Article Text

Abstract
Background: More than 50% of patients initially resuscitated from out-of-hospital cardiac arrest die in hospital.
Objective: To investigate the prognostic value of serum protein S-100 and neuron-specific enolase (NSE) concentrations for predicting (a) memory impairment at discharge; (b) in-hospital death, after resuscitation from out-of-hospital cardiac arrest.
Methods: In a prospective study of 143 consecutive survivors of out-of-hospital cardiac arrest, serum samples were obtained within 12, 24–48 and 72–96 hours after the event. S-100 and NSE concentrations were measured. Pre-discharge cognitive assessment of patients (n = 49) was obtained by the Rivermead Behavioural Memory Test (RBMT). The relationship between biochemical brain marker concentrations and RBMT scores, and between marker concentrations and the risk of in-hospital death was examined.
Results: A moderate negative relationship was found between S-100 concentration and memory test score, at all time points. The relationship between NSE and memory test scores was weaker. An S-100 concentration >0.29 μg/l at time B predicted moderate to severe memory impairment with absolute specificity (42.8% sensitivity). S-100 remained an independent predictor of memory function after adjustment for clinical variables and cardiac arrest timing indices. NSE and S-100 concentrations were greater in patients who died than in those who survived, at all time points. Both NSE and S-100 remained predictors of in-hospital death after adjustment for clinical variables and cardiac arrest timing indices. The threshold concentrations yielding 100% specificity for in-hospital death were S-100: 1.20 μg/l (sensitivity 44.8%); NSE 71.0 μg/l (sensitivity 14.0%).
Conclusions: Estimation of serum S-100 concentration after out-of-hospital cardiac arrest can be used to identify patients at risk of significant cognitive impairment at discharge. Serum S-100 and NSE concentrations measured 24–48 hours after cardiac arrest provide useful additional information.
- cardiac arrest
- hypoxia–ischaemia (brain)
- cognitive function
Statistics from Altmetric.com
Before the implementation of pioneering out-of-hospital resuscitation initiatives in the 1970s, survival from out-of-hospital cardiac arrest was uncommon.1 Defibrillation initiatives and public cardiopulmonary resuscitation (CPR) training have increased the number of people with cardiac arrest who survive to discharge.2–4 Despite these advances, most centres report in-hospital mortality rates of around 50%.5 6 More than one-third of patients who survive to discharge have cognitive deficits which are severe enough to hinder daily activities.7
Prognostic assessment of patients with cardiac arrest is challenging. Clinical scoring systems may be limited in ventilated patients, and neurophysiological methods such as somatosensory evoked potentials require specialist interpretation.8 Recently, estimation of serum concentrations of brain proteins has shown promise as a method of predicting in-hospital death.9 10 Protein S-100 is an astroglial protein which is released after stroke and cardiac arrest.11–20 This marker may have clinical utility in identifying cardiac arrest survivors with severe brain injury and a poor prognosis. Neurone-specific enolase (NSE) is a neurone-derived enzyme which is also released after stroke and cardiac arrest, and merits further evaluation.16–18
Memory impairment affects up to 40% of cardiac arrest survivors. Until now, studies have tended to focus on mortality and broad indices of neurological function. Identification of patients with sublethal brain injury may help clinicians target rehabilitation resources at those who are likely to have cognitive impairment. Neither NSE nor S-100 have been specifically evaluated as predictors of cognitive impairment in patients who survive. In this study we have evaluated S-100 and NSE as prognostic markers of two end points: (a) cognitive function at discharge, using an extensively validated test of episodic long-term memory and (b) death.
PATIENTS AND METHODS
Study patients
In a prospective study we identified 148 initial survivors of out-of-hospital cardiac arrest, of cardiac aetiology, admitted to the Royal Infirmary of Edinburgh, UK. Patients were enrolled over 36 months from June 1999. The catchment population is about 650 000. Approximately 320 cardiac arrests are attended by the emergency services annually. Of these, about half are cases of witnessed ventricular fibrillation, for whom the survival rate to discharge is historically 12%. The principal outcome measures in this study were memory test score (described below) and in-hospital mortality. Exclusion criteria were organic brain disease, psychiatric illness, use of psychotropic medication, stroke. Systemic cooling was not an available local treatment at the time this study was conducted.
Sampling protocol
Blood sampling time points were based on data from published studies10 13: time A (within 12 hours of cardiac arrest), B (24–48 hours) and C (72–96 hours).
Sample storage and analysis
Samples were centrifuged, serum frozen at −40°C, and analysed within 4 months. Serum S-100 concentration was measured by an immunoluminometric assay (Sangtec, Bromma, Sweden).19 The antibody recognises the β-subunit of S-100. The limit of detection was 0.05 μg/l where the intra-assay impression exceeds a coefficient of variation (CV) of 10%. Interassay CVs were 8.3% at 0.3 μg/l (n = 10) and 3.3% at 11 μg/l (n = 10). The upper limit of the reference range in healthy subjects is 0.2 μg/l. NSE concentration was measured by an enzyme immunoassay on the ES300 analyser (Roche Diagnostics, Lewes, UK).20 The detection limit was 4 μg/l. Interassay CVs were 6.8% at 4.9 μg/l (n = 10) and 5.0% at 13.6 μg/l (n = 10). The upper limit of the reference range in healthy subjects is 14 μg/l.
Cognitive assessments
Cognitive assessment was performed by a trained research nurse within 24 hours of planned discharge.8 The Rivermead Behavioural Memory Test (RBMT) score was the principal cognitive outcome measure.21 This test of episodic long-term memory identifies memory difficulties encountered during daily living using 12 subtests. Memory performance was categorised according to age-adjusted normative data: normal (22–24 points), mild (17–21 points), moderate (11–16 points) and severe (<11 points) memory impairment. Age-adjusted scores are unaffected in patients after myocardial infarction who have not had a cardiac arrest.7 Short-term memory (working memory) was assessed using the digit span test (from the revised Wechsler Memory Scale).22
We examined the following covariates: age, social deprivation (using Carstairs and Morris postcode scores23), affect (Hospital Anxiety and Depression questionnaire24). The National Adult Reading Test (NART) was used as an index of premorbid intelligence.25 This test was chosen since performance is relatively unaffected by other forms of dementia.
Clinical scoring system
To determine whether NSE and S-100 concentrations provided additional predictive information over clinical assessment, all patients were assessed using a clinical prognostic scoring system which has been previously validated in the same catchment population.7 The scoring criteria are (a) arrest rhythm not ventricular fibrillation or ventricular tachycardia: +3 points; (b) CPR not given by trained bystander: +1 point; (c) Glasgow Coma Score (GCS) 4 or 5 on admission: +1 point; GCS 3 on admission: +2 points.
Timing indices
Time indices were identified using the Heartstart Scotland database. Timings were obtained to the nearest minute from the ambulance dispatcher and from the memory of the defibrillators.
Statistical analysis
Spearman rank correlation (rs) was used to examine relationships between cognitive scores and brain marker concentrations, and between these variables and age, NART, Hospital Anxiety and Depression questionnaire, and social deprivation scores. The Mann–Whitney test was used to compare brain marker concentrations between survivors and those who died, and between survivors with RBMT scores above 16 points, and scores of 16 points or less. Receiver operating characteristic (ROC) analysis was used to estimate sensitivity and specificity values for each marker.
Multiple logistic and linear regression methods were used to identify which factors independently predicted (a) in-hospital mortality, and (b) RBMT scores, after adjusting for one another. For this analysis NSE and S-100 results were log transformed because of their skewed distributions. A prespecified analysis was applied to the subgroup of patients admitted with significantly impaired consciousness (GCS ⩽ 6) on admission, since this is the group in which prognostic tests have the most widespread clinical application.
The study protocol was approved by the Lothian Research Ethics Committee.
RESULTS
Subject characteristics
One hundred and forty-eight cardiac arrest victims were admitted during the study period. One hundred and forty-three (106 male and 37 female) were eligible for the study. Three were excluded because of previous stroke, one because of dementia, and one refused to participate. Mean age was 68.2 (range 32.2–94.2) years. Table 1 summarises the baseline characteristics. Most cardiac arrests were witnessed ventricular fibrillation events. Causes were deemed by the attending cardiologist to be: acute myocardial infarction (67 cases, 46%), ischaemic heart disease with left ventricular impairment (29 cases, 20%), acute myocardial ischaemia without infarction (16 cases, 11%), other (31 cases, 21%). Ten patients died in the emergency room before blood samples could be taken. Samples were obtained at time A in 133 cases. Most in hospital deaths occurred within 72 hours of admission, so samples at times B and C were obtained in 105 and 69 cases, respectively. No samples were omitted other than when the patient had died.
Of patients where samples were obtained, 56/133 subjects (42%) survived to discharge and 49 of these (87%) consented to cognitive testing. There was no significant difference in age, comorbidity, or estimated cardiac arrest duration between those who consented and those who did not. Median (range) time to cognitive testing was 8 (5–26) days. Mean (SD) NART score was 30.4 (9.9), within the expected range. No significant differences were found in demographic variables between patients who survived and those who died, consistent with previous observations.7 No significant associations were noted between any baseline patient variables, affect, premorbid intelligence or social deprivation and either brain marker concentrations or memory test scores. Episodic long-term memory was moderately impaired in 15 (30.6%) and severely impaired in 13 (26.5%) of subjects, consistent with previous data.7
Brain proteins and pre-discharge memory function
No significant correlations were noted between either of the markers and digit span test score. Spearman’s correlation coefficients for RBMT profile score versus S-100 concentration at each time point were: time A: rs = −0.349, p = 0.015; time B: rs = −0.480, p = 0.001; time C: rs = −0.318, p = 0.033. For time B (fig 1), the S-100 threshold value that gave the greatest combined sensitivity and specificity for moderate to severe memory impairment (RBMT profile score ⩽16 points) was 0.16 μg/l (specificity 86%, sensitivity 59%). The threshold S-100 concentration that gave 100% specificity for moderate to severe memory impairment was 0.29 μg/l (sensitivity 42.8%).
Correlation coefficients for RBMT score versus NSE concentration at each time point were not significant: time A: rs = −0.015, p = 0.917; time B: rs = −0.304, p = 0.035; time C: rs = −0.241, p = 0.111.

Multivariate analysis of brain enzyme concentrations and memory function
There was a significant correlation between depression score and RBMT score (rs = −0.287, p = 0.003), and between clinical prognostic score and RBMT score (rs = −0.34, p = 0.021). There was a negative correlation between age and RBMT score (rs = −0.41, p = 0.003). Anxiety, NART score, deprivation score and timing indices did not correlate significantly with the RBMT score. Multiple regression included S-100 and NSE concentrations for time B (since this time point provided the best correlations between these markers and RBMT score) and also incorporated age, social deprivation score, NART and clinical prognostic score. NSE and S-100 concentrations were significant independent predictors of outcome (time B: NSE p<0.05; S-100 p<0.01; 95% confidence intervals for change in RBMT score corresponding to doubling of marker concentration: NSE −6.6 to −1.0; S-100 –3.1 to −0.7; adjusted r2 = 0.33). Age, deprivation score, NART score and clinical score did not provide additional prognostic information.
Brain proteins and in-hospital mortality
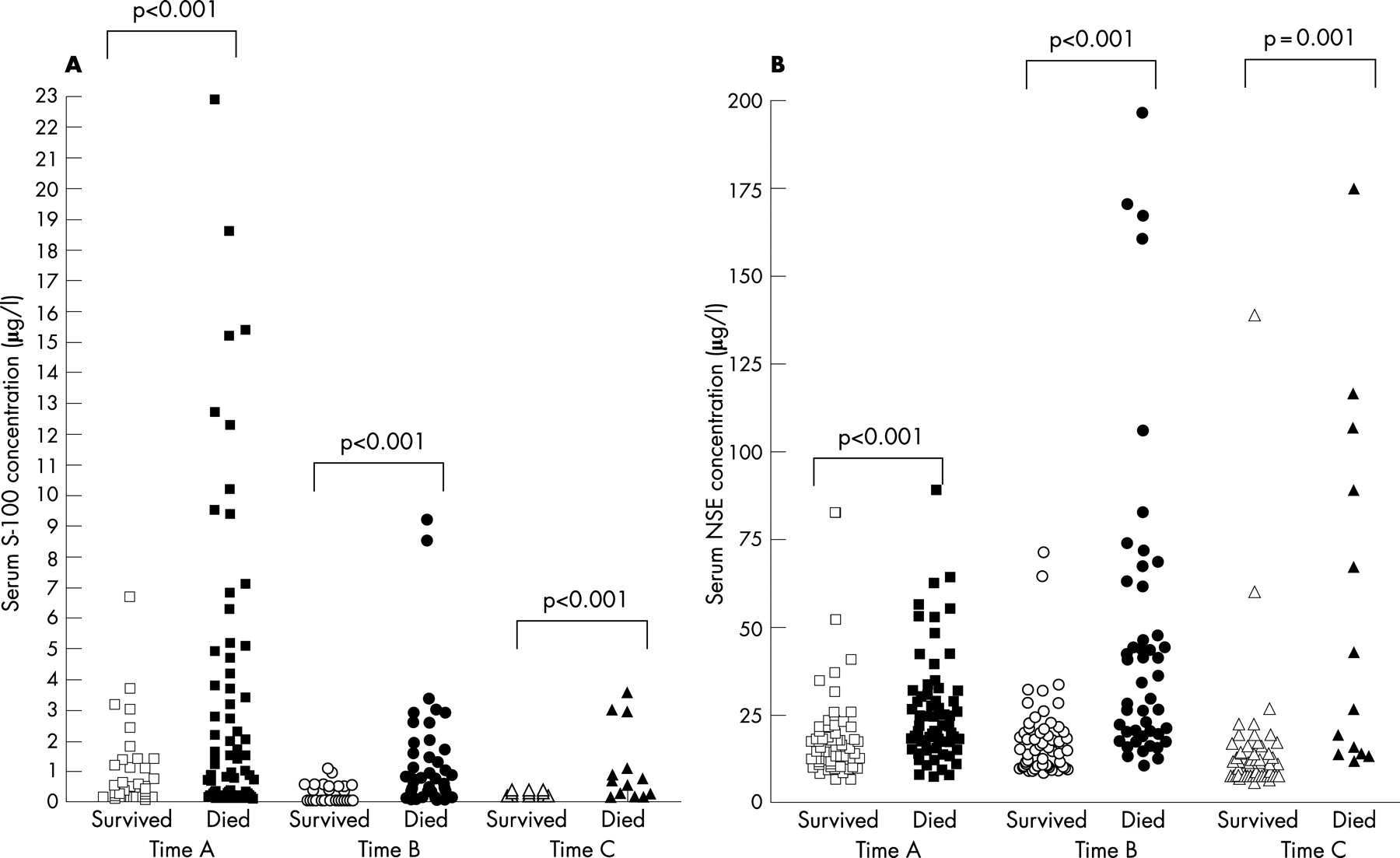
At all three sampling time points, serum NSE and S-100 concentrations were significantly greater in patients who died than in survivors (table 2 and fig 2). NSE and S-100 remained predictors of in-hospital death after adjustment for clinical variables and timing indices. ROC analysis (fig 3) gave area under the curve values for S-100—time A: 0.614; time B: 0.733; time C: 0.811 and for NSE—time A: 0.662; time B: 0.810; time C: 0.885. (Note that samples taken at times A, B and C represent different groups; for example, sample C does not include patients with severe neurological injury who died within the first 72 hours.) For time B, a threshold serum S-100 concentration of 0.29 μg/l yields 73% sensitivity and 76% specificity for in-hospital death. A threshold NSE concentration of 24.0 μg/l gives 60% sensitivity and 86% specificity for in-hospital death. Serum concentrations which gave 100% specificity for in-hospital death were for S-100: 1.2 μg/l (sensitivity 44.8%) and for NSE: 71.0 μg/l (sensitivity 14.0%). For time C (effectively predicting late (>72 hours) in-hospital death), a threshold S-100 concentration of 0.23 μg/l gives 70% sensitivity and 88% specificity for late in-hospital death. A time C S-100 threshold of 0.44 μg/l had 100% specificity for in-hospital death (sensitivity 53%). A threshold NSE concentration of 16.0 μg/l gives 70% sensitivity and 81% specificity for in-hospital death.

{kind=link}
{kind=link}
{kind=link}
Multivariate analysis of brain protein concentrations and mortality
Multiple logistic regression analysis confirmed that each of the three components of the clinical score independently predicted in-hospital mortality at p<0.05 or less. The clinical score alone was a highly significant predictor of mortality (p<0.001). Both NSE and S-100 concentrations derived from time B remained significant predictors of mortality (S-100: p = 0.037; NSE: p = 0.004) when included separately with the clinical score in the multiple logistic regression. NSE was independently significant after adjusting for the clinical score and S-100 concentration. The area under the curve of the ROC function derived from the multiple logistic regression coefficients and defined by the formula: clinical score + 4 × log10 (NSE time B) was 0.905.
Subgroup with low Glasgow Coma Score
One hundred and twelve patients (78%) were admitted with a Glasgow Coma Score of 6 or less. NSE and S-100, assessed 24–48 hours after cardiac arrest, remained significant predictors of in-hospital death in this subgroup, after adjustment for the clinical score. The NSE concentration was independently significant after adjusting for the clinical score and S-100 concentration.
NSE and S-100 within-patient trends
Not all patients at time A survived to time B or time C, so the data in table 2 do not reflect the concentration trend within the same patients. Within the group of patients who survived at least 72 hours (n = 69), median (range) S-100 concentrations were time A: 0.28 (0.01–9.50) μg/l; time B: 0.16 (0.00–2.60) μg/l; time C: 0.12 (0.00–3.00) μg/l. Median (range) NSE concentrations were time A: 14.4 (6.6–82.5) μg/l; time B: 16.9 (8.3–170) μg/l; time C: 11.7 (7.3–175 μg/l.
DISCUSSION
This study has shown that estimation of serum concentrations of S-100 and NSE can be used to predict both cognitive deficits and in-hospital death in cardiac arrest survivors. These markers provide prognostic information additional to that gained from clinical assessment and cardiac arrest time indices.
Cognitive deficits
Identification of patients at risk of cognitive impairment is important, since deficits may hinder rehabilitation. Although in some cases cognitive function improves after discharge, our group previously identified that important, persistent cognitive deficits affect nearly 40% of patients—an important consideration as around half of cardiac arrest survivors in the UK are eligible to drive and half are of working age.3 7
NSE estimation provides insufficient sensitivity to detect differences between cognitively impaired and intact subjects. S-100 estimation at 24–48 hours provided useful prognostic information, correlating significantly with memory indices. S-100 concentrations >0.29 μg/l identified a subgroup of patients with significant impairment of working memory at the time of discharge from hospital. Memory impairment does not necessarily impinge on all aspects of memory function. The dissociation between preserved working memory (eg, ability to immediately recall numbers using the digit span test) and impaired episodic long-term memory has been previously described.7 Deficits in episodic long-term memory interfere with the ability to transfer new information from working memory to long-term memory, thus affecting retention of information and rehabilitation. These deficits are not necessarily obvious unless actively sought, but have a significant impact on patients’ function. Future studies will examine the effects of cardiac arrest on aspects of cognitive function other than memory.26
Timing indices did not correlate well with RBMT score. Two factors may contribute to this—estimates of “down time” by bystanders may be quite inaccurate, and there may exist a threshold effect in the relation between cerebral hypoxia and cognitive function. No association was found between estimated premorbid intelligence (NART score) and RBMT score. Only three patients had a NART score in the range which might have a major negative impact on performance in memory tests (<15 points).
In-hospital death
Accurate prediction of the likelihood of survival of a cardiac arrest victim is valuable because it aids decision making about treatment and about whether further resuscitation is appropriate. Even when interventional management policies are instituted, around 50% of patients die in hospital, often after a protracted admission to an intensive care environment.5–7 This has significant implications for use of hospital resources, as well as for the patient and relatives. An ideal prognostic test should provide high specificity for in-hospital death, so that treatment is not denied to patients who might then survive. Prediction of the likelihood of survival can be made using coma score ratings or a prognostic scoring system based on clinical findings, but these assessments lack specificity unless they are applied at least 3–4 days after the cardiac arrest.7 8 27 28 Electroencephalogram and somatosensory evoked response measures are a useful adjunct to clinical assessment, but lack specificity within the first 2 days of cardiac arrest, can be affected by sedative drugs such as benzodiazepines and require specialist interpretation.29
A previous study reported that NSE concentrations exceeding 33 μg/l at any time within a week of cardiac arrest had sensitivity of 80% and specificity of 100% for persistent coma.16 For S-100, reported thresholds for predicting in-hospital death have varied, with 24-hour concentrations of 0.2 μg/l and 0.7 μg/l derived from these studies.10 18 These studies did not determine whether NSE and S-100 provide independent prognostic information additional to that provided by clinical assessment or from cardiac arrest time indices.
The American Academy of Neurology recently conducted a systematic review and produced a guideline for predicting outcome in comatose cardiac arrest survivors.30 That guideline states that “serum NSE levels >33 μg/l at days 1–3 after CPR accurately predict poor outcome” and also that “there are inadequate data to support or refute the prognostic value of other serum markers”.
In this study we found that both NSE and S-100 predicted in-hospital death, independent of clinical factors and cardiac arrest timing indices. S-100 is likely to be more useful in the clinical setting because of its better specificity. A threshold concentration of 1.0 μg/l was required to achieve 100% specificity 24–48 hours after cardiac arrest, higher than previously published thresholds.10 21 For NSE, a threshold concentration of 71 μg/l gives 100% specificity for in-hospital death, but with lower sensitivity than in previous reports. Possibly, differences in comorbidity between study groups led to more patients dying in this study despite low NSE levels. For both markers, the sensitivity of the test for predicting in-hospital death was relatively low at the threshold that gave high specificity. This is not surprising, since patients with good neurological function can succumb to cardiac death. Also, mode of death may be multifactorial in unconscious patients, with heart failure, and non-cardiac variables contributing. These were not systematically examined in the present study.
Useful prognostic information can therefore be obtained by measuring serum concentrations of brain proteins between 24 and 48 hours after cardiac arrest. A group of patients with no likelihood of survival can be identified using the thresholds described above. Prognostic information about late in-hospital death can also be obtained, particularly using S-100—no patient survived to discharge if the 72-hour S-100 concentration exceeded 0.44 μg/l. Furthermore, significant cognitive impairment at discharge can be predicted from the S-100 estimation. Thus, S-100 and NSE have a potentially useful clinical role in the assessment of hypoxic brain injury in cardiac arrest survivors. Using commercial kits, (ElecSys S-100 and NSE, Roche Diagnostics Ltd, Lewes, UK) results could be made available within a few hours of sampling. Long-term follow-up of this cohort will determine whether S-100 estimation identifies patients at risk of chronic memory deficits.
Acknowledgments
This study was funded by a 3-year grant awarded by the Chief Scientist Office, a division of the Scottish Executive.
REFERENCES
Footnotes
Competing interests: Dr NR Grubb was reimbursed for consultancy work for St Jude Medical between 2005 and 2006. He was also reimbursed for consultancy work for CardioDigital, a signal analysis company, between 2003 and 2006. Dr Grubb does not hold shares in either company.
- Abbreviations:
- CPR
- cardiopulmonary resuscitation
- CV
- coefficient of variation
- GCS
- Glasgow Coma Score
- NART
- National Adult Reading Test
- NSE
- neurone-specific enolase
- RBMT
- Rivermead Behavioural Memory Test
- ROC
- receiver operating characteristic