Article Text

Abstract
Background: Residential proximity to highways is a potential proxy for exposure to traffic-related pollution that has been linked to adverse birth outcomes. We evaluated whether proximity to highway interacts with individual and neighbourhood socioeconomic status (SES) to influence birth outcomes.
Methods: The study population consisted of all live singleton births in Montréal, Canada, from 1997 to 2001 (n = 99 819). Proximity was defined as residing within 200 m of a highway. Neighbourhood SES was measured for census tracts as the proportion of families below the low-income threshold. Individual SES was represented by maternal education. Using multilevel logistic regression, the odds of preterm birth (PTB), low birthweight (LBW) and small-for-gestational-age (SGA) birth were calculated for mothers residing in proximity to highways, accounting for individual and neighbourhood SES. Effect modification between SES and proximity to highway was tested for each outcome.
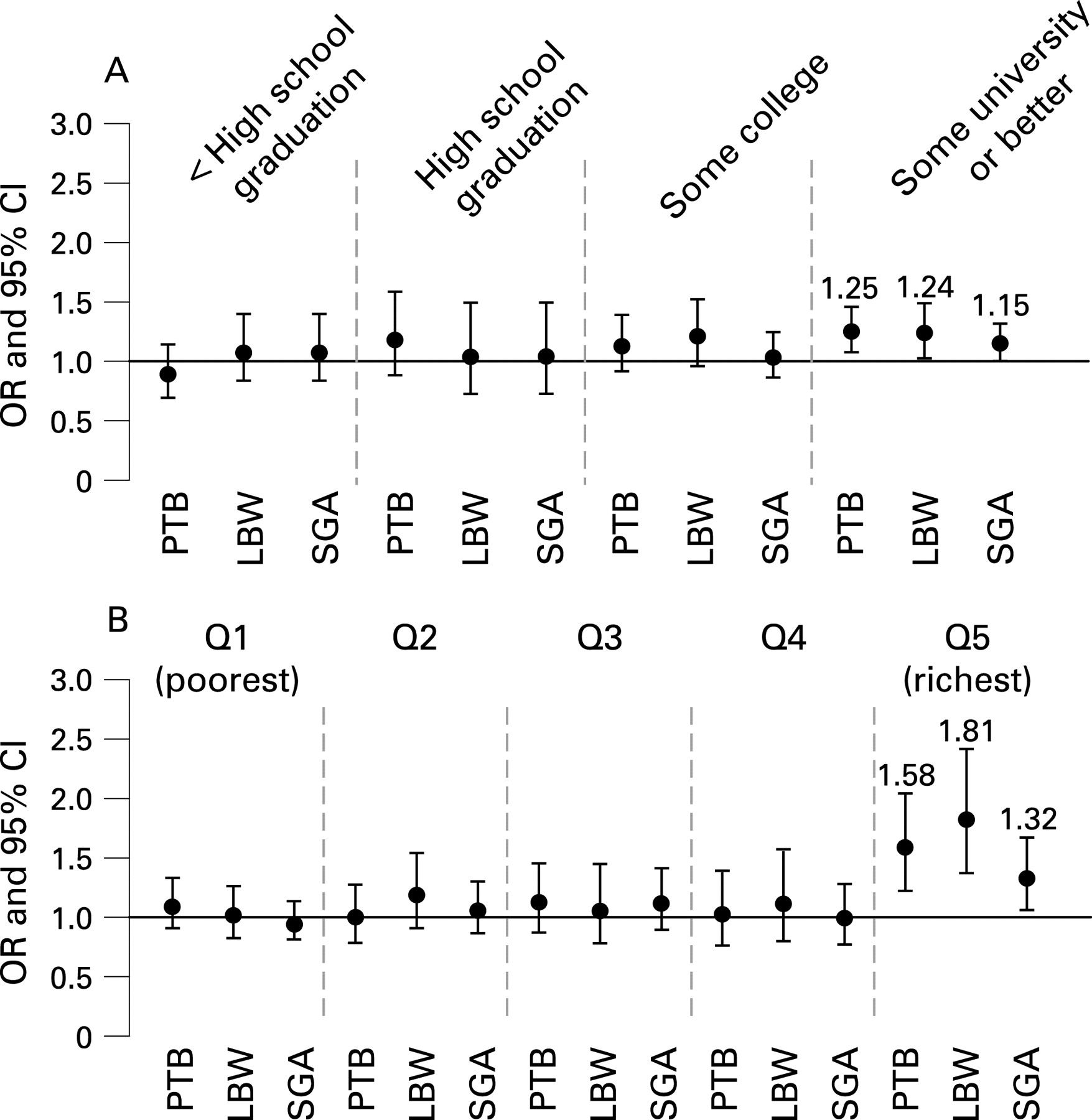
Results: In wealthy neighbourhoods, proximity to highway was associated with an elevated odds of PTB (OR 1.58, 95% CI 1.23 to 2.04), LBW (OR 1.81, 95% CI 1.36 to 2.41) and SGA birth (OR 1.32, 95% CI 1.05 to 1.66). For highly educated mothers, proximity to highway was associated with PTB (OR 1.25, 95% CI 1.07 to 1.46) and LBW (OR 1.24, 95% CI 1.03 to 1.49), but the association was borderline for SGA birth (OR 1.15, 95% CI 1.00 to 1.32). Proximity to highway was not associated with birth outcomes in other maternal and neighbourhood SES categories.
Conclusion: Counterintuitively, high SES mothers may be more likely than low SES mothers to experience adverse births associated with residential proximity to highway.
Statistics from Altmetric.com
Maternal exposure to air pollution is associated with adverse birth outcomes.1–7 These observations are based on studies that use average pollutant concentrations at fixed ambient monitoring stations to estimate maternal exposure.1–6 While such measures reflect exposure to air pollution at regional levels, they account poorly for small-scale spatial variation. In the absence of direct measures of emissions, the use of surrogate traffic-related measures can facilitate analyses, particularly as vehicular traffic emissions contribute appreciably to air pollution.8 Indeed, a number of studies have shown that residential distance to highway and traffic density are associated with various health outcomes.7 9–13
Use of distance to highway has advantages over use of traffic density measures for the investigation of traffic-related pollution and adverse birth outcomes. First, marked changes in pollution concentration can occur over short distances,14 15 and these may not be captured by traffic density measures. Second, the associations between traffic density and health outcomes such as childhood asthma have been inconsistent, whereas this is not the case for distance to highway.11 Third, the influence of distance to highway on newborn health is supported by a study that found short distances were associated with an elevated likelihood of preterm birth (PTB), accounting for maternal socioeconomic status (SES).7
Associations between pollution and health may be subject to confounding by SES, which must be evaluated and accounted for.16–18 Some studies suggest that traffic-related pollution and individual and neighbourhood SES are correlated,13 19 and newborn health is itself associated with maternal and neighbourhood SES.20–22 Furthermore, the results of two different studies suggest that neighbourhood SES might modify and not simply confound relations between pollution and birth outcomes in urban areas.23 24 Mothers living in deprived neighbourhoods might be differentially susceptible to pollution compared with mothers living in affluent neighbourhoods. In these two studies, however, pollution exposure was measured with an index of traffic density rather than distance to highway. In each study, neighbourhood poverty modified the influence of traffic density such that mothers in low SES areas were more likely to experience PTB and LBW relative to mothers in high SES areas.23 24 Effect modification by SES of the role of traffic-related pollution on newborn health is supported by evidence that proximity to highway interacts with SES to influence mortality and hospital admissions.25 26 To date, no study has simultaneously considered distance to highway and individual and neighbourhood SES in relation to adverse birth outcomes.
The present study tested the hypotheses that residential proximity to highway is associated with PTB, LBW and SGA birth, and that neighbourhood and individual SES modify these relationships.
METHODS
Study subjects and setting
We extracted from the Québec birth registry 99 819 live singleton infants born in Montréal, Canada, from 1997 to 2001. Montréal is a large urban city with documented variability in traffic-related air pollution and socioeconomic conditions.14 27 28 The study was restricted to the island of Montréal to increase the probability of a constant background ambient pollutant concentration over the area.
Proximity to highway
Distance (in metres) between residence and nearest highway was calculated as follows. First, the six-digit postal code of the mother’s residence at the time she gave birth was geocoded into latitude and longitude coordinates using PCCF+ 4G version software (Statistics Canada, Ottawa, Canada, http://www.statcan.ca). Second, the geographic coordinates of Canada’s national road network were obtained from the 2005 Road Network File (Statistics Canada, Ottawa, Canada, http://www.statcan.ca), precise up to 10 m. Highways were defined as expressways operating under the principle of controlled access (ie a road having a maximum speed limit of at least 70 km/h).29 Roadways with intersections controlled by stop signs or traffic lights and designed for low-speed operation of motor vehicles were excluded. Third, the Euclidean (straight line) distance between residential and highway coordinates was calculated using MapInfo Professional 8.0 version software (MapInfo, Troy, New York, USA, http://www.mapinfo.com). Only highways on the island of Montréal were used in calculations. We defined residential proximity as a distance of 200 m from a highway. The rationale for this decision was based on research indicating that major air pollutant concentration decreases begin to occur at 200 m.14 Our choice of the 200 m mark was further supported by a preliminary evaluation of the dose–response relation between different distances to highway (eg 100 m, 200 m and 300 m cut-offs) and adverse birth outcomes. A 100 m cut-off did not yield precise effect estimates, and a 300 m cut-off was not associated with birth outcomes.
Maternal and infant characteristics
Maternal education (<11 years, 11 years, 12–13 years, ⩾1 years) was used as the indicator of individual SES.30 Education cut-points are based on the Quebec educational system, where less than 11 years corresponds to not having a high school diploma, 11 years indicates high school graduation, 12–13 years corresponds to some college or preuniversity studies, and 14 years and over represents at least some university studies. Covariates available for extraction included: age (<20 years, 20–34 years, ⩾35 years); marital status (legally married versus other); maternal country of birth (Canada versus other); birth order (firstborn versus subsequent births); history of previous stillbirth (yes versus no); infant sex; and year of birth.
Missing values for maternal education (n = 7109) were imputed as the mean maternal education for the six-digit postal code of the mother’s place of residence. Newborns with missing maternal country of birth (n = 1317) were coded as “other” to maximise statistical power. Final analyses were rerun after excluding births with imputed maternal education or missing country of birth.
Neighbourhood SES
Census tracts were used to represent neighbourhoods because they have been found to correspond to natural neighbourhood boundaries in Montréal.31 The six-digit residential postal code was used to link births to census tracts. The proportion of families in census tracts living below the low-income cut-off (income level at which families spend 20% more than the average on food, shelter and clothing) was calculated using 2001 Census data.20 32 Census tracts were ranked into quintiles according to neighbourhood poverty.
A small number of births could not be assigned distance or neighbourhood values because of invalid postal code information or because neighbourhood data were not available (n = 610). Hence, the data analysed included 99 209 births within 506 census tracts. The mean (standard deviation) number of births per census tract was 196 (±115) (range 10 to 690 births).
Outcomes and statistical analysis
Outcome variables were PTB (gestational age <37 completed weeks), LBW (<2500 g) and SGA birth (<10th percentile based on updated Canadian birthweight for gestational age and sex reference values).33 PTB, LBW and SGA birth could not be determined for 31, 29 and 122 births, respectively, because of missing or implausible data. We created one final file for each outcome which excluded missing values (PTB n = 99 178, LBW n = 99 180, SGA birth n = 99 087). Gestational age <22 and >44 weeks (n = 62) and birthweight <500 and >5000 g (n = 232) were considered extreme but plausible values. We analysed the data both including and excluding these values. Because the results did not differ, we report results including these extreme values.34
Multilevel logistic regression was used to calculate crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) for adverse birth outcomes according to proximity to highway. Census tracts were specified as a random effect. For each outcome, a null two-level model was tested (births within census tracts). The initial null models were followed by a second model containing proximity to highway, and a third model containing proximity to highway and individual and neighbourhood variables (without interaction). A fourth model contained individual and neighbourhood variables, and specified either a cross-level interaction term between proximity and neighbourhood SES or a within-level interaction term between proximity and individual SES. A last model entered both interaction terms simultaneously.
Intraclass correlation coefficients (ICC) were calculated using the latent variable method, with median odds ratios (MOR) and proportional change in variance (PCV) also computed.35 The MOR and PCV are measures of variation useful for assessing the importance of cluster units (“neighbourhood” in this case) for binary outcomes. A MOR represents the likelihood of an adverse outcome that a mother would have, in median, were she to move to a higher risk neighbourhood. The PCV measures the relative change in area-level variance between less and more complete models.35
Analyses were undertaken using SAS 9.0 with the GLIMMIX macro for binary outcomes (SAS Inc., Cary, NC, USA, http://www.sas.com).
This study was conducted as part of work to monitor and research population health in the province of Québec, Canada, as mandated by the Health Ministry and approved by the Québec public health ethics committee.
RESULTS
In our sample, 6.3% of births were PTB, 4.6% were LBW, and 9.2% were SGA. Mothers residing within 200 m of a highway (6.0%) had a higher frequency of PTB (7.0%), LBW (5.3%) and SGA birth (9.8%) relative to mothers residing further away (table 1). The frequency of adverse birth outcomes was positively associated with neighbourhood poverty and inversely associated with maternal education.
Table 2 displays frequencies and crude ORs for proximity to highway according to maternal education and neighbourhood SES. The odds of living within 200 m of a highway were highest in the poorest neighbourhoods (OR 1.87) compared with mothers in the wealthiest neighbourhoods. Compared with university-educated mothers, mothers of lower education status were also more likely to live in proximity to highway.
Table 3 shows associations between proximity to highway, SES and birth outcomes for the crude and adjusted models (excluding effect modification). Proximity to highway was more strongly associated with PTB (adjusted OR 1.14, 95% CI 1.02 to 1.27) and LBW (adjusted OR 1.17, 95% CI 1.04 to 1.33) than with SGA birth (adjusted OR 1.06, 95% CI 0.96 to 1.17). Comparison of crude and adjusted models shows the association between proximity and birth outcomes was robust. Highly educated mothers and mothers residing in high SES neighbourhoods had lower odds of adverse outcomes, and these were more protective for LBW than for PTB and SGA birth.
Proximity to highway did not explain much area-level variation, as shown by the stability of measures of neighbourhood variation (ICC, MOR and PCV) when comparing crude with null models (table 3). The MOR showed that a mother would, in median, increase her odds of all adverse birth outcomes by 12–13% should she move to a higher propensity area. The PCV from table 3 reveal minimal changes in neighbourhood variance after adding proximity to highway to null models.
Effect modification was present between (a) proximity to highway and neighbourhood SES and (b) proximity to highway and maternal education, in separate models. Figure 1 illustrates the adjusted odds of adverse birth outcomes for proximity to highway according to maternal education and neighbourhood SES. In university-educated mothers, proximity to highway was associated with PTB (OR 1.25, 95% CI 1.07 to 1.46) and LBW (OR 1.24, 95% CI 1.03 to 1.49), but the association was not statistically significant for SGA birth (OR 1.15, 95% CI 1.00 to 1.32). Proximity to highway was not associated with birth outcomes in other education categories. Similarly, in the wealthiest neighbourhoods, proximity to highway was associated with an elevated odds of PTB (OR 1.58, 95% CI 1.23 to 2.04), LBW (OR 1.81, 95% CI 1.36 to 2.41) and SGA birth (OR 1.32, 95% CI 1.05 to 1.66), whereas no association was observed in other neighbourhood SES categories. Therefore, neighbourhood SES modified the relation between proximity and birth outcomes more strongly than did maternal education. Furthermore, when both interaction terms were tested together in one model, the interaction between neighbourhood SES and proximity to highway remained, while that of maternal education and proximity to highway did not (results not shown).

{kind=link}
DISCUSSION
Our results indicate that distance to highway is associated with adverse birth outcomes, and that maternal and neighbourhood SES modify these relations. However, the influence of SES is opposite to that anticipated. Low SES mothers and mothers in low SES neighbourhoods were less, rather than more, likely to experience adverse birth outcomes associated with proximity to highway compared with high SES mothers and mothers in high SES neighbourhoods. These counterintuitive findings contribute in several ways to our knowledge of the relationship between traffic-related pollution and newborn health. First, our study provides empirical support for the hypothesised association between proximity to highway, a proxy for exposure to traffic-related air pollution, and adverse birth outcomes.7 Second, our results agree with other studies demonstrating effect modification of traffic-related pollution by neighbourhood SES,23 24 but reach further than previous work by demonstrating effect modification by individual-level maternal SES as well. Lastly, our results stimulate a critical examination of the underlying mechanisms linking distance to highway with newborn health.
Our data indicate that mothers residing within 200 m of a highway have a 14% increased odds of PTB and a 17% increased odds of LBW, compared with mothers who do not reside close to a highway. The sole other published study using the distance to highway measure found a 30% greater likelihood of PTB for mothers living within 500 m of a highway, accounting for maternal SES but not neighbourhood SES.7 In a supplementary analysis of the dose–response relation between distance to highway and adverse birth outcomes, we found an association using a 100 m cut-point, but no association using a 300 m cut-point, suggesting that most of the influence of traffic-related air pollution on newborn health occurs within 200 m of a highway (associations for 100 m were less precise than for 200 m, given fewer mothers residing this close to a highway).
We found that proximity to highway was associated with birth outcomes primarily for mothers living in rich neighbourhoods and for highly educated mothers. Our results are contrary to those of California-based researchers who found a stronger association between traffic exposure and adverse birth outcomes for mothers in low SES areas.23 24 These opposing findings may partly be explained by the fact that the exposure was measured differently (traffic density versus distance to highway) in each study. Our conflicting results might also reflect the different SES settings characterising Canada and the United States.28 Residents from Canada benefit from social programmes such as social security and universal health care, which may protect from the negative effects of absolute deprivation experienced by mothers living near a highway in poor neighbourhoods. In wealthy settings such as Canada, relative deprivation may be more important than absolute deprivation.36 37 Considering that residential proximity to highway is generally undesirable, mothers residing near highways in high SES neighbourhoods may perceive themselves as relatively deprived compared with affluent people in the same community, a situation that may be linked to birth outcomes.
Higher susceptibility to proximity to highway among advantaged mothers may also be interpreted in the context of competing causes.38 Low SES mothers and mothers in low SES neighbourhoods could be subject to the influence of additional risk factors for PTB, LBW and SGA birth, such as smoking or poor nutrition. These factors may be less common in high SES mothers and mothers in high SES neighbourhoods, as supported by our data, which show a steady decrease in odds of adverse birth outcomes with higher maternal and neighbourhood SES (table 1). Consequently, advantaged mothers may be more susceptible to environmental hazards because they have been protected from other hazards. These mothers may be particularly susceptible to exposure to air pollution during pregnancy, which is hypothesised to interfere directly with intrauterine growth via pollutant absorption and placental exchange, or indirectly by increasing maternal susceptibility to infection or impairing maternal respiratory function.1–4
Interestingly, our results demonstrate that SES modifies the association between proximity to highway and birth outcomes to a greater extent when SES is measured at the neighbourhood level (eg LBW: OR 1.81, 95% CI 1.36 to 2.41) rather than the individual level (OR 1.24, 95% CI 1.03 to 1.49). Neighbourhood rather than individual factors may be more important in modulating the role of proximity to highway on birth outcomes. This hypothesis is supported by our finding that only the interaction term for proximity and neighbourhood percentage low-income families remained statistically significant when tested with an interaction term for proximity and maternal education in models. Alternatively, this observation might result from different weightings of neighbourhood and maternal SES groups: about 50% of mothers were found in the highest maternal education category, while only 20% were in the most favourable neighbourhood income category. This variation yielded high SES categories that were not balanced between levels of analysis, with the broad high maternal education category possibly diluting the effect of high education at the individual level. The differences in strength of the associations cannot be explained by misclassification due to imputation of missing maternal education values because the same results were obtained after excluding imputed values.
Our results lead us to question whether distance to highway could be a proxy for something other than traffic-related air pollution exposure. If mothers living close to highways are more deprived than mothers living further away, independent of their educational status, then proximity to highway may be capturing such differences rather than air pollution itself. Underlying pathways could be related to housing market dynamics in which depressed values of dwellings near highways preferentially attract residents already at higher risk of adverse birth outcomes.17 Another possibility is that distance to highway may be measuring noise pollution, which is a chronic stressor that may influence perinatal health indirectly by altering biological function, or by affecting a mother’s affective/emotional state.39
Our study is subject to several limitations. First, the residential postal code at time of birth might not correspond to the place of residence for the whole duration of pregnancy. Second, we do not address non-residential exposure such as exposure that can occur at the workplace. Third, we could not adjust for other potential confounders, such as maternal active and passive smoking, nutritional status, domestic violence and access to prenatal care. In fact, higher rates of smoking among parents who reside near highways are possible as such parents are also more likely to be poor and to live in poor areas (Table 2), and it has been well established that smoking rates are inversely related to SES.40 Fourth, the latitudes and longitudes derived from postal codes are not as precise as coordinates based on actual street addresses. Postal codes are nevertheless valid residential address substitutes, the latter rarely being available in national registries. Canadian postal codes geocode to point locations and are spatially more restricted than American zip codes.20
Our study on newborn health is methodologically unique as it is the first to use proximity to highway, defined as living within 200 m of a highway, as a proxy for exposure to traffic-related air pollution, while accounting for individual and neighbourhood SES in a multilevel perspective. Furthermore, our study goes beyond existing published studies as it examines three birth outcomes, allowing an assessment of consistency of relations across several standard epidemiological measures of adverse birth outcomes.41 Contrary to the prevailing literature, we have found a disproportionably high association between a proxy of traffic-related pollution and birth outcomes among advantaged mothers. Neighbourhood SES contributes relatively more to this relation than does maternal education. These interesting results suggest that mechanisms linking proximity to highway and adverse birth outcomes need to be clarified.
What this study adds
Both individual and neighbourhood SES might confound and/or modify the relation between proximity to highway and adverse birth outcomes. No study has simultaneously considered proximity to highway and multilevel SES in relation to infant health.
We found that highly educated mothers and those residing in wealthy neighbourhoods were more likely than poorly educated mothers and those in more deprived neighbourhoods to experience adverse births associated with proximity to highway. These counterintuitive results suggest that mechanisms linking proximity to highway and adverse birth outcomes need to be clarified.
Acknowledgments
The authors are indebted to Nathalie Gravel, technician, who assisted with data preparation, and to the reviewers for the helpful comments and suggestions on the manuscript.
REFERENCES
Footnotes
Funding: This study was not funded. Mark Daniel is supported by a Canada Research Chair award from the Canadian Institutes of Health Research (CIHR).
Competing interests: None.
Linked Articles
- In this issue