Article Text

Abstract
The recent British Thoracic Society guidelines recommend that surgical mortality should not be greater than 8% for pneumonectomy and 4% for lobectomy. These cut offs are advanced as guidelines to inform decision making as to whether or not patients with operable lung cancer should be offered surgery. They have been developed from a notion of what acceptable surgical mortality should be. The planning of care for patients with lung cancer involves making choices between different treatments with different outcomes. While it is accepted that the probability of these outcomes is likely to differ among patients, individual patient preferences for them are also likely to vary. Fixed cut offs for surgical mortality mean ignoring this variation. Decision analysis can be used to assist in the complex task of integrating clinical characteristics and varying patient preferences. By considering high risk patients with potentially curable stage Ia non-small cell lung cancer, it is shown that decision analysis has the potential to illuminate decision making and guideline development within the field of cancer care.
- decision analysis
- lung cancer
Statistics from Altmetric.com
The recent British Thoracic society guidelines1 on the selection of patients with lung cancer for surgery provide recommendations for thresholds of operability. Although the guidelines contain recommendations for action, their use in practice remains challenging because of the complexity of the decision they are intended to inform. In decisions that entail choosing between multiple alternatives under conditions of uncertainty, decision analysis can be helpful. In this paper we use decision analysis to explore the operative decisions for patients with stage Ia non-small cell lung cancer (NSCLC) and borderline lung function.
WHAT THRESHOLD FOR LOBECTOMY OR PNEUMONECTOMY IN PATIENTS WITH STAGE IA NSCLC WITH BORDERLINE LUNG FUNCTION?
In patients with stage Ia disease and borderline lung function the guidelines1 suggest that patients should be discussed in the multidisciplinary meetings, but that cut offs for surgery should be relatively fixed at 4% for lobectomy and 8% for pneumonectomy. This recommendation implies that the treatment of any patient with a given set of clinical characteristics should be largely decided in the light of a prior decision about what the surgical mortality rate over a series of patients should be. However, if the decision making process is approached in a decision analytical way, taking simultaneous account of the other alternative treatments and the individual patient's preferences, it becomes clear that the maximum chance of surgical mortality an individual patient should face may well differ significantly from these figures.
In order to understand why this is the case it is helpful to consider, in the light of the medical decision making literature as a whole, how it might be possible to arrive at an answer to the question “what should the surgical mortality rate be?”
Answer 1
It should be the ex post (after the event) rate found in best practice surgery as determined in randomised controlled trials or, in their absence, well conducted clinical studies. The question arises: how did those trials and studies deal with patient preferences in general and variations between patients in their preferences in particular? If the studies dealt with patient preferences by ignoring them, or by making assumptions about those of the “average” patient, this answer is clearly not an answer compatible with explicit respect for patient preferences, either average or individual.
Answers 2 and 3
It should be the (ex post) surgical mortality rate that results from the implementation, by “competent” surgeons, of the decisions for each individual patient (between surgical and other treatment options) made on the basis of:
-
the average patient's preferences (elicited in some explicit way) in conjunction with the clinical characteristics of the individual patient;
-
the individual patient's preferences (elicited in some explicit way) in conjunction with the clinical characteristics of that individual patient.
In any specific context these three answers may clearly differ numerically, the first from the latter pair because there may be only a loose connection between clinicians' assumptions about patient's preferences and their actual preferences,2 and the second from the third because individual patient preferences may not be distributed symmetrically around the “average”.
Following such conceptual clarification it will be fairly obvious that, in the local application of guidelines for an individual patient, only the third answer has ethical validity. Moreover, it becomes apparent that guidelines that seek to determine a cut off surgical mortality rate beyond which patients are discouraged from choosing surgery risks denying patients the opportunity to reflect their preferences. The uniform guideline approach has pragmatic appeal in that it greatly simplifies the decision making process, but it should not be forgotten that the ex post mortality rate for a group of patients has, per se, no ethical relevance in the clinical situation. Here the only issue is whether the patient concerned has consented to surgery on the basis of the best available assessment of their personal chance of dying on the table in the forthcoming operation. In this assessment, any ex post outcome frequency rate—either for the surgeon, the operation, or both—can provide only one input (albeit a typically useful one) into the derivation of this necessarily subjective and ex ante (before the event) probability.
WHAT CHANCE OF SURGICAL MORTALITY SHOULD THE PATIENT BE WILLING TO ACCEPT?
Having been provided with this best available assessment of the probability of their personal chance of surgical mortality on this occasion, the issue for the patient is to compare this chance with the highest that they would be willing to accept. If it is lower than this “threshold” chance, they should accept surgery. If it is higher, they should refuse surgery.
But what chance of surgical mortality should the patient be willing to accept? This is not a simple straightforward matter of arriving at a figure directly and without consideration of other aspects of the choice situation. In fact, in order to establish it properly we have to establish the chances of, and the patient's personal values (utilities) for, all outcomes of all treatment options—that is, not only the chances and utilities for all the possible outcomes of the surgical option, but those for all non-surgical options as well. Only when we have modelled the management decision in this full complexity can the patient discover what chance of surgical failure is “too high”. The threshold surgical mortality probability for a patient cannot be established by considering only the surgical option.
We can make this point in the simplest possible way by using a binary example.
If there are only surgical and medical options and both have the same outcomes when successful (the patient survives 100 units of time) and when unsuccessful (the patient dies within 30 days), then, if the chance of failure in the medical option is x%, that is the threshold chance for surgery. If the 30 day medical mortality chance is 40%, any surgical mortality chance less than 40% makes surgery optimal in this case. Introducing various complications—including those arising from risk preferences and time preferences—as well as quality of life considerations does not change this essential point: the threshold chance for surgery is a function of the chances and outcomes in all relevant non-surgical options. Introducing these complications may, however, lead the point to be lost or overlooked. While it may seem utterly banal, it is all too easy for specialists in one management option to attempt to devise specialty-specific thresholds for patients when what is required are the patient-specific thresholds that can only be derived from analysis of all management options.
What are the aspects of the decision that patients attend to in formulating their preference (utility function)? The answer is that we do not know until it is explored systematically with the patient. A patient's preferences will reflect his or her attitude to uncertainty (conventionally called risk preference), to health effects occurring at differing periods of time in the future (conventionally called time preference), to different dimensions of health related quality of life (such as functional capacities, pain and discomfort, and anxiety and depression), and to the trade off between such health related quality of life considerations and life expectancy. This composite outcome of the duration and quality of survival is described by the Quality Adjusted Life Year (QALY). Much empirical work assumes that patients will make decisions driven by an attempt to maximise the number of QALYs that their choice produces. In other words that, in evaluating alternative courses of action, future life years are adjusted (downwards) to the extent that the health related quality of life experienced during any year falls short of full health. Such expected QALYs may, in addition, be time discounted and/or risk adjusted, although it is unusual to undertake both because empirically the two are necessarily confounded.
The ideal approach to a complex decision such as this, given that one wishes to be able to pay serious attention to patient preferences over outcomes as well as to questions of technical effectiveness, is to construct a decision analytical model. The best available patient-specific evidence and the patient's preferences should be put into this model and the alternative management options evaluated according to various outcome measures and integrating principles.
In the current absence of such an analysis we present a simple speculative model to confirm the importance of proceeding to this more sophisticated analysis and the advantages of doing so.
EXPLORATORY MODEL
The exploratory model is constructed using published data to derive the outcome probabilities for patients with stage Ia NSCLC. The outcomes associated with the radiotherapy arm use data from a series of 167 patients with T1N0 disease treated with a minimum tumour dose of 50 Gy given in 20 fractions over 4 weeks where 5 year survival was 32%.3 In units with facilities for continuous hyperfractionated accelerated radiotherapy (CHART) this survival would be likely to be better. Patients with stage Ia disease who survive surgery with only mild increase in breathlessness can be expected to have a 5 year survival rate of 61%.4 In operating on patients with poorer lung function some might survive surgery to be left very breathless. Survival data in such cases do not exist, so a best guess is used for the survival probability of patients left very short of breath after “successful” surgery. We have guessed that such patients might have half the survival of patients with only mild postoperative shortness of breath (0.3) The advantage of decision analysis is that, once an outcome estimate has been made, the impact of variations around that estimate can be explored using sensitivity analysis. It is important to emphasise that the tree is tailored to each individual patient. If, for example, a patient was particularly unfit and expected to do particularly badly with surgery, they might also have a particularly bad prognosis with radiotherapy. Here clinical judgement is being employed to refine trial data and the resulting probabilities can be used in the tree.
The other uncertainty is the preferences of patients for the various outcomes of the different possible management options. Decision analysis requires these preferences to be made explicit. In acknowledging the many difficulties in doing this, it should not be forgotten that conventional decision making claims to incorporate these preferences in some way or another and therefore is open to the same questions.
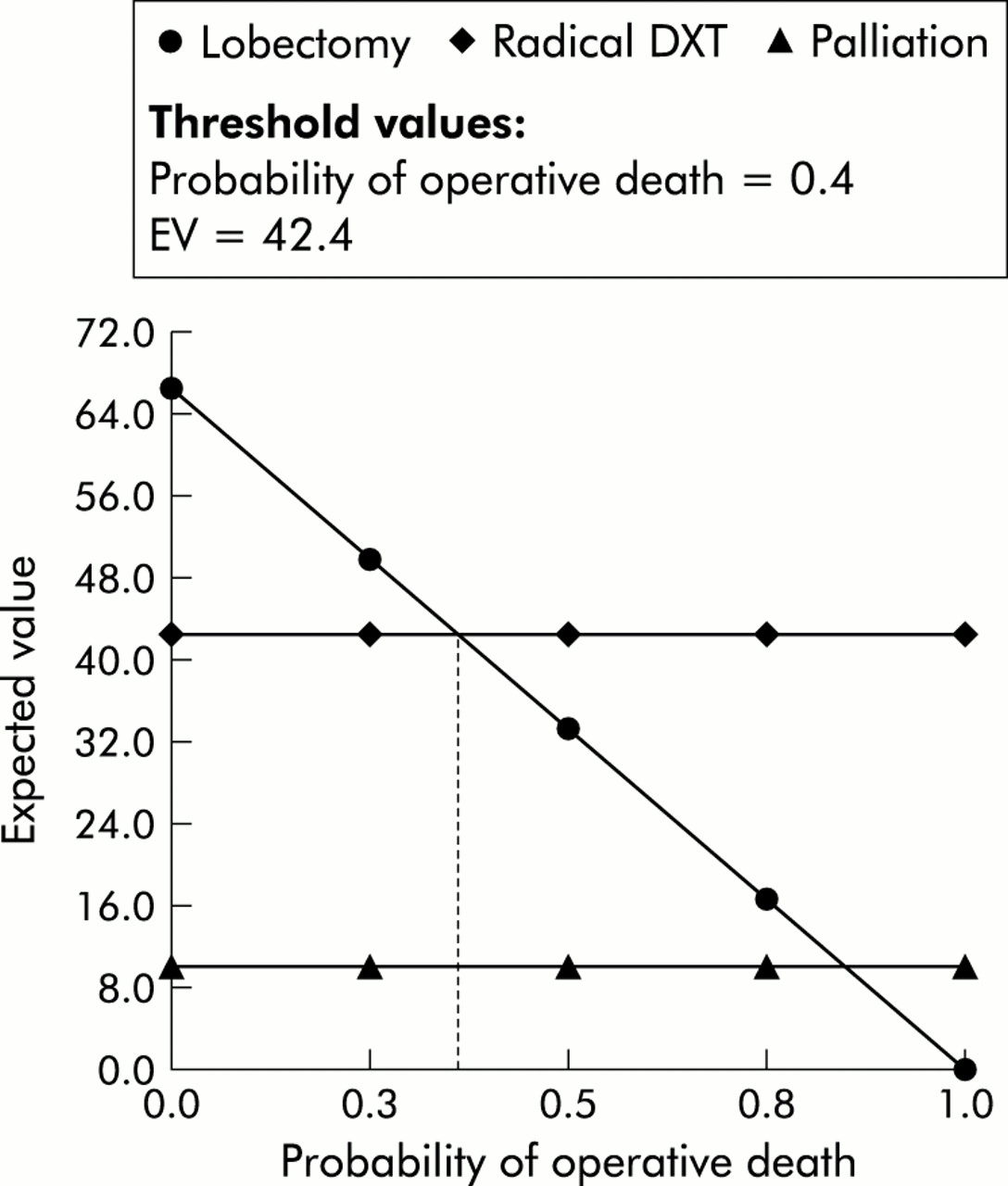
Our example shows that, when decision analysis is used to take simultaneously into account the risk of operative death along with the potential for cure both by surgery and radiotherapy, patients may well have a threshold probability of surgical mortality that is much higher than single figures. This raises the possibility that guidelines designed in such a way as to produce surgical mortality below 4% for lobectomy or 8% for pneumonectomy would be denying surgery to some patients for whom it is the optimal treatment. Figure 1 shows the “rolled back” evaluation of the baseline case.

Decision tree that lays out the treatment options open to individuals confronted with stage Ia lung cancer, the outcomes that might occur, and the patient's values attached to each. The square at the extreme left represents the decision node and a decision maker will choose one of the three branches: lobectomy, radiotherapy (DXT), or palliation. Once a choice has been made the outcomes of the choice will not be known with certainty but can be estimated using probabilities composed from clinical judgement informed by the evidence in the literature. Since the specific outcomes arising from a choice are uncertain, the branch points following a decision node are known as chance nodes (represented as circles). The label on a branch indicates an outcome and the number the probability of its occurrence. In this example patients opting for lobectomy might be faced with a risk of surgical mortality of 10% and thus the chance of survival will be 90%. Each branch ends with an outcome that has been valued by the patient on a scale from 100 (indicating the patient's best possible outcome) to 0 (the worst possible outcome). The expected value of any decision is calculated by multiplying the values of the various possible outcomes by the chance of their occurrence. Thus, the expected value (utility) of lobectomy where the risk of mortality is 10% can be calculated by adding all the branches—(0.1 × 0) + (0.081 × 70) + (0.189 × 30) + (0.384 × 100) + (0.246 × 40) = 59.6. A patient might be expected to choose the option having the highest expected value, known in decision analytical terminology as the highest expected utility, when the values incorporate risk attitude.
The baseline probabilities for the events in fig 1 are taken as closely as possible from the guidelines:
-
Operative death = 0.1 (this is varied in the sensitivity analysis shown below)
-
Very short of breath (SOB) post-lobectomy = 0.3
-
Survive 5 years given mild SOB post-lobectomy = 0.61
-
Survive 5 years given very SOB post-lobectomy = 0.3
-
“Cured” given 50 Gy given in 50 fractions over 4 weeks = 0.32
-
Survive 5 years given palliative care = 0.01
The baseline utilities attached to the outcomes in fig 1 are no more than a subjective attempt to integrate the life expectancy and quality of life differences for the various outcomes including any reductions in the latter associated with treatment processes. (We see them as risk adjusted but not time discounted.) The utility scale is an interval one so does not possess ratio properties: only intervals can be compared. Conventionally, 100 is assigned to the best outcome that is possible and 0 to the worst. We have assigned 0 to surgical mortality and 100 to survival for 5 years with some shortness of breath following surgery.
-
Survive 5 years with mild SOB after surgery (uSurvOpMildSOB5YS) = 100
-
Survive 5 years with mild SOB after radical DXT (uNoOpDXTMildSOB5YS) = 90
-
Survive 5 years very SOB after surgery (uSurvOpVerySOB5YS) = 70
-
Survive 5 Years very SOB with palliative care only (uNoOpPallVerySOB5YS) = 60
-
Survive <5 years with mild SOB after surgery (uSurvOpMildSOBNot5YS) = 40
-
Survive <5 years very SOB after surgery (uSurvOpVerySOBNot5YS) = 30
-
Survive <5 Years very SOB after radical DXT (uNoOpDXTVerySOBNot5YS) = 20
-
Survive <5 Years very SOB with palliative care only (NoOpPallVerySOBNot5YS) = 10
-
Operative Death (uOpDeath) = 0
Lobectomy emerges as the clearly optimal strategy in the baseline analysis, but our interest here is in the chance of surgical mortality that would change this decision. Figure 2 shows that a one way sensitivity analysis on surgical mortality indicates a threshold of 40%—that is, as we increase the chance of surgical mortality step by step (other things remaining the same), surgery remains the optimal choice until it reaches that figure.

{kind=link}
{kind=link}
The y axis displays the expected value (EV, utility) that results from patients choosing lobectomy, radiotherapy (DXT), or palliation. This results from multiplying the patients' value for a given outcome by the probability of its occurrence. For DXT and palliation the expected values are fixed and reflect the information in the tree in fig 1. For lobectomy the diagram displays a sensitivity analysis that shows how the expected value of lobectomy changes as the risk of operative death varies along the x axis from a probability of operative death of 0 to a chance of operative death of 1 (certain death). Normatively decision theory would suggest that the alternative with the highest expected value be chosen and lobectomy has the highest expected value until operative mortality reaches 36%. It should be noted that this result is a theoretical example consequent upon imputed patient valuations of outcome. It is not intended to suggest that the surgical mortality threshold should be 36% because this will depend upon real patient values and any “surgical threshold” should be patient specific.
Different utilities and probabilities from those in our baseline case will, of course, produce different surgical thresholds and that is our fundamental point, not that the surgical threshold will usually or often be of this order. Indeed, if surgeons were to act in such a way as to produce (ex post) the suggested rates of 4% and 8%, this may equally mean operating on some patients for whom surgery is not the optimal treatment. The essential point is that no generalisation can be usefully made without explicit consideration of all the individual patient preferences involved, and any ex post mortality rate needs to be interpreted and used in a very careful manner.
DISCUSSION
The use of decision analysis to explore operability thresholds for patients with stage Ia NSCLC with borderline lung function illustrates the way in which decision analysis allows patients' preferences to interact with the information in guidelines to obtain the care that best reflects their clinical characteristics and preferences. Although the spirit of the guidelines implies that flexibility will be provided by the discussion of individual cases in multidisciplinary meetings, these discussions are open to the effects of framing. The earliest of many demonstrations of framing effects focused on a hypothetical scenario of lung cancer decision making involving a choice between radiotherapy and surgery.5 Physicians' choices were influenced by whether the outcomes were presented in terms of the probability of survival or of death. Structuring treatment options using decision analysis avoids the framing effect because both probabilities are always in view. It is easy to see how individual centres might modify the decision tree if, for example, they were able to offer CHART.
While our fundamental point is a conceptual one, there are clearly practical implications. The actual mechanics of involving patients in a decision analytical approach to management remains poorly developed in lung cancer, but there are other areas where this has been successfully achieved.6,7 The complex task of structuring the decision requires the explicit formulation of the medical options and the probabilities consequent upon those options. Although this task is time consuming and involves the esoteric knowledge of the clinician, it can be done at leisure away from the consulting room. (A more complex tree exploring the possibility of surgical upstaging is available on request.) This leaves time in the consultation to concentrate on eliciting the patient's “expertise” which lies in evaluation of the possible outcomes.8 Inputting the patient's values for the outcomes into the decision tree once elicited is straightforward. The decision tree will then carry out the complex task of calculating which treatment choice maximises the patient's chance of seeing his or her goals realised.
Although the theoretical model described here suggests that a particular patient might opt for “high risk” surgery, it should be remembered that increased postoperative mortality would have wider implications for unit management with increased postoperative deaths taking their toll in terms of bed occupancy and staff morale. It would be naïve to suggest that a decision analytical approach that aims to capture patient values could ever be the sole dictator of practice. Treatment strategies can never be adopted in isolation from the constraints of the system delivering the service, notwithstanding whether those constraints involve coping with waiting lists or maintaining morale. But clinical decision analysis can facilitate the articulation of patient preference and that preference then becomes one of the many competing drivers of what “should” be done.
The Bristol paediatric heart surgery case raises many of the same issues we have discussed here. Once the role of patient preferences is clarified, we can see how important it becomes to ensure that the issue of “what should the surgical mortality rate be?” is carefully distinguished, both from the issue of “was the surgeon technically competent in this case/these cases?” and from the issue of “was appropriate informed consent obtained in each individual case?” Indeed, it becomes clear that the first question is really a problematical one to ask—and proffer an answer to in guidelines.
An ex post failure rate of 29% from a particular type of surgery carried out by a specific surgeon may indeed result from his or her (relative) technical incompetence. It may also result from technically competent surgery following failure to obtain parental consent on the basis of the best available evidence concerning the chance of surgical mortality in each individual case (in the context of a full exploration of the alternative courses of action). But it may also result from the fully informed and consented decision of parents who have accepted that the best available assessment of the chance of surgical mortality is less than their threshold probabilities (as determined by all the probabilities and preferences relevant to all their treatment choices) and performance of the ensuing surgery by technically highly accomplished practitioners. A decision tree which has been prepared in advance to reflect both the complexity and the uncertainty of the decision and then used to capture, articulate, and incorporate the patient's evaluation of outcomes can serve as a permanent record of an explicit process of informed consent.
Acknowledgments
Dr M Wildman is supported by an MRC Training Fellowship in Health Services Research.
Footnotes
-
Conflicts of interest: None.
-
The decision tree produced using the specialist decision analytic software DATA 3.5 by TreeAge will be automatically sent on receipt of an email message to jack.dowie{at}lshtm.ac.uk with the subject SEND THORAX. A demonstration version of DATA 3.5 may be downloaded from the TreeAge website at http://www.treeage.com. The additional tree mentioned in the discussion will also be sent. This will allow readers to input their own centre specific data (e.g. patient utilities or radiotherapy survival data) and test for surgical cut off.