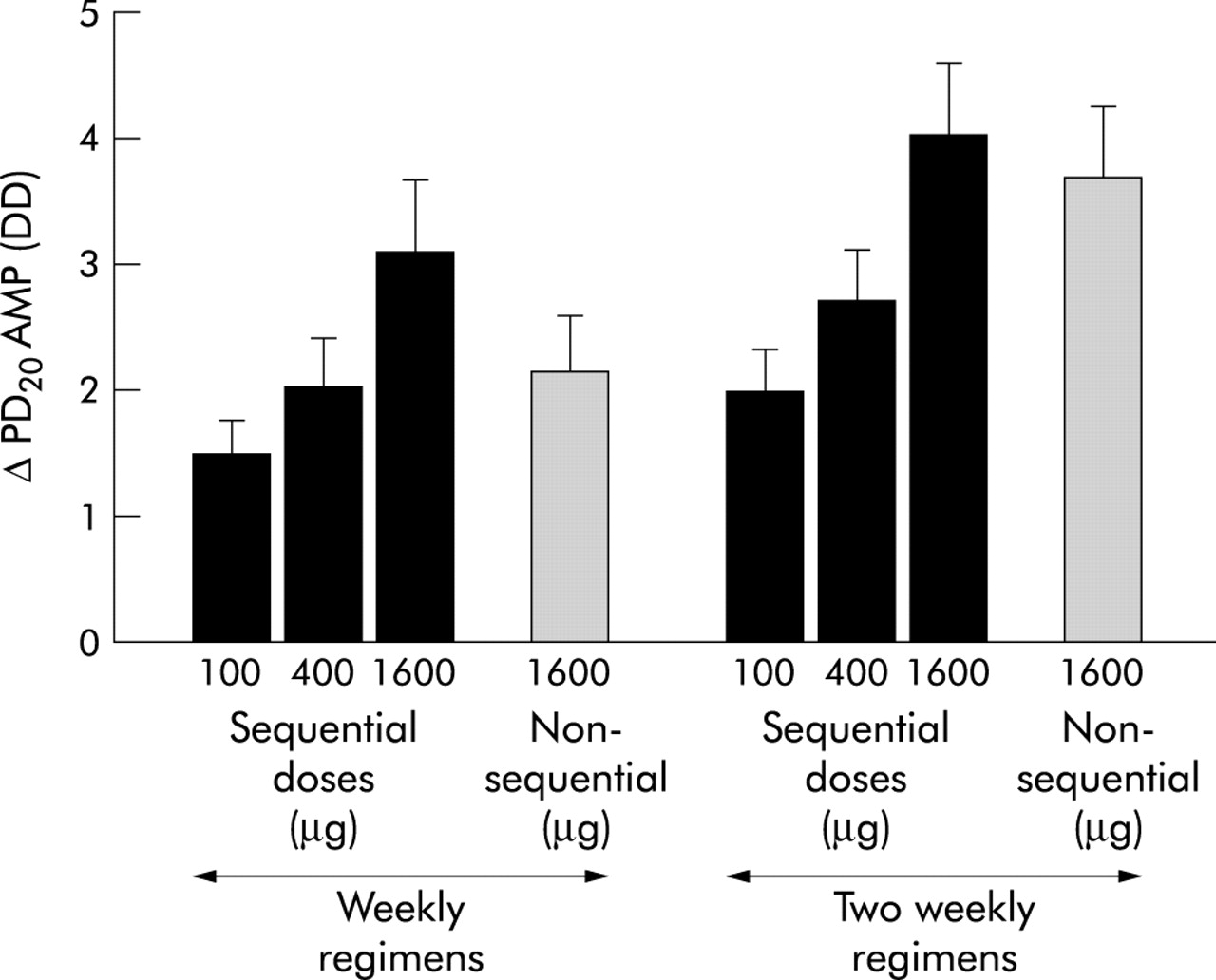
Mean (SE) change in PD20AMP (doubling doses, DD) after quadrupling doses of budesonide in the 1 and 2 week sequential regimens and after the first and second week of 1600 μg in the non-sequential regimen.
Lung function
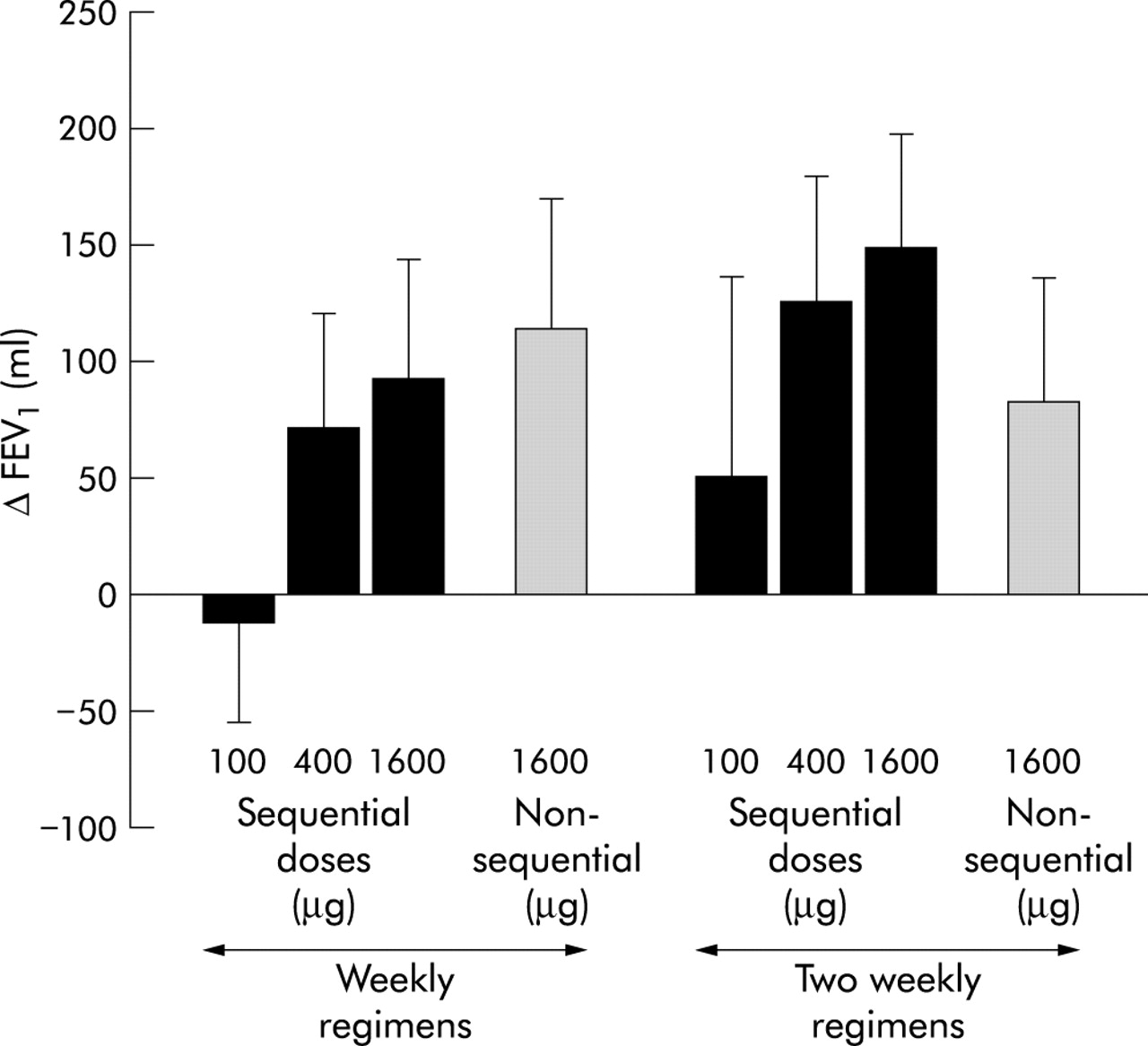
There was a small dose related increase in FEV1 which was significant for the 1 week but not for the 2 week sequential regimen. The size of the response ranged from −14 ml following the lowest dose to 90 ml following the highest dose in the 1 week sequential regimen and from 50 ml to 148 ml in the 2 week sequential regimen (fig 2, table 2). The variability of the response was large with standard deviations ranging from 192 to 367 ml.

Mean (SE) change in FEV1 after quadrupling doses of budesonide in the 1 and 2 week sequential regimens and after the first and second week of 1600 μg in the non-sequential regimen.
Morning PEFR also showed a small dose related increase which was significant for the 1 week but not the 2 week regimen (fig 3, table 2). Mean absolute values for the lowest to highest doses of budesonide ranged from 470 to 491 l/min for the 1 week regimen and from 469 to 484 l/min for the 2 week sequential regimen; the standard deviation of the measurements was around 90 l/min. Changes in evening PEFR were small and not dose related (fig 3).

{kind=link}
{kind=link}
{kind=link}
Mean (SE) morning (A) and evening (B) peak expiratory flow rates (PEFR) after quadrupling doses of budesonide in the 1 week and 2 week sequential regimens and after the first and second week of 1600 μg in the non-sequential regimen.
Symptoms and bronchodilator use
There were no dose related effects of treatment on daytime or night time symptoms or bronchodilator use with either sequential regimen (table 2).
Maximum change in PD20AMP with each regimen
The change in PD20AMP following 1600 μg budesonide was higher with the 2 week regimen than with the 1 week sequential regimen although the difference was not significant (fig 1). The change in PD20AMP with 1600 μg budesonide was also higher with the sequential than with the non-sequential regimen after both 1 week (0.75 DD) and 2 weeks (0.4 DD), but again neither difference was significant (table 3).
Mean (95% CI) difference in change in PD20AMP after 1600 μg budesonide between the two sequential regimens and between the sequential and non-sequential regimens
DISCUSSION
In this crossover study in patients with mild asthma there was a large dose related increase in PD20AMP following three sequential quadrupling doses of budesonide with both the 1 and 2 week regimens. Changes in FEV1 and morning PEFR were small and less clear cut than PD20AMP and were only dose related in the 1 week regimen; changes in evening PEFR, symptoms, and relief inhaler use were small and were not dose related.
Previous dose-response studies of inhaled corticosteroids have sometimes shown dose related changes but not always, due in part to differences in study design and end points measured.9–15 We therefore compared two sequential dosing regimens and a range of end points to assess the response to an inhaled corticosteroid. Sequential dosing regimens may offer advantages when comparing different inhaled corticosteroids and different doses of an inhaled corticosteroid. They are shorter than traditional crossover studies which require a washout period after each dose, and they require fewer subjects than parallel group studies.
By using quadrupling doses of an inhaled corticosteroid we found a large dose related increase in PD20AMP even in subjects with mild asthma. The variability in the response was small in relation to the size of change in PD20AMP and similar for the two sequential regimens, suggesting that moderate numbers of subjects would be required for comparative studies. The mean effect of treatment on bronchial responsiveness is probably an underestimate since treatment with budesonide caused a small number of PD20AMP values to be censored, although these were evenly distributed between treatment regimens. Bronchial responsiveness to AMP was a more sensitive end point than measures of lung function, symptoms, and relief inhaler use and would appear to have considerable advantages for comparative and dose-response studies of inhaled corticosteroids. The poor sensitivity of the other end points was partly caused by the fact that we studied subjects with mild asthma; however, these subjects have other advantages for studies of inhaled corticosteroids since they are less likely to require other medication or to have an exacerbation during the study. Bronchial responsiveness appears to correlate well with more clinical markers of efficacy as detailed in the companion paper also published in this issue of Thorax.16
Three previous studies have used sequential doubling dose regimens to compare systemic and airway effects of inhaled corticosteroids.13–15 The largest changes were seen in the study that measured PC20AMP following 1600 μg budesonide after doubling increments every 3 weeks,14 and the size of the effect was similar to that seen in our study. Use of quadrupling doses with shorter treatment periods, as in our study, should enable the duration of dose-response comparisons to be reduced.
The changes in PD20AMP seen with sequential dosing regimens will relate to duration of treatment as well as dose. This appeared to be the case since, although not significant individually, the changes in PD20AMP following 1600 μg budesonide were greater after 2 weeks than after 1 week, both within and between the sequential and non-sequential regimens.
We conclude that combining measurement of PD20AMP with a sequential quadrupling dose regimen in which doses are increased at 1 or 2 week intervals provides a simple and efficient method to assess the response to an inhaled corticosteroid. This should facilitate comparisons of different inhaled corticosteroids and different doses of an inhaled corticosteroid.
Acknowledgments
The authors thank AstraZeneca for providing financial support and indistinguishable active and placebo inhalers, Sarah Pacey for subject randomisation and dispensing the medication, Sarah Lewis for statistical advice, and Sarah Newton and Sue Cooper for help with the subjects.