Article Text

Abstract
Background: There have been difficulties in applying spirometric tests to children of preschool age.
Methods: The feasibility of measuring lung function was examined in 652 children aged 3–6 years using dynamic spirometry with an animation programme and the guidelines approved by the European Respiratory Society.
Results: Data from 603 (92%) children with at least two acceptable forced expiratory manoeuvres were analysed; 408 (68%) achieved at least three acceptable manoeuvres. Children with only two acceptable manoeuvres were younger, shorter, and weighed less (p<0.001). The lower levels of lung function in this group were partly explained by body size. 63% of those with three acceptable manoeuvres had a difference of ≤5% between the highest and second highest forced expiratory volume in 1 second (FEV1); when a difference of ≤10% was applied, 91% of the children were included. A similar trend was seen for forced vital capacity (FVC). The acceptability and reproducibility increased with increasing age, and levels of lung function increased linearly with age. The linear regression model showed that standing height was a satisfactory predictor of lung function; the explained fraction of variance (R2) was 59% for FEV1. Most FVC manoeuvres in children older than 3 years were acceptable and reproducible.
Conclusions: Spirometric testing is feasible in preschool children and may be useful for both clinical practice and research. This study may fill the deficiency in reference values for European preschool children.
- lung function
- spirometric testing
- preschool children
Statistics from Altmetric.com
Measurement of lung function is a well established part of pulmonary medicine, and lung function parameters are used in the diagnosis of respiratory diseases, assessment of clinical status and drug treatment response, as well as in surveillance of patients with a chronic pulmonary disease. The 1992 International Consensus Report on Diagnosis and Treatment of Asthma states that spirometry is recommended in the initial assessment of most patients with suspected asthma.1 Spirometry is also a central method of measuring outcome in respiratory epidemiology. The most commonly used test of lung function is spirometry, especially a set of 3–5 forced vital capacity (FVC) manoeuvres, from which the forced expiratory volume (FEV1) and FVC are measured.2–4 This method and the instruments for performing FVC tests are comprehensively standardised in the guidelines approved by the European Respiratory Society (ERS) and the American Thoracic Society (ATS).3,4 An important application of lung function measurement in epidemiology is to study the genetic and environmental determinants of lung function—either the level in cross sectional studies or the rate of change over time in longitudinal studies—and to assess lung function as a predictor of later disease or disability. It is also important to understand the natural development of lung function parameters over time. A series of large epidemiological studies have provided information on normal development of lung function in adults and schoolchildren.5 Recently, special methods to measure the lung function in newborn infants have also been developed.6 Little is known about the levels and development of lung function in preschool children aged 1–6 years, whereas growth curves are available for tracking a child's FEV1 and FVC from the age of 6 years.7–10 There have been difficulties in using spirometric tests in preschool children, and the validity and reproducibility have been thought to be seriously compromised in this age group whose attention span is short or who may not cooperate appropriately.11,12 The commonly used reference standards such as those of Polgar and Promadhat,13 Zapletal et al,14 and Knudson and co-workers15 have few children below 115 cm standing height and do not include children smaller than 110 cm in height and younger than 6 years of age. However, a recent study of 184 healthy children in the US included preschool children aged 3–6 years.10
Animation programmes for measuring lung function have recently been developed which may minimise the degree of cooperation required of preschool children. The objectives of this study were to examine the feasibility of measuring lung function in preschool children and to estimate how age, height, weight, and sex affect the acceptability of spirometric tests. We focused on forced expiratory flow-volume curves which would be useful in epidemiological studies of preschool children.
METHODS
Study population
The source population constituted all children living in the city of Oslo who attended a day care centre. As part of the Day Care Environment and Health Project, we studied children aged 3–6 years in 24 full time day care centres in Oslo. Of the 919 eligible children, 652 (80%) were present at the day care centre on the days the data collection took place. The regional ethics committee and the data protection registrar approved the study and written informed consent to take part was obtained from the parents on behalf of their children.
Baseline spirometry
Lung function was measured by dynamic spirometry (MasterScreen Pneumo, Erich Jaeger GmbH, Germany) using an animation programme according to the guidelines recommended by the European Respiratory Society (ERS).3 Regular calibration was done with a 1 litre calibration syringe. Two experienced technicians performed the spirometry testing in the day care centres using ananimation programme with illuminated candles and a balloon. The measurements were conducted on one or two days depending on the number of children in each centre. The age of each child was calculated by subtracting his/her date of birth from the date of the testing day. Standing height and weight without shoes were measured using the same equipment and standardised procedures in all day care centres. Children with major signs of upper respiratory tract infections were excluded.
Lung function was measured in February–April 1999. The children were trained in groups of three. First they played with their mouthpiece, blowing through it as fast, hard, and for as long as possible. Individual flow-volume curves were then measured with the subject sitting wearing a nose clip. Calibration, taking into consideration ambient conditions, was conducted after every fifth child. All manoeuvres complied with the general acceptability criteria of the ERS.3 Individual flow-volume curves were reviewed for technical acceptability and were considered unacceptable if: (1) the child waited too long before starting; (2) the child coughed or breathed in during the measurement; (3) the curve was flat or rounded without a distinct peak; (4) the top of the curve was to the right or there was more than one distinct peak. At least three technically acceptable attempts of maximal forced expiratory flow-volume curves were recorded. However, children with at least two acceptable manoeuvres were also included in the analysis.3
The lung function parameters measured were: forced expiratory volume in 1 second (FEV1), forced expiratory volume in 0.5 seconds (FEV0.5), forced vital capacity (FVC), and peak expiratory flow (PEF). Reproducibility of FVC and FEV1 was considered acceptable when the highest FVC and FEV1 value did not exceed the second highest value by more than 5%. The corresponding cut off point was 10% for PEF. The reproducibility criterion was not used to exclude children with a complete test set. Tests that did not meet this criterion were marked so that these data could be analysed separately. The highest reading is reported using the envelope method of reading flows, which means that the highest flow at a given lung volume is chosen, irrespective of the curve.3 The variables are presented as absolute values.
Data analysis
We compared the lung function parameters, age, height, and weight in children with at least three acceptable manoeuvres and those with two acceptable manoeuvres. We also compared the proportion of children with a reproducible measurement of lung function using differences of both 5% and 10% between the highest and second highest measurement of FEV1 and FVC. The role of age as a determinant of level and reproducibility of lung function parameters was measured by comparing four age groups: 3 years (n=143), 4 years (n=201), 5 years (n=201), and 6 years (n=58). Differences between groups were assessed by a two sample t test and a χ2 test.
Linear regression was applied to assess the dependency of the lung function measures FEV0.5, FEV1, FVC, and PEF on the explanatory variables age, height, weight, sex and acceptability of three or more manoeuvres. The effects of sex and acceptability were assessed by indicator variables (1/0). Parental smoking habits and presence of asthmatic symptoms were known in a subset of children (n=476). Not all parents who allowed their children to take part in the spirometric tests returned the 2-week diary and parental questionnaire that included this information. Additional regression models were carried out on this subset taking smoking and asthma into account. The models were compared by the explained fraction of the variance (R2). The regression models were tested for interaction between the two groups and the other explanatory variables (age, height, weight, and sex). The models were also tested for deviation from linear effects of age, height, and weight by means of additive models (GAM)16 and by including square terms of the explanatory variables. An assumption of multiple linear regression models is homoscedastic (constant) variance. This assumption was checked by smoothing of squared residuals on fitted values by means of additive models (GAM). Alternative models in which the lung function measures and/or the explanatory variables were log transformed were also carried out. The predicted values of FEV1 and FVC by height are shown using the equations from this present study and those of Eigen et al10 with 95% prediction limits and 95% confidence limits.
The analyses were conducted using the computer program SPSS version 9.0 (SPSS Inc, Chicago, USA, 1999) and the GAM procedures in S-Plus (MathSoft4, Seattle, 1997).
RESULTS
Lung function was measured in 630 (97%) of the 652 children aged 3–6 years; 22 (3%) children refused to participate. After an evaluation of all flow-volume curves using the acceptability criteria of the ERS,3 analyses were performed on data from 603 (92%) children. In contrast to the ERS criteria, we also included all children with two acceptable manoeuvres.
Table 1 shows the distribution of age, sex, height, weight, and lung function levels for children with at least three acceptable manoeuvres (n=408, 68%) and for those with two acceptable manoeuvres (n=195, 32%). Children with only two acceptable manoeuvres were younger, shorter, and lighter and had lower levels of lung function than those with ≥3 acceptable manoeuvres. The acceptability increased with age (p<0.001) (not shown). Among children aged 3 years, 51% had at least three acceptable manoeuvres compared with 69%, 76%, and 78% in children aged 4, 5 and 6 years, respectively. About 10% of the children were unable to expire for 1 second.
Characteristics of the study population
In general, the reproducibility of lung function parameters was higher in children with three acceptable manoeuvres than in those with two (table 2); 63% of the children with three manoeuvres fulfilled the 5% reproducibility criterion in FEV1 compared with 91% using the 10% criterion. A similar trend was seen for FEV0.5, FVC, and PEF (table 2). Furthermore, the reproducibility increased with age using a reproducibility of ≤5%; this trend was weaker using a difference of ≤10% between the highest and second highest values (table 3).
Percentage of preschool children with a difference between the highest and second highest value of FEV1, FEV 0.5, FVC and PEF of ≤5% and 6–10% in children with at least three acceptable manoeuvres and those with two acceptable manoeuvres
Percentage of preschool children with a difference of ≤5% and 6–10% between the highest and second highest value of FEV1, FEV 0.5, FVC, and PEF by age.
Figure 1 shows the unadjusted means of FEV1, FEV0.5, FVC, and PEF with 95% confidence intervals. The levels of lung function increased linearly with increasing age. This increase was consistent for both children with at least three acceptable manoeuvres and for those with two acceptable manoeuvres. The same trend was seen for height (fig 2).

Level of lung function (FEV1, FEV0.5, FVC, and PEF) by age in children aged 3–6 years. The solid line represents the whole group and includes 95% confidence intervals in each age group. The dotted line represents children with at least three acceptable manoeuvres and the dashed line represents children with two acceptable manoeuvres.
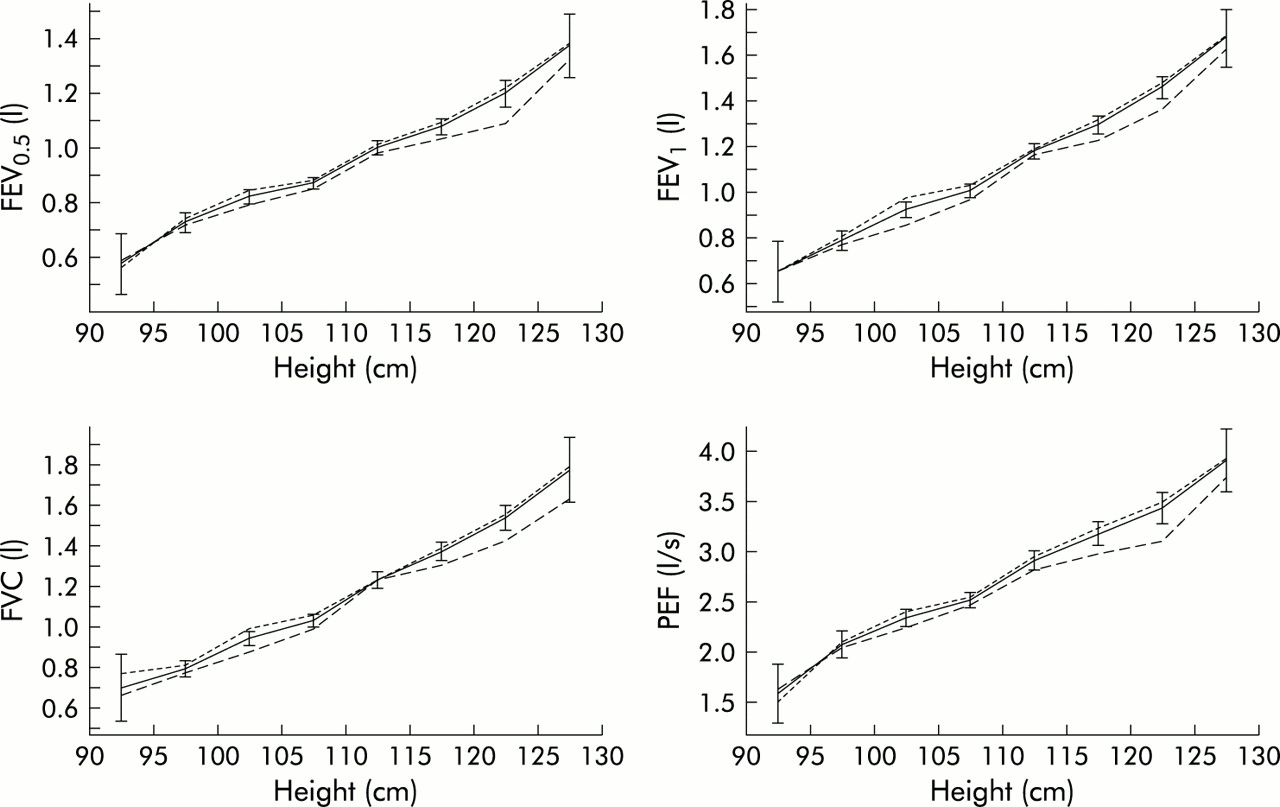
Level of lung function (FEV1, FEV0.5, FVC, and PEF) by height in children aged 3–6 years. The solid line represents the whole group and includes 95% confidence intervals in each age group. The dotted line represents children with at least three acceptable manoeuvres and the dashed line represents children with two acceptable manoeuvres.
Separate simple linear regression models entering only one of the explanatory variables (height, weight and age) were fitted. The largest explained fractions of variance (R2) were obtained for height, which was 59% for FEV1 and FVC (table 4); age accounted for up to 48% and weight up to 40%. The best linear predictor of FEV1 based on a single explanatory variable is thus predicted FEV1 = –1.92 + 0.0277 height (cm) with a standard deviation (SD) of 0.18 (table 4). The distribution of the residuals was in good agreement with a normal distribution. One would therefore expect that about 68% of children of a given height will have values of FEV1 in the interval predicted FEV1 (±SD) and about 95% in the interval predicted FEV1 (±2SD). Similar prediction intervals apply for the other lung function parameters. Also, the z score that can be compared with the standard normal distribution can be computed as, for instance, z = (observed FEV1 – predicted FEV)/SD.
Height as a predictor of lung function parameters for girls and boys given as the results of the crude linear regression analyses Y = β0 + β1h where h = height (cm) and Y = one of the lung volume measures (FEV0.5, FEV1, FVC and PEF). Slope β1 represents the change per cm height
Multivariate regression models on the subset of 476 children with information on parental smoking and asthmatic symptoms showed that neither of these factors influenced lung function. About 30% were smokers, and the prevalence of wheezing during the last 12 months and ever asthma was 23% and 9.7%, respectively. In the multivariate regression analyses on all children, all explanatory variables (height, age, weight, sex, and acceptability of three manoeuvres) had clear significant effects with the exception of the effect of sex on PEF (p=0.18). The improvements in R2 were modest, however (table 5). For example, R2 was 64% in the multivariate analysis of FEV1 and 59% in the analysis with height only. A prediction rule of FEV1 based on all explanatory variables becomes: where h is height in cm, w is weight in kg, a is age in months, m is the indicator of three or more manoeuvres, and b is the indicator of a boy. In this regression model the SD was 0.17 and a 68% (95%) prediction intervals for a new observation becomes the interval predicted FEV1 ± SD (±2 SD).
where h is height in cm, w is weight in kg, a is age in months, m is the indicator of three or more manoeuvres, and b is the indicator of a boy. In this regression model the SD was 0.17 and a 68% (95%) prediction intervals for a new observation becomes the interval predicted FEV1 ± SD (±2 SD).
Predictors of lung function parameters given as the results of adjusted linear regression analyses Y = β0 + β1 h + β2 w + β3 a + β4 m + β5 b, where h = height (cm), w = weight (kg), a = age (months), m = an indicator of three acceptable manoeuvres. and b = an indicator of a boy. Y is one of the lung volume measures FEV05, FEV1, FVC and PEF.
When fitting the data with additive models, significant non-linearity was found on height for FEV0.5, FEV1, and FVC. However, the improvement in R2 was only 0.5%. Almost the same improvement was obtained by including height squared in the regression model. The estimated coefficient of the square term was positive, so there were indications of a convex relationship between lung function measurements and height. Interactions between sex and height were significant for FEV1 and FVC. However, in the crude analysis shown in table 4, the increase in R2 by including sex and the interaction terms was less than 1%. Similarly, inclusion of the interaction term in the adjusted analyses led to improvements in R2 of less than 0.5%. The interactions between acceptability of three manoeuvres and the other explanatory variables were not significant. There were indications that the standard deviation increased with the predicted value. However, for FEV1 this increase was not significant. Log transformation of lung function measurements and/or height gave a similar although somewhat smaller explained fraction of variance. Figure 3 shows the predicted values of FEV1 and FVC by height using the equations from the present study and the values predicted by Eigen et al.10 The figure includes 95% confidence intervals to show the uncertainty in the estimated regression lines and prediction intervals, which should include a new value with a probability of 95%. There is a good overlap between these two studies.

{kind=link}
{kind=link}
{kind=link}
Predicted values of FEV1 and FVC by height using the equations of the present study and that of Eigen et al10 with 95% prediction limits and 95% confidence limits.
DISCUSSION
The results of this study show that spirometry using an animation programme is feasible in children aged 3–6 years. The acceptability and reproducibility were reasonable for the whole age range, but there was a steady improvement with age. The levels of lung function were found to be higher in children with three acceptable manoeuvres than in those with two. This was partly explained by age and body size. Standing height was the best predictor of lung function.
Approximately 80% of all children in Oslo aged 3–6 years attend a day care centre. The willingness to participate in our study was unusually high, and about 80% of the eligible children were present in the day care centres on the days the lung function measurements took place. Most of the absenteeism was accounted for by part time day care attendance and some children were absent because of illness or other activities outside the day care centre. In all, the children included in the present study should be reasonably representative of all children of a similar age.
The quality of lung function measurements depends on the quality of the equipment and the testing procedure. The technicians were trained to follow carefully the standardised technique of recording FEV1 and FVC to reach maximum validity and minimum variability in these recordings. The present testing procedure followed the standardised guidelines of the ERS with regard to equipment, manoeuvres and measurements, as well as acceptability and reproducibility criteria.3 FEV1 and FVC were chosen as the main parameters since these variables are the most widely used measures of ventilatory function, and FEV1 is the most reproducible pulmonary function variable.2–4 The strengths of the present study are consequently that the results were based on tests made with well defined equipment that meets satisfactory demands regarding accuracy and applicability. The children also received instructions and encouragement from two well trained technicians with a lot of experience in lung function measurements in children and adolescents.
Even when the acceptance criteria were satisfied, however, both the FVC and FEV1 may be underestimated. The children in our cross sectional survey had only one measurement session; it has been shown that the reliability increases with subsequent visits.12,17,18 The effect of learning was assessed by Studnicka et al19 during a 15 month follow up of 151 children. The short term lung function variability decreased markedly between the first and second lung function test sessions, but thereafter no further reduction was seen.19 Le Souef et al20 trained inpatients with asthma of preschool age and found that reliable test results were possible in most 4–5 year old children. Children who are well trained will therefore have valid lung function tests. To improve the validity of our tests we used an animation programme with illuminated candles and a balloon because of the specific pedagogic qualities of this programme. The programme motivated the children to breathe in maximally and to deliver maximal force from the beginning to the very end of the exhalation. Furthermore, the children were trained individually before the actual test session to inhale and exhale completely.
Population based studies among preschool children are rare. However, Eigen et al10 have recently evaluated spirometric lung function in 259 normal US children aged 3–6 years attending Indianapolis nursery schools. 82.6% (214/259) were successful in generating technically acceptable flow-volume curves during the first testing session, 95% of whom achieved three technically acceptable curves; about 78% of all the children had three technically acceptable curves.10 In our study 92% were successful in generating technically acceptable flow-volume curves and, when applying the strict acceptability criterion suggested by the ERS (at least three acceptable manoeuvres), altogether 70% of the children reached acceptable values. Our study population (n=603) included 143 children aged 3 years and only 58 children aged 6 years, whereas the population (n=184) studied by Eigen et al10 included mainly children aged 4 years and older up to 7 years. This large difference in sample size and age distribution may partly explain the different findings. Kanengiser and Dozer conducted forced expiratory manoeuvres in 98 children aged 3–5 years with a variety of respiratory disorders before and after bronchodilator treatment.12 Over 90% of the patients cooperated; only 49% (48/98) generated a FEV1 on at least two out of three prebronchodilator and postbronchodilator curves, and less than 50% of the children yielded an acceptable reproducibility of FEV1 by ≤5%.3 In line with the results from previous studies conducted in both adults and children, we found that subjects who did not fulfil the test criteria differed in body size and age.19,21,22 Body size is an indirect measure of lung size and can thus influence lung function parameters. Lung size can also be related to respiratory disease. Furthermore, children with asthma, wheeze, or a positive provocation challenge have a greater variability in lung function than healthy children.19 Exclusion of subjects who fail spirometric tests may bias the results of epidemiological studies. Including a diagnosis of asthma in our regression analysis model did not, however, contribute significantly. We therefore suggest that the ERS criteria of acceptability could be too strict in epidemiological studies which assess determinants of lung function or respiratory diseases related to lung function in preschool children. Less strict recommendations will thus be less influenced by differences in body size, which is a proxy of lung size.
Kanengiser and Dozer found that the reproducibility of FEV1 met ATS criteria—that is, a difference of no more than 5% or 100 ml between the two best manoeuvres—in only 32% of the children; the corresponding figure for FVC was 59%.12 However, using 100 ml as one of the criteria in preschool children will subsequently include children with a difference of about 10% between the highest and second highest measure because of the lung volumes of these children. In our study a difference of at least 10% between the highest and second highest value of FEV1 and FVC included about 90% of children aged 4–6 years. However, in children below 4 years of age there were problems with their attention span and cooperation, and the measurements were less reproducible. Our data corroborate the suggestion that an adaptation of the criteria to include children with a 10% difference between the highest and second highest measurement in population based studies could be required.17,19,23
Another possible recommendation regarding lung function testing in preschool children is to include the use of FEV0.5 as a variable to take into account the fact that a proportion of preschool children empty their lungs in 1 second or less.17,24 This variable had the highest acceptability and reproducibility in the present study. The maximum validity and minimum variability in this recording needs to be further examined.
Much effort has been made to describe the level and development of lung function throughout life. Data on levels of lung function by age are available for children down to 6 years of age.5 Gold et al have estimated the annual increase in the level of lung function by age from 6 to 16 years in US children.25 Our results indicate a linear relation between the level of lung function and age in children aged 3–6 years. The study by Eigen et al10 in 184 healthy US children aged 3–7 years found that all lung function parameters increased with increasing height. In contrast, the results of our study did not show a better fit by log transforming the lung function parameters and height. However, the estimates from our log transformed analyses were similar to those of Eigen et al. A comparison of the predicted values of FEV1 and FVC by height using the equations of the present study with the values predicted by Eigen et al showed good agreement (fig 3). Another recent small study showed very similar results using another computer animated system.26
In line with other studies, we found that standing height is a satisfactory predictor of lung function. However, we also found that inclusion of age, weight, and sex in the model yielded some information. This is partly due to our large sample size. In contrast to the commonly used reference standards such as those of Polgar and Promadhat,13 Zapletal et al,14 and Knudson et al,15 our study included a large proportion of children under 6 years of age and shorter than 115 cm. Ideally, the rate of change in lung function should be estimated from longitudinal studies. Adequate studies to describe the development of lung function in healthy children throughout infancy and the preschool years, or to provide adequate reference data to define abnormality, are still needed.
Thee results of spirometric tests in preschool children using an animation programme are encouraging. Most FVC manoeuvres of children older than 3 years are acceptable and reproducible. Spirometry seems to be feasible in preschool children and potentially useful for both clinical practice and research. This study may fill the deficiency in reference values for European children of preschool age.
REFERENCES
Footnotes
-
This study was supported by grants from the Norwegian Research Council.