Article Text

Abstract
Background Inhaled hypertonic saline (HTS) improves quality of life and reduces pulmonary exacerbations when given long term in patients with cystic fibrosis (CF). While increasingly being offered for acute pulmonary exacerbations, little is known about the efficacy in this setting.
Objectives The authors examined the tolerability and efficacy of HTS use among adult subjects hospitalised with a CF pulmonary exacerbation and hypothesised that use of HTS would improve pulmonary function during the admission.
Design Pilot retrospective non-randomised study.
Setting Single tertiary care centre.
Participants 45 subjects admitted to the inpatient service for acute CF pulmonary exacerbation in 2006–2007. A subset of 18 subjects who were also admitted in 2005 when HTS was not available was included in the comparative study.
Primary outcome Change in forced expiratory volume in one second from admission to discharge.
Secondary outcomes Change in weight from admission to discharge and time to next exacerbation.
Results Mean age was 32.5 years, and mean length of stay was 11.5 days. HTS was offered to 33 subjects and was well tolerated for a total use of 336 days out of 364 days of hospital stay. Baseline demographics, lung function and sputum culture results were comparable in first and second visits. Use of HTS was not associated with an improvement in forced expiratory volume in one second (p=0.1), weight gain (p=0.24) or in the time to next admission (p=0.08).
Conclusions These pilot data suggest that HTS is well tolerated during CF pulmonary exacerbation but offers no clear outcome benefits. It is possible that HTS may not have much advantage above and beyond intensive rehabilitation and intravenous antibiotics and may add to hospital costs and treatment burden.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Long-term use of inhaled HTS improves pulmonary function and decreases exacerbation frequency in patients with CF.
Despite lack of available data regarding efficacy and safety, inhaled HTS is frequently used during hospitalisation for exacerbation of CF pulmonary disease.
Key messages
This retrospective non-randomised study suggests that inhaled HTS is well tolerated during hospitalisation for exacerbation of CF pulmonary disease.
Short-term (14 days) use of inhaled HTS provided no added improvement over standard care (intravenous antibiotics and chest physical therapy) in pulmonary function, weight gain or time to next hospitalisation.
Strengths and limitations of this study
This study allowed within-patient comparison of standard treatment with or without inhaled HTS in a relatively homogeneous adult population in an inpatient setting.
The main limitation of this study is the retrospective and non-randomised design and unavailability of detailed compliance and side effect data. Sample size was adequate for the objectives of the study.
Background
Lung disease is the leading cause of morbidity and mortality in patients with cystic fibrosis (CF). It is characterised by chronic bacterial colonisation and recurrent infections of the airways, which have been evident manifestations of the disease since the term ‘cystic fibrosis’ was first coined.1 2 Mutations in the CF transmembrane conductance regulator gene result in defective epithelial chloride transport in human airway epithelia, but the downstream consequences of this defect and how they result in CF lung disease remain to be further elucidated.3 4 The clinical course of patients with CF is characterised by periods of ‘stable’ disease, interspersed by recurrent exacerbations during which symptoms such as sputum production and cough tend to acutely increase in intensity and are associated with increased bacterial density in the lungs and hypoxaemia.5–8
During acute CF lung disease exacerbation, usual treatment involves intravenous antibiotics, enhanced nutritional supplementation and airway clearance therapies (eg, frequent chest physiotherapy, inhaled albuterol, aerobic exercise).7 9 Inhaled rhDNase can improve pulmonary function when used long term, albeit at a relatively high cost.10–12 Inhaled hypertonic saline (HTS) is an attractive addition because it is inexpensive, fairly well tolerated and acutely increases whole-lung mucus clearance. Long-term treatment with inhaled HTS has been shown to improve pulmonary function and decrease exacerbation frequency.13–18 However, HTS use during an exacerbation may be potentially more harmful by causing more bronchospasm or haemoptysis. To our knowledge, no studies have examined the safety profile and efficacy of inhaled HTS treatment given during CF pulmonary exacerbation.
In this pilot retrospective study, we examine the impact of HTS use among a cohort of adult subjects hospitalised with CF pulmonary exacerbation compared with the same group of subjects during a previous exacerbation when HTS was not used. We hypothesised that use of inhaled HTS in addition to standard care during hospitalisation for acute exacerbation of CF would result in greater improvement in common end points such as pulmonary function, body weight and the time to next exacerbation when compared with standard of care.
Methods
The study was approved by the University of Iowa Institutional Review Board (200710793). This is a retrospective chart review of all adult admissions for CF lung disease exacerbation at the University of Iowa Hospitals and Clinics during the years 2006 and 2007 when inhaled HTS was first offered to patients. Standard care consists of intravenous antibiotics chosen based on the most recent sputum culture and susceptibility testing, nutrition supplementation, pulmonary rehabilitation and intensive mucus clearance techniques such as chest physical therapy four times per day. Study subjects had a diagnosis of CF based on a sweat chloride test or a nasal voltage test, and genotyping of the CFTR gene. For the comparative study, data were abstracted from the admission during which HTS (‘second visit’) was first used and compared with an earlier admission in the previous year (2005) in which HTS was not used (‘first visit’).
Variables studied include age and gender, body mass index on admission and discharge, duration of hospitalisation, intravenous antibiotics use, CF mutation, use of chest physical therapy, sputum culture results, time to next exacerbation and HTS use during subsequent hospitalisations. Baseline pulmonary function values were obtained from testing performed on admission day or in the previous 7 days. During admission, pulmonary function testing was performed twice a week. One subject was discharged after 2 days with a peripherally inserted central catheter to complete antibiotics at home. Subjects received an inhaled β2 agonist to minimise the risk of bronchospasm followed by a 4 ml dose of 7% HTS solution twice daily through a Pari LC nebuliser (PARI Respiratory Equipment, Midlothian, VA, USA). Compliance data are reported as total days of HTS use per total hospitalisation days in the study population. For the comparison study, only subjects who used HTS at least 7 days were included. Main outcome variable of comparison was change in per cent of predicted forced expiratory volume in one second (FEV1) from baseline to discharge. Subjects who failed to reach 90% of their best per cent of predicted FEV1 in the 6 months previous to hospitalisation were defined as non-responders to therapy.19 Other outcomes analysed include length of stay, compliance, time to next admission and weight gain.
Power analysis
Power analysis suggested a paired sample size of 18 patients to detect a change of 10.9% in FEV1 (primary outcome) or weight with a conservative between-group SD of 16%, with 80% power at two-tailed α of 0.05. Observed power analysis for primary and secondary outcomes is detailed in the Discussion section.
Outcomes analysis
Data were analysed using Prism 5 for Mac OS (Graphpad Software) and SAS V.9.2 (SAS Institute). Power analysis was performed using Statmate (Graphpad Software). Univariate data are reported as means and SD and proportions. Paired t test was used for comparisons using a 5% level of significance. Mixed models for repeated measures were used to compare FEV1 change from baseline in the comparison study. Fisher's exact test was used to compute p value of contingency analysis of ‘non-responders’ and ‘responders’ in both visits and to analyse categorical data in table 1.
Patient characteristics during admission*
Results
Study participants
Between January 2006 and December 2007, 45 subjects were admitted to the CF inpatient service at the University of Iowa Hospitals and Clinics. Mean age at admission for this subject population was 32.5±10.1 years, and mean length of stay was 11.1±4.1 days (p>0.05, unpaired t test). Forty-six per cent of these subjects were men. Of the 45 subjects, 25 had an admission in the previous year. All 25 subjects had pulmonary function testing performed around time of admission and at discharge. Of these 25 subjects, 18 had no history of asthma or recent haemoptysis and thus inhaled HTS was offered. These 18 subjects were therefore included in the comparative study as described in the Methods section. Baseline characteristics at admission for subjects who fulfilled inclusion criteria into the comparative study are shown in table 1. During the entire study period, use of HTS at home prior to admission was uncommon (0% of subjects during the first visit and 5% during the second visit). The proportion of patients using inhaled tobramycin or rhDNase was similar prior to both admission (p>0.05), and the prevalence of colonisation with Pseudomonas aeruginosa or Staphylococcus aureus was also similar in both admissions (p>0.05).
HTS is well tolerated by the majority of subjects hospitalised for acute exacerbation of CF
During the study period, inhaled HTS was offered to 34 out of 45 subjects, of whom 33 used it for at least 1 day. The remaining 11 subjects were not offered inhaled HTS due to history of asthma or recent haemoptysis. Among 33 subjects, there was a collective use of HTS for a total of 336 days out of 364 days of hospitalisation. Of the 28 total discontinuation days, 24 were explained by side effects (wheezing and mild haemoptysis) in two subjects. Twenty-seven subjects used HTS for more than 7 days. These data suggest that inhaled HTS is well tolerated by subjects hospitalised for exacerbation of CF lung disease.
HTS does not improve pulmonary function during hospitalisation for acute exacerbation of CF
Among the 18 subjects included in the comparative study, average change in percentage predicted FEV1 from baseline to discharge (in percentage points) was 12.2% (95% CI 7.7% to 16.5%) when HTS was not used and 8.9% (95% CI 4.9% to 12.9%) when HTS was used (figure 1A), suggesting that inhaled HTS resulted in decreased improvement in FEV1 at discharge (p=0.02, 95% CI 0.5% to 5.9%). However, the mean percentage predicted FEV1 at admission was higher when HTS was used (p=0.04) (figure 1B), while the average discharge FEV1 values were not significantly different (p=0.46) between the two visits (figure 1C). The data suggest that the decrease in FEV1 improvement when inhaled HTS was used is therefore likely due to a higher admission FEV1 during that hospitalisation. A mixed-model adjustment for the differences in FEV1 at baseline showed no changes in FEV1 improvement when inhaled HTS was used (p=0.10). Next, we analysed the number of subjects who failed to reach at least 90% of their best per cent FEV1 in the 6 months prior to admission at the end of hospitalisation. This strategy attempts to minimize the confounding effects of week-to week variability in FEV1.19 Four subjects were ‘non-responders’ when HTS was not used and two when HTS was used (p=0.65). Overall, these data suggest that use of inhaled HTS during hospitalisation for exacerbation of CF lung disease does not result in improved or worsened FEV1 over standard of care in this small population.
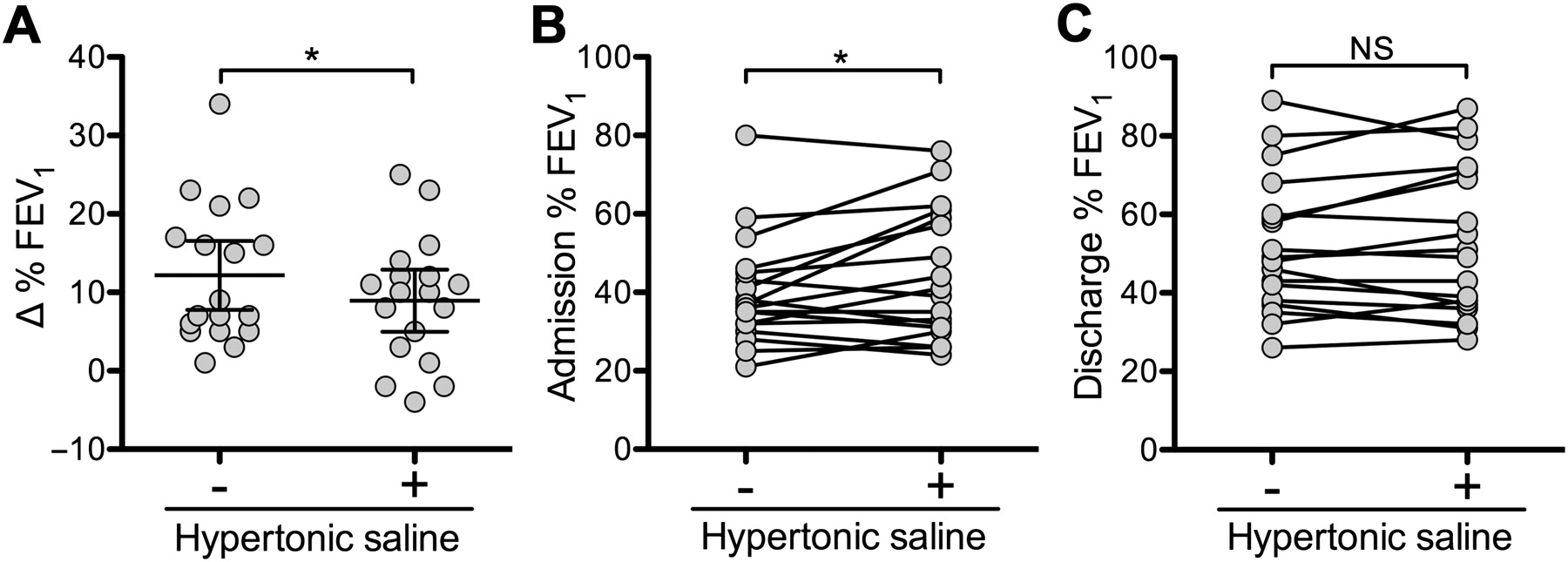
Forced expiratory volume in one second (FEV1). The admission (year 2005) in which hypertonic saline was not used (−) was compared with the admission (year 2006 or 2007) in which hypertonic saline was used (+). (A) Change from admission to discharge FEV1. Units are change in total percentage of predicted. Mean ± 95% CI are shown. Per cent predicted FEV1 at admission (B) or discharge (C). Units are percentage of predicted. Lines join data from both visits for the same subject. n=18. *p≤0.05; NS, p>0.05.
HTS does not augment weight gain during hospitalisation for acute exacerbation of CF
In our experience, subjects hospitalised for exacerbation of CF lung disease gain weight during the visit, probably as a result of enhanced caloric intake and/or control of the inflammatory state in the lungs resulting from infection. Figure 2 shows that the addition of inhaled HTS was not associated with an improved or worsened weight gain during hospitalisation. Average weight gain was 3.4% (95% CI 0.44% to 6.3%) when HTS was not used and 1.5% (95% CI −1.3% to 4.3%) when HTS was used (p=0.24, 95% CI −1.4 to 5.0).

Change from baseline weight. The admission (year 2005) in which hypertonic saline was not used (−) was compared with the admission (year 2006 or 2007) in which hypertonic saline was used (+). Units are per cent change in weight from admission to discharge. n=18. Data = mean ± 95% CI. NS, p>0.05.
HTS does not increase time to next admission after an acute exacerbation of CF
Since inhaled HTS was used during hospitalisation but not as outpatient in our clinical practice through this study period and in the year 2008, we were able to study the effect of inpatient HTS on time to next admission for pulmonary exacerbation. Average time to next admission was 247 days when HTS was not used (95% CI 154 to 340 days) and 176 days when HTS was used (95% CI 98 to 253 days). Figure 3 shows that HTS was associated with decrease time to next admission, but this decrease is not statistically significant (p=0.08, 95% CI −9.8 to 152.7). Failure of increase in the time to next admission is probably related to short-term use of HTS in this study.

{kind=link}
{kind=link}
{kind=link}
Time to next admission. The admission (year 2005) in which hypertonic saline was not used (−) was compared with the admission (year 2006 or 2007) in which hypertonic saline was used (+). Units are number of days between discharge and next admission with a diagnosis of acute exacerbation of cystic fibrosis lung disease. n=18. Data = mean ± 95% CI. NS, p>0.05.
Conclusions
In this retrospective pilot study of subjects hospitalised for exacerbation of CF lung disease, use of inhaled HTS was not associated with additional benefit over standard treatment, which includes intravenous antibiotics, enhanced nutritional supplementation and airway clearance therapies. Two recently published studies showed that inhaled HTS improved outcomes in subjects with CF presumably by hydration of airway surface liquid and improved clearance of airway secretions. HTS can improve pulmonary function and mucus clearance in patients with stable CF lung disease even when used for a short time (2 weeks).13 20 In a large, multicentre randomised controlled trial of stable subjects with CF, twice daily inhalation of 7% HTS over 48 weeks was shown to decrease exacerbation frequency compared with isotonic saline.15 The decrease in exacerbation frequency can also be observed in later stages of the disease.21 The only study of inpatient use of HTS to our knowledge is a study of hospitalised infants with viral bronchiolitis, where nebulised 3% HTS was well tolerated and reduced length of stay significantly.22 In another recent study, 7% HTS was found to be safe and well tolerated in infants with CF.17
Patients admitted for exacerbation of CF lung disease have been offered inhaled HTS as an adjunct to conventional therapy in our institution (and others-verbal communication). The decision to use inhaled HTS is based on the premise that the benefit will outweigh the risk of adverse events (which have been minimal in most studies) and the low cost and ease of administration of this agent.10–12 14 15 23–26 However, inhaled HTS can induce cough10–12 14 20 23 24 26 in human subjects and has been used to provoke bronchoconstriction.25 27 In previous studies of inhaled HTS for CF, cough and dyspnoea have been the reasons for discontinuation of use and exclusion from study.14 20 23 24 Increased airway inflammation could cause hospitalised patients to be particularly susceptible to HTS-induced bronchospasm. One of the primary aims of this study was to examine the tolerability of HTS in this high-risk population. We did not observe an increased incidence of bronchospasm or worsening obstructive physiology when HTS was used.
A recent analysis of risk factors that are associated with failure to recover to spirometric baseline (at least 90% of the best FEV1 in the 6 months previous to an exacerbation) after intravenous antibiotic treatment reported that approximately 25% of subjects fail to recover at least 3 months after the episode.19 In our study, four out of 18 subjects failed to recover to spirometric baseline at discharge when HTS was not used, whereas two out of 16 failed to do so when HTS was used. This analysis also fails to demonstrate significant benefit of using HTS during acute exacerbation of CF, although the data from both studies are not directly comparable since patient populations with different characteristics are analysed.
Why were we unable to detect any improvement in pulmonary function tests or weight gain in this group of CF inpatients? In contrast to previous studies,13 15 this group of subjects do not present with stable lung disease. In a patient with acute exacerbation who is already receiving maximal treatment including intravenous antibiotics, chest physical therapy and rhDNase, the additional benefit of HTS could be trivial because of a ceiling effect. The fact that admission FEV1 during the visit in which HTS was used was generally higher while discharge FEV1 was similar in both visits also supports a possible ceiling effect, in which only a certain degree of improvement may be possible, even with maximal therapy.
Limitations of this study include retrospective nature of data collection from a single institution and unavailability of detailed compliance and side effect profiles. Due to its inherent retrospective nature, this study is non-randomised and does not benefit from intention-to-treat analysis. Although we examined several variables such as FEV1, sputum microbiology and co-interventions, there may be other unmeasured biases between the two admission time periods that may have diluted or masked the treatment effect. Observed power analysis reveals that our sample size and data distribution allow us to detect a difference of at least 3.6% FEV1 (primary outcome) between admission and discharge FEV1 with 80% power (18 pairs, SD between groups of 5.44). These data will be useful for adequate power analysis prior to future related studies. The sample size is too small to allow subgroup analysis based on factors, such as baseline FEV1 and age. For the secondary outcome of weight gain (14 pairs, SD between groups of 5.65), our sample size allows detection of 4.23 kg in weight gain difference between admissions. In the case of time to next admission (18 pairs, SD between groups of 163.44), which was a more variable outcome, our sample size allows detection of a change of 107 days or more. The absence of increased weight gain from using HTS during hospitalisation could be the result of insufficient follow-up time, although a long-term study also failed to demonstrate a benefit.15
This study also highlights an important clinical dilemma in CF patient care. In the last decade, at least five new agents have shown benefits compared with placebo.28 These valuable, placebo-controlled randomised control trials for new treatments, however, do not analyse synergy or interaction with other therapies. In real-world applications, the clinician must apply ‘new’ therapy in conjunction with standard treatments (eg, airway clearance techniques) and other relatively new therapies (eg, rhDNase). Questions such as ‘How should the clinician prioritise these therapies?’ and ‘Are there important interactions between these therapies?’ have been raised by those writing consensus documents for CF practice.29 The results of the current study demonstrate the importance of addressing these questions in well-planned clinical trials since the outcomes of ‘uncontrolled’ combinations in clinical practice are unpredictable. A recently registered prospective randomised controlled trial (ANZCTR # ACTRN12605000780651) may provide clearer answers regarding the role of inhaled HTS during hospitalisation for exacerbations of CF lung disease.
In conclusion, in this study, use of inhaled HTS during hospitalisation for acute exacerbation of CF was not associated with FEV1 improvement, additional weight gain or increased time to next admission over standard treatment in this retrospective study. The question of whether clinicians should offer or withhold this treatment to patients hospitalised for an exacerbation of CF will require a well-controlled therapeutic combination type studies showing added efficacy without added burden. As new therapies are expected, the CF research community will increasingly face the dilemma of how to combine/prioritize multiple effective treatments.
Acknowledgments
The authors thank Drs Joseph Zabner and Michael Welsh for insightful discussion, Dr Bridget Zimmerman for guiding our statistical analyses and Janice Launspach and Rebecca Beek for excellent assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
To cite: Pezzulo AA, Stoltz DA, Hornick DB, et al. Inhaled hypertonic saline in adults hospitalised for exacerbation of cystic fibrosis lung disease: a retrospective study. BMJ Open 2012;2:e000407. doi:10.1136/bmjopen-2011-000407
Contributors AAP, DAS, DBH and LD contributed to the overall concept, design and interpretation of the study, data collection and manuscript preparation. All authors read and approved the final manuscript. LD guarantees the accuracy of data presented in this study.
Funding This work was supported by the National Institutes of Health (grants K23 HL75402-5, U01 HL102288-01 and K08 AI076671).
Competing interests None.
Ethics approval Ethics approval was provided by the University of Iowa Institutional Review Board (200710793).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data in this study.