Article Text

Abstract
The diagnosis of pulmonary sequestration traditionally requires arteriography to identify abnormal systemic vessels feeding the abnormal portion of the lung. Non-invasive imaging techniques have recently been used to replace arteriography. Conventional computed tomographic (CT) scanning is, however, at a disadvantage because of its inability to obtain multiplanar images. The combination of slip ring CT scanning and computerised three-dimensional reconstruction (spiral CT angiography) can be used to visualise the anatomical detail of a wide range of vessels within the lung. Four cases of pulmonary sequestration are reported which were successfully diagnosed using spiral CT angiography. Spiral CT scanning allows simultaneous imaging of anomalous vessels and lung parenchyma in a single examination and is particularly useful in the diagnosis and assessment of pulmonary sequestration.
- pulmonary sequestration
- spiral computed tomography
Statistics from Altmetric.com
Pulmonary sequestration is a rare congenital pulmonary disorder defined as an area of dysplastic and non-functioning pulmonary tissue with an anomalous systemic blood supply.1 It has been classically described in two forms—intralobar sequestrations located within the visceral pleura and surrounded by normal lung, and extralobar sequestrations which have a separate pleural covering. Both types are supplied with blood from the aorta or its branches. The venous return of the intralobar sequestration is usually via the pulmonary veins while extralobar sequestrations generally have systemic venous drainage. Nevertheless, many variations and combinations of these classical patterns have been described.2
Traditionally, the diagnosis of pulmonary sequestration requires arteriography to identify abnormal systemic vessels feeding the abnormal portion of the lung. More recently, other procedures have been advocated as a less invasive means of identifying the anomalous artery. Although conventional computed tomographic (CT) scanning can show both abnormal lung parenchyma and the systemic arterial supply,3 it lacks the multiplanar images which limits its usefulness in the diagnosis of sequestration. With the advent of helical technology, spiral CT angiography is able to delineate the aorta and its branches. The role of CT scanning in evaluating suspected pulmonary sequestration should therefore be re-evaluated.4
In this report we describe the use of spiral CT angiography to image the aberrant systemic artery in four cases of pulmonary sequestration.
Methods
We performed four CT angiography studies with a PQ2000S helical scanner (Picker International Inc, Highlands Heights, Ohio, USA). Spiral volumetric CT scanning was performed with 4 mm slide thickness, 4 mm table speed, 3 mm reconstruction index, and smooth reconstruction algorithm. A non-ionic contrast medium (120 ml, iodine 300 mg/ml) was administered at a rate of 3 ml/s via the antecubital vein. A 25 second scan delay was used in order to optimise contrast in the systemic arterial phase of the study. Three-dimensional reconstruction (3D) was performed with a Voxel Q work station using a shaded surface display (SSD) program with segmentation option.
Case reports
CASE 1
A 32 year old man with a 34 pack-year history of cigarette smoking who still smoked two packs a day was admitted to the smoking cessation programme at our hospital. There was a history of pneumonia at the age of 14. A chest radiograph showed localised air trapping in the left lower lobe. A spiral CT scan (fig 1) revealed a multicystic lesion in the posterior basal segment of the left lower lobe supplied by an artery derived from the coeliac axis; venous return to the pulmonary veins was also demonstrated. The presence of the anomalous systemic artery and venous drainage were confirmed by aortography. The patient was asymptomatic and refused surgery.

Spiral CT scan of case 1. (A) Contrast enhanced CT axial image showing the small aberrant artery (arrow) adjacent to the upper abdominal aorta (a). (B) Anterior view of helical CT angiogram. The anomalous artery (arrow) feeding the pulmonary lesion (L) arises from the coeliac axis.
CASE 2
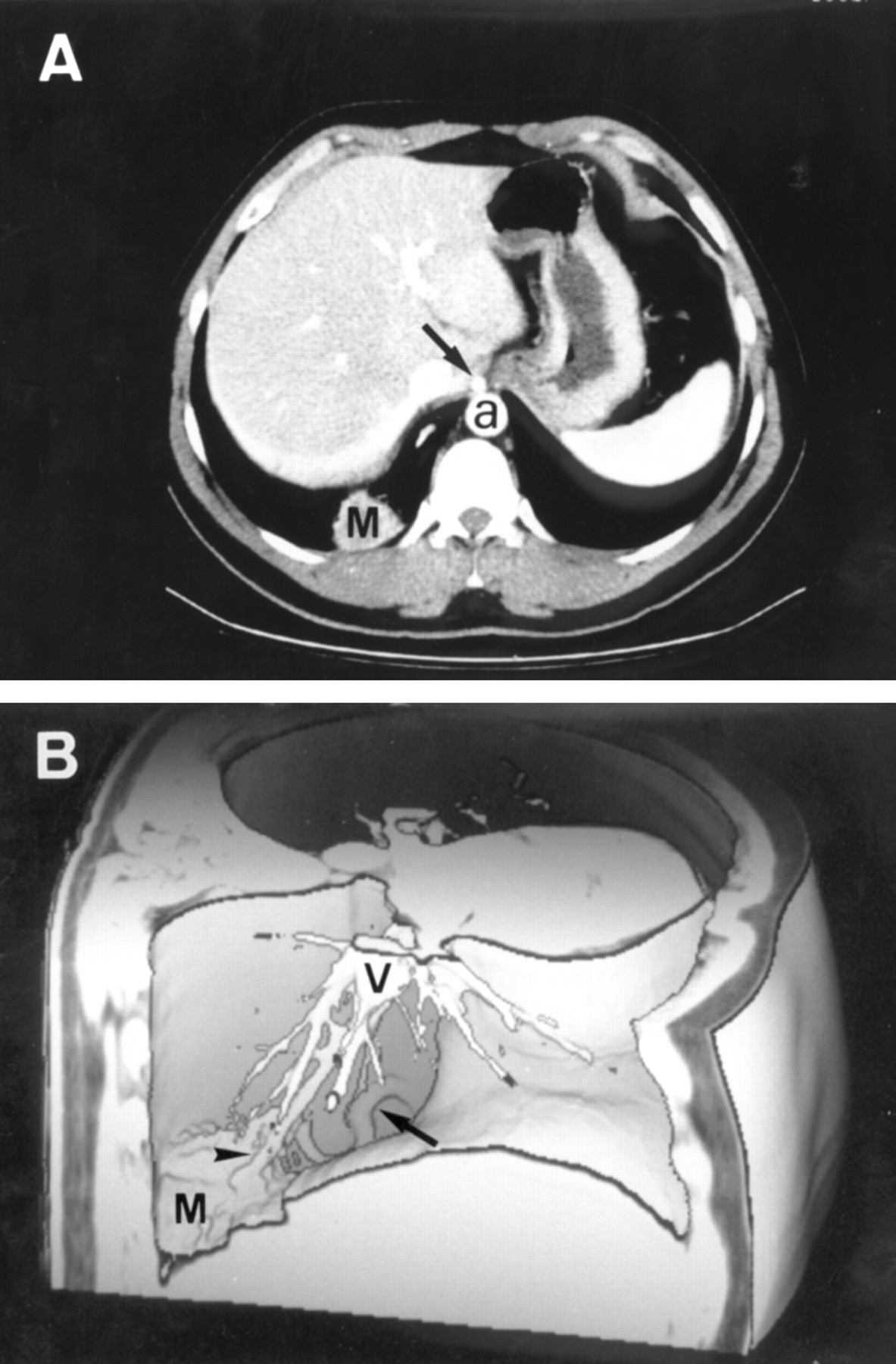
A 28 year old man presented with a one month history of recurrent haemoptysis. He smoked one pack of cigarettes daily. Chest radiography showed a mass, 4 cm in diameter, in the right lower lobe. Bronchoscopic examination indicated that the source of bleeding was the right lower lobe but no endobronchial lesions were seen. A spiral CT scan (fig 2) revealed a homogeneous mass in the right lower lobe contiguous to the diaphragm and identified its anomalous arterial supply derived from the upper abdominal aorta just above the coeliac artery; venous drainage into the pulmonary veins was also visualised. Intralobar pulmonary sequestration was confirmed by aortography and thoracic surgery.

Spiral CT scan of case 2. (A) Contrast enhanced CT axial image showing the pulmonary mass (M) supplied by an anomalous systemic artery (arrow) arising from the upper abdominal aorta (a). (B) Right view of helical CT angiogram showing the course of the arterial vessel (arrow) to the pulmonary mass (M). Note the venous drainage (arrowhead) to the pulmonary veins (V).
CASE 3
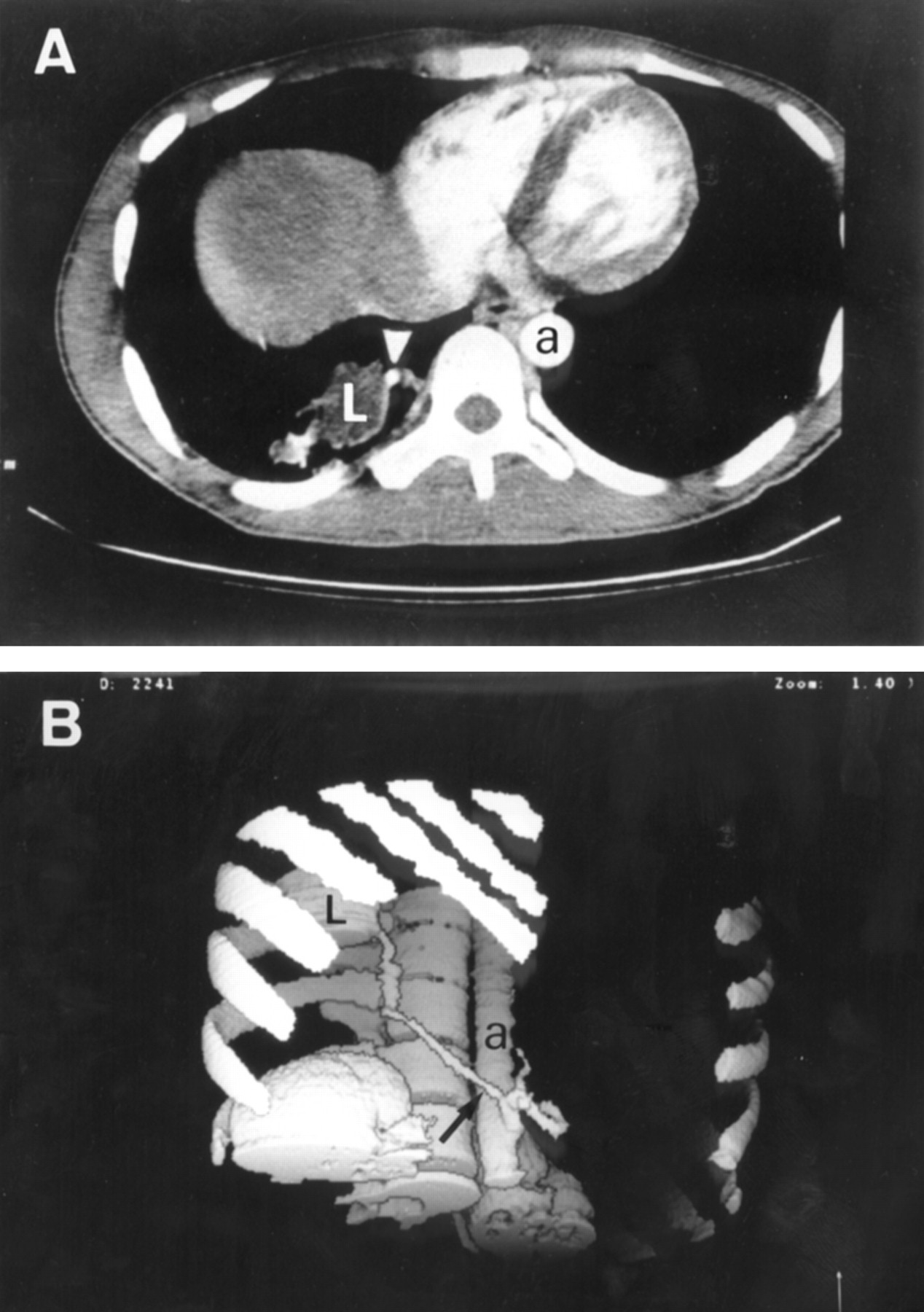
A 65 year old male cigarette smoker had a two week history of productive cough and fever. The patient improved with antibiotic therapy but a persistent cough developed. Radiography of the chest showed partial collapse of the left lower lobe and a mass like opacity with an air-fluid level. A CT scan demonstrated a non-homogeneous mass with multiple cystic appearing spaces and cavitation involving the posterior basal segment of the left lower lobe. Fibreoptic bronchoscopic examination disclosed no abnormality. A percutaneous fine needle aspiration biopsy specimen of the lesion revealed non-diagnostic findings. Spiral CT angiography (fig 3) showed a feeding systemic artery arising from the descending thoracic aorta and venous drainage to the pulmonary veins. At surgery an infected intralobar sequestration was found.

Spiral CT scan of case 3. (A) Contrast enhanced CT axial image showing an anomalous systemic artery (arrow) feeding the pulmonary lesion (L) in the left lower lobe. (B) Left oblique view of helical CT angiogram demonstrating the anomalous artery (arrow) originating from the left wall of the thoracic aorta (a).
CASE 4
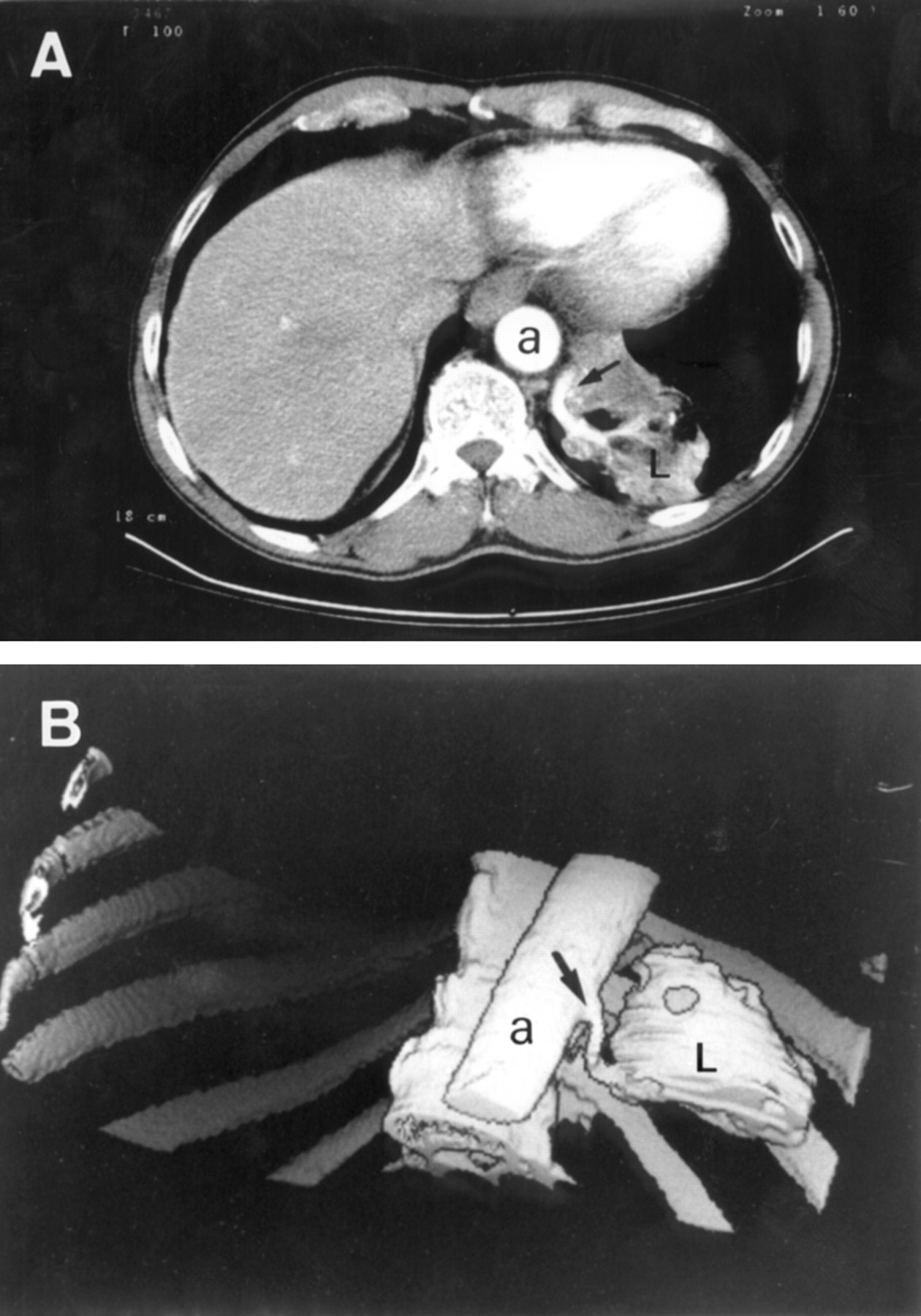
A 41 year old man was admitted to hospital with a 48 hour history of fever and pleuritic chest pain. There was no history of use of tobacco. Chest radiography revealed a homogeneous density in the right lower lobe. He was diagnosed as having pneumonia and treated with clarithromycin. One month later he was readmitted with clinical deterioration, unproductive cough, weakness, anorexia, weight loss, and fever. Chest radiography showed a diffuse and bilateral micronodular pattern with persistence of the right lower lobe density. Miliary tuberculosis was confirmed by histopathological examination of a transbronchial biopsy specimen and positive culture of bronchial aspirate. A spiral CT angiogram (fig 4) revealed a focal area of increased density in the right lower lobe supplied by an artery originating from the coeliac axis. An abdominal aortogram showed the anomalous artery and the venous return via the pulmonary veins. Because the lower pulmonary veins were not included in the upper sections of pre-established contrast enhanced helical CT acquisition, in this case spiral CT angiography could not identify the venous drainage. Surgery was not considered at the time this case was presented.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Spiral CT scan of case 4. (A) Contrast enhanced CT axial image showing a systemic artery (arrowhead) feeding the pulmonary lesion (L) in the right lower lobe. (B) Right oblique view of helical CT angiogram showing the anomalous systemic artery (arrow) arising from the coeliac axis. a = aorta.
Discussion
Both intralobar and extralobar sequestration characteristically involves the lower lobes of the lungs. Intralobar pulmonary sequestration accounts for 73% of all sequestrations and has a predilection for the posterior basal segment of the lower lobes. It occurs slightly more often in the left lung than in the right.2 The blind ending bronchi, which may become distended trapping mucus, are prone to infection. In about two thirds of the cases reported the first symptoms occur after the age of 10 years and are usually secondary to a superimposed infection. Productive cough, fever, haemoptysis, recurrent pneumonia, and chest pain are typical presenting complaints. Extralobar sequestrations are frequently discovered during the neonatal period in infants with other congenital anomalies. The clinical picture is usually dominated by the associated anomalies although infection can occur, especially if there is a communication with the oesophagus or the stomach. Extralobar sequestrations that are not diagnosed in newborn infants are often asymptomatic and detected on routine radiography.
In case 1 pulmonary sequestration was detected by routine radiography, while in case 2 haemoptysis was the presenting symptom of an intralobar sequestration. Case 3 had an intralobar sequestration typically manifested by symptoms of infection and case 4 had concomitant disseminated tuberculosis.
Plain radiographs of the chest often show a single homogeneous opacity or, less commonly, a cystic mass in the base of one lung that can sometimes suggest the diagnosis of sequestration.1 Less specific findings include recurrent pneumonia and focal bronchiectatic changes. The principal objective for diagnosis of pulmonary sequestration is to identify the systemic artery supply. With this information, imaging can distinguish sequestration from other causes of lung opacity. Because accessory arteries, pleural investment, and venous drainage are adequately determined intraoperatively, at some institutions only the presence and location of an aberrant systemic artery are considered essential for preoperative assessment for any symptomatic pulmonary sequestration.4
Imaging strategies for suspected pulmonary sequestration are based on case reports or small series since it is a rare congenital disorder and no study exists that objectively compares imaging techniques for detection, definition, or cost effectiveness.4 Since the definitive step in the diagnosis of sequestration is the demonstration of the systemic arterial supply, for a long time diagnosis was made by conventional angiography. More recently all imaging techniques capable of showing the artery have been implicated in evaluating sequestration. Magnetic resonance (MR) imaging and MR angiography can be used together to diagnose pulmonary sequestration in a single non-invasive examination.5 Nevertheless, MR cannot accurately evaluate lung parenchyma and the airways and must be considered in terms of cost and availability. Sonography requires a favourable acoustic window and is ideally suited for evaluating the chest prenatally and postnatally.6 Other non-invasive techniques for evaluation of sequestration such as scintigraphy are only rarely necessary.
In all four cases described in this report spiral CT angiography successfully delineated the origin and course of the anomalous systemic artery. Axial images were enough to make the diagnosis but three-dimensional reconstruction aided both radiologists and referring clinicians by demonstrating anatomical relationships, particularly for vessels orientated in the z axis.7 On the other hand, venous drainage was also identified in the three cases in which lower pulmonary veins were included in contrast enhanced helical CT scans. We have performed three-dimensional reconstruction (3D-SSD) segmentation for a better understanding of the anatomy of the abnormal systemic arteries. However, as shown in case 2, three-dimensional imaging dedicated to the venous drainage can also be made.8
Spiral CT angiography is a minimally invasive technique for vascular imaging that is made possible by combining slip ring CT scanning and computerised three-dimensional reconstruction.9 Spiral CT angiography has several advantages over other non-invasive vascular imaging techniques.4 10 CT scanning, with its superior spatial resolution, yields the most information about the bronchial anatomy and the pulmonary parenchymal lesion. Sonography and MRI cannot evaluate lung abnormalities accurately although MRI can reveal the cystic nature of many intralobar sequestrations as well as the variable solid, fluid, haemorrhagic, and mucus-containing components. MR angiography is hampered by artefacts caused by respiratory motion whereas this problem is generally avoided in helical CT scanning. CT angiography is less expensive than MR angiography and can be used on patients with a metallic device or who do not tolerate the MR examination. Furthermore, helical CT scanning is faster resulting in less sedation and reduced amount of contrast medium. The disadvantages of helical CT scanning are minor and arise from exposure of the patient to ionising radiation and the administration of intravenous contrast material.
In summary, we report four cases of pulmonary sequestration successfully diagnosed using spiral CT angiography. By allowing simultaneous imaging of anomalous vessels and parenchymal lesions in a single examination, spiral CT angiography is a particularly efficacious technique and has the potential to become the procedure of choice in the diagnosis and assessment of pulmonary sequestration.