Article Text

Abstract
Background In July 2008 a case of smear-positive pulmonary tuberculosis (TB) in a white UK-born nursery teacher was notified in London. The case had been symptomatic for 9 months while working in the nursery. The outbreak is described and the protective effect of BCG vaccination against latent Mycobacterium tuberculosis infection as measured by an interferon gamma release assay (IGRA) is assessed.
Methods Screening by chest X-ray and IGRA of nursery children, staff and their contacts was conducted using a ‘stone-in-the pond’ approach. Information was collected on various factors including BCG vaccination status, and data were analysed using multivariable logistic regression.
Results Overall, 168 children, 31 staff members and 57 other adults associated with the nursery were screened for TB. There were 12 cases of active TB and 43 cases of latent TB (72% children). 37.5% (95% CI 18% to 56%) and 40% (95% CI 30% to 50%) had a positive IGRA among teachers and children, respectively. 42% of children and 60% of adults were BCG vaccinated. In the adjusted analysis, BCG vaccination showed a significant protective effect against M tuberculosis infection in children (OR 0.25, 95% CI 0.09 to 0.69) and being taught by the index case was associated with acquiring TB infection (OR 18.91, 95% CI 4.43 to 80.79). A vaccine effectiveness of 66% was calculated, implying that 21 of the 32 infections could have been avoided if all children had been vaccinated with BCG.
Conclusions This outbreak shows extensive transmission of TB among very young children. BCG seems to have a protective effect against TB infection as assessed by positive IGRA in this cohort.
- Tuberculosis
- BCG
- outbreak
- IGRA
- nursery
Statistics from Altmetric.com
Background
The incidence of tuberculosis (TB) in the UK, and in particular in London, has increased over the last two decades.1 This has been accompanied by a change in the epidemiology of TB, with the disease now largely concentrated in certain population groups. The incidence of TB among children aged <5 years in the UK remains low.2 In 2005, despite the overall increase in TB cases, the Department of Health changed the UK policy on Bacillus Calmette-Guerin (BCG) vaccination from the general vaccination of all schoolchildren to a selective policy targeting infants with a high risk of acquiring TB and certain other risk groups.3 This decision was made in part because the UK met the criteria set by the International Union against Tuberculosis and Lung Disease4 for a selective BCG vaccination policy.
Several risk factors have been associated with an increased risk of acquiring tuberculous infection. Among these are immunosuppression, old age, smoking and contact with someone who has infectious TB including through travelling to or living in areas that are highly endemic for TB (>40 cases/100 000 population/year).5 The latter is reflected in the current UK policy on BCG vaccination6 which recommends immunisation of all infants (aged 0–12 months) living in areas of the UK where the annual incidence of TB is >40/100 000, all infants (with catch-up to 16 years of age) with a parent or grandparent born in a high-incidence country (annual incidence of TB >40/100 000), new entrants <16 years born in or who have lived for at least 3 months in a high-incidence country, individuals at occupational risk and travellers aged <35 years going to high-incidence areas for >3 months.6
Meta-analyses indicate that BCG vaccination is effective in reducing the risk of severe manifestations of TB and that it reduces the risk of acquiring TB in newborns by, on average, 50%.7 8 It has been difficult, however, to determine the effect of BCG vaccination on the risk of infection with Mycobacterium tuberculosis because the methods traditionally used for testing (eg, tuberculin skin test) do not distinguish between the effect of BCG vaccination and that of M tuberculosis infection.9 The interferon γ release assay (IGRA) is a blood test which measures interferon γ release of T lymphocytes stimulated by M tuberculosis antigens not present in M bovis BCG. It can therefore detect an immune response to M tuberculosis infection without also including the positive results induced by a prior BCG vaccination. IGRA performed in contacts of patients with infectious pulmonary TB for identification of individuals who have latent M tuberculosis infection is not confounded by prior BCG vaccination as is the tuberculin skin test,10 making it possible to study the protective effect of BCG against latent tuberculous infection as suggested by recent studies.9 11 12
In July 2008 the North West London Health Protection Unit (HPU) was contacted about a case of smear-positive pulmonary TB in a UK-born teacher who worked in a nursery in London. The case had been undiagnosed and symptomatic while working in the nursery for 9 months. Public health investigations led to the identification and management of an outbreak in the nursery. This paper describes the outbreak and assesses whether BCG vaccination has a protective effect against M tuberculosis infection.
Methods
The outbreak
The index case was a UK-born adult of British white ethnicity. The case was investigated by her GP because of a prolonged history of cough, tiredness and weight loss. The case had no history of travel to high-incidence areas during the last 2 years and had been vaccinated with BCG as a teenager. The case had been suffering from chronic cough and weight loss for 9 months and was initially diagnosed with ‘bronchitis’ before being diagnosed with TB (three sputum samples, all with mucopurulent appearance, acid-fast bacilli seen in all three samples, cultured as fully sensitive M tuberculosis, IGRA positive and x-ray changes compatible with pulmonary TB). The case was then immediately started on a 6-month course of antituberculous treatment. Household and close contact tracing was performed and a risk assessment was conducted at her workplace.
The index case was a nursery teacher. Active case finding was conducted where all children and staff who had been exposed in the nursery while the index case was symptomatic were contacted for screening of TB. The screening was conducted according to the ‘stone-in-the-pond’ principle13 whereby all close contacts of each new active case of TB were screened.
The setting
The workplace of the index case was a private nursery located in one of the most affluent parts of London. More than 90% of the children lived in either Kensington and Chelsea or Westminster boroughs of London, areas with a relatively low incidence of TB (in 2007, 29.1 and 29.9/100 000, respectively) but originated from diverse countries, mostly with a low incidence of TB.
The children who regularly attended the nursery were 2–5 years old, but there was also a weekly 1 h carer and toddler group where each toddler came with an adult carer. The nursery also ran a ‘summer camp’, a day nursery for children who were in London over the summer. The term for all the children had ended just before the index case was diagnosed with TB and the screening of contacts started 6 weeks after the last possible contact with the index case.
All individuals seen at a public hospital in this outbreak were seen at either St Mary's or Chelsea and Westminster hospitals in London. All IGRA tests were performed at St Mary's hospital using the QuantiFERON-TB Gold In-Tube assay (Cellestis, Darmstadt, Germany). QuantiFERON uses the region of difference−1 antigen's early secretory antigen targets 6 (ESAT-6) and TB 7.7, and culture filtrate protein 10 (CFP 10) to stimulate T effector cells specific for M tuberculosis to produce interferon γ. Those with a positive IGRA test from any screening round were recalled for a chest x-ray examination and clinical review. All previously unvaccinated children with a negative IGRA test were offered BCG vaccination.
Data collection
All children were assessed by the local paediatric and TB teams using a questionnaire and IGRA tests. For logistic purposes, all contacts were also screened by chest x-ray and baseline liver function tests were performed at the same time. At the time of screening, information on age, sex, BCG vaccination status, country of origin and contact with the nursery and the index case was collected. BCG vaccination status was assessed by vaccination card and/or BCG scar.
Definitions
Close contact: a person with a cumulative total exposure to a smear-positive case of TB exceeding 8 h within a restricted area equivalent to domestic rooms/class rooms.5
Latent M tuberculosis infection: in this outbreak, refers to an asymptomatic person with a positive IGRA test and a normal chest x-ray.
Active TB disease: x-ray changes compatible with TB in a person with a positive IGRA test and symptoms of TB where a decision to treat with a full course of antituberculous drugs has been taken, with or without the isolation of M tuberculosis.
Data analysis
Data were entered in Microsoft Excel and later imported to Stata 10.1 for analysis. We calculated attack rates and performed logistic regression for associations between latent TB infection and BCG vaccination, age, sex and having been taught by the index case. Adjusted ORs were used to get an approximation of the RR using the following formula: RR=OR/((1−Po)+(Po×OR)) where Po=incidence of outcome of interest (ie, infection rate in the group not BCG vaccinated) as described by Zhang and Yu.14 This formula is used to correct the adjusted OR obtained from logistic regression and to derive an estimate of an association or treatment effect that better represents the true RR. This RR approximation was used to calculate RR reductions/vaccine effectiveness (VE) using the formula VE=1–RR.
Results
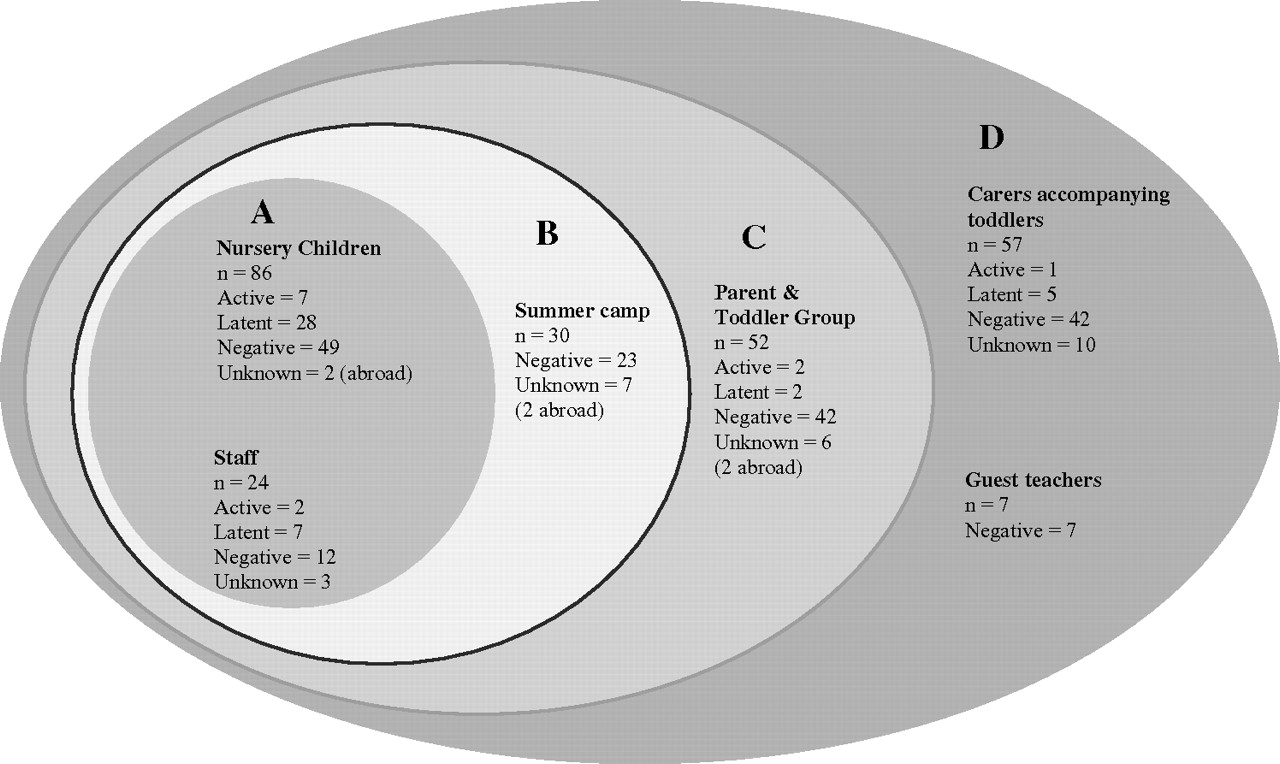
Using the ‘stone-in-the-pond’ approach,13 168 children, 31 staff members and 57 other adults associated with the nursery were screened for TB (figure 1). Among those in whom the BCG vaccination status was known (figure 2), 42% (53/126) of the children and 60% (32/53) of the adults were BCG vaccinated (table 1).

Screening results for cases stratified by closest exposure to the index case.

{kind=link}
{kind=link}
Overview of the individuals screened in the outbreak broken down by BCG vaccination status and development of latent or active tuberculosis infection. ATB, active TB infection; BCG+, BCG vaccinated; BCG−, not BCG vaccinated; BCG NK, BCG vaccination status unknown; IGRA, interferon γ release assay; LTBI, latent TB infection; Neg, negative IGRA; no test, individual not screened for TB; TB, tuberculosis.
Number of nursery contacts screened and outcome of the screening
Nursery contacts
Among the 256 nursery contacts screened, we found 12 active TB cases and 42 individuals with latent infection; 72% of these were children (table 1). The attack rate for infection, measured as IGRA positivity, was 9/24=37.5% (95% CI 18% to 56%) and 35/86 = 40.7% (95% CI 30.3 to 51.1) among teachers and children, respectively. For active disease, the rates were 2/24=8.3% (95% CI 2% to 14%) and 7/86=8.1% (95% CI −3% to 19%) for adults and children, respectively. Of 79 individuals with known place of birth, only 7 were from a country with a high incidence of TB. The median age of children was 2.6 years (IQR=1.5). Among the children, a significantly lower proportion of IGRA positivity was seen in BCG vaccinated individuals than in non-vaccinated individuals (13% vs 36%, p=0.008, 126 observations; table 2).
Association between infection with Mycobacterium tuberculosis and risk factors for the 168 children in the outbreak population
Univariable analysis
Among the 168 children, no significant association was found between tuberculous infection and age or sex (table 2). Information on country of birth was available for 66 children, 2 of whom came from a high-incidence country. Being taught by the index case was associated with a positive IGRA test (OR 11.61, 95% CI 3.87 to 34.83) and BCG vaccination showed a protective effect against infection (OR 0.28, 95% CI 0.11 to 0.70, table 2).
Among the 88 adults, no significant association was found between tuberculous infection and BCG vaccination (OR 0.11, 95% CI 0.01 to 1.03).
Multivariable analysis
Multivariable analysis was performed for the 168 children. In the fully adjusted model, BCG vaccination showed a significant protective effect for infection (OR 0.25, 95% CI 0.09 to 0.69). Similarly, being taught by the index case was an independent risk factor for acquiring tuberculous infection (OR 18.91, 95% CI 4.43 to 80.79, table 2).
BCG vaccine effectiveness
Using the adjusted OR for BCG vaccinated children acquiring TB infection, we calculated a corrected risk reduction14 of 0.34 (95% CI 0.26 to 0.42). Using the formula VE=1−RR, this translates into a vaccine effectiveness of 0.66 or 66%, implying that 21 of the 32 infections could have been avoided if all children had been BCG vaccinated.
Microbiological investigations
DNA fingerprinting using the 15 loci-based Mycobacterium Interspersed Repetitive Units Variable Number Tandem Repeats (MIRU-VNTR) typing scheme15 showed that the M tuberculosis strain (22 233 24 326 14 323, LAM lineage) of the index case was indistinguishable from the strains of two of the adults found to have sputum smear-positive TB. Sputum for culture of M tuberculosis was not available from any of the children.
Discussion
We report extensive transmission of M tuberculosis among very young children with a prolonged exposure to an adult with sputum smear-positive TB. Furthermore, BCG seems to confer a protective effect in children against M tuberculosis infection as assessed by positive IGRA in this cohort.
The UK national BCG immunisation policy was changed in 2005 from universal vaccination of school age children to an approach targeting high-risk infants. This policy change is supported by the International Union against Tuberculosis and Lung Disease consensus statement recommending this change in low-incidence areas,4 16 and the change in TB epidemiology from a disease largely affecting the general population to that concentrated in particular high-risk groups. In addition, studies had indicated that the school programme was no longer a cost-effective public health measure17 18 and the decline in TB incidence in the UK provided further support for the policy change.19 Since 1998 the incidence of TB has increased in the UK, although this increase has been predominantly in high-risk groups.
Individual primary care trusts (PCTs) are responsible for the decision to implement universal or targeted BCG vaccination using recommended national criteria. Because of the high overall TB incidence, the diverse population and the large movement within London, more than half of the 26 PCTs in the city have now changed to a universal infant vaccination policy, including some areas with incidence of TB of <40/100 000. Most of the children in our outbreak cohort lived in the PCTs of Westminster and Kensington and Chelsea, both with a TB incidence of <40/100 000. These two PCTs introduced universal BCG vaccination of infants in 2005 and 2004, respectively, but the coverage is unknown and thought to be low.
Our results are unique in that they measure BCG effectiveness in a UK population in which universal infant vaccination is recommended. This is usually not the case in high-income countries where BCG is instead offered to risk groups. The latter skews the data as the vaccinated population has a higher risk of being exposed to TB compared with the unvaccinated population, leading to an apparent lack of protective effect of vaccination. As the children in this cohort are young, they have not been selected for vaccination following a negative tuberculin skin test result as was previously done with the school age BCG vaccination programme. This would have resulted in an apparent protective effect.
The affluent population affected in this outbreak is not generally perceived as being at appreciable risk of TB. The high international mobility of the group, however, potentially increases the risk of exposure to TB and the probability of being lost to follow-up in vaccination programmes. The majority also seek private healthcare with less close ties to the public health programmes.
It is widely accepted that BCG vaccination reduces the risk of severe forms of TB in infants.8 20 The evidence for the effect of the BCG vaccine on the risk of tuberculous infection is more limited.7 12 Only 42% of the children in this study were BCG vaccinated. This low coverage could be due to the children recently having moved to the area or because universal BCG vaccination for newborns was not actively promoted when these children were born.
Our results suggest that 21 of the 32 paediatric cases of TB infection in this study could have been prevented by BCG vaccination. This should, however, be interpreted with caution. Our current knowledge of IGRA tests does not allow distinction between true latent TB infection and lasting immunological responses after exposure to M tuberculosis infection.21 Emerging evidence suggests that an IGRA test may not always correctly predict progression to active TB, but appears to be a more accurate indicator of the presence of latent TB infection than the tuberculin skin test.22 23 However, IGRA testing provides at least the same or possibly higher sensitivity for detecting those who will progress to active TB compared with the tuberculin skin test.22–24 Due to the young age of the children in this cohort, it seems unlikely that exposure prior to this outbreak is sufficient to explain the high probability of a positive IGRA. Nonetheless, data on IGRA in young children are scarce and should be interpreted carefully.21 Only longitudinal follow-up studies will allow us to distinguish the lasting immunological response from latent infection.
The vaccine effectiveness of 66% found in our study is higher than the 38% reduction in RR found in another UK study9 and the 24% reduction found in a larger and robust study by Soysal et al.12 Overlapping CIs between the studies would suggest that the differences may not be significant. One of the reasons for this difference could be that the other studies investigated latent tuberculous infection in older children who could have acquired their infection prior to the period under investigation in the children. However, the children in the Turkish study12 were also offered BCG vaccination at 2–3 months of age, similar to the children in our study.
One limitation of the study is the lack of information on BCG vaccination status from a part of the study population due to difficulties in coordinating the different private physicians who took care of some of the children. As mentioned above, it was not possible to perform tuberculin skin tests on the children. This might have been done at the same time as the IGRA test to be able to compare the results, as it has been shown that false negative IGRA results do occur.23 24 However, it has been shown that IGRA results are not associated with previous BCG vaccination.10 It should also be noted that the data are from an outbreak investigation and that the findings therefore are not necessarily generalisable to all situations. Furthermore, the study design used in this study can only identify an association between BCG vaccination and reduced risk of infection; only a randomised controlled trial could prove its protective efficacy as such.
Conclusion
We have used IGRA positivity as a measure for M tuberculosis infection and found a protective effect of BCG vaccination. These findings highlight the need to review the evidence for the effectiveness and cost effectiveness of BCG immunisation, in particular with regard to the current TB incidence cut-off level required for universal BCG vaccination in the UK. Owing to the high mobility across the boroughs of the city, we also recommend careful monitoring of TB incidence, BCG vaccination uptake and transfers across PCT boundaries within London among school children. Further research into better markers of latent tuberculous infection and longitudinal follow-up of exposed individuals is needed to find ways to distinguish individuals latently infected with live M tuberculosis from those who have persistent antimycobacterial immune responses without an increased risk of ever progressing to TB.
Acknowledgments
The authors would like to thank all those who took part in the outbreak investigation, in particular Sheena Basnayake, Lesley Ruta, Marie O'Donoghue, Maria Mercer, the TB and paediatric teams at St Mary's and Chelsea and Westminster hospitals and the rest of the outbreak control team. The authors also thank Professor Paul Fine and Dr Doris Radun for reviewing and commenting on the manuscript.
References
Footnotes
Competing interests None.
Ethics approval This study was carried out during an outbreak investigation. The Health Protection Agency has Patient Information Advisory Group approval to hold and analyse communicable disease data for public health purposes under Section 60 of the Health and Social Care Act 2001.
Provenance and peer review Not commissioned; externally peer reviewed.