





Abstract
Diagnosis of Mycobacterium avium complex pulmonary disease (MAC-PD) can be difficult. A previous study from Japan reported the usefulness of a serodiagnostic test for MAC-PD. The objective of this study was to evaluate the usefulness of the test in similar patients in the USA.
100 patients with known or suspected MAC-PD and 52 healthy volunteers were enrolled into the study at National Jewish Health, Denver, CO, USA. Serum glycopeptidolipid core immunoglobulin A antibody levels were measured with an enzyme immunoassay (EIA) kit and routine clinical evaluations were performed.
The patients were divided into two groups based on clinical evaluation: 87 patients with MAC-PD that met American Thoracic Society criteria, and 13 who did not meet the criteria. The sensitivity and specificity (cut-off point 0.3 U·mL−1) of the serodiagnostic test for diagnosing MAC-PD were 70.1% and 93.9%, respectively. Among the 44 patients in the MAC-PD group with two or more positive sputum cultures within the previous 6 months, sensitivity was 81.8%.
The EIA kit demonstrated good sensitivity and specificity for the identification of MAC-PD, particularly in patients with two or more positive cultures, and may be useful for rapid MAC-PD diagnosis.
Introduction
Mycobacterium avium complex (MAC) can cause chronic lung infections, varying from asymptomatic and mild to severe and debilitating. The incidence of MAC pulmonary disease (MAC-PD) in patients seronegative for HIV is reportedly increasing in many countries [1–3]. The diagnosis of MAC-PD is often complicated and time-consuming. In contrast to Mycobacterium tuberculosis, MAC has the potential to contaminate clinical specimens and one positive culture does not definitively diagnose the disease [4, 5]. The diagnosis of MAC-PD is based on a combination of clinical, radiological and bacteriological criteria advocated by the American Thoracic Society (ATS) in 2007 [6]. Some patients must undergo bronchoscopic examination to isolate MAC from a culture of a bronchial wash or, alternatively, long-term follow-up with repeated sputum examination. Therefore, new diagnostic tools for MAC-PD diagnosis are needed.
Previous Japanese studies reported the usefulness of a serodiagnostic test for MAC-PD [7–10]. The test is an enzyme immunoassay (EIA) that detects serum immunoglobulin (Ig)A antibodies directed against the glycopeptidolipid (GPL) core, a component of the mycobacterial cell wall [11, 12]. In a multicentre study of immunocompetent patients, IgA levels were significantly higher in MAC-PD patients compared to patients with other lung diseases, including pulmonary tuberculosis (TB) [10]. The test was useful for rapid diagnosis of MAC-PD and for discriminating MAC-PD from pulmonary TB. However, its applicability in clinical practice cannot be determined until its usefulness is confirmed in patients of different ethnicities and other regions. Therefore, we conducted a clinical study in the USA to investigate whether the test was useful in similar patients.
Materials and methods
Study patients and serum collection
The study was conducted at National Jewish Health, Denver, CO, USA between January and September 2009. Serum samples were collected from 100 patients with known MAC-PD who met ATS criteria or with clinically suspected MAC-PD (i.e. showing nodular bronchiectasis, or with a previous positive culture for MAC) who did not meet ATS criteria at the time of serum collection. Patients who were known to be seropositive for HIV or who were receiving treatment for MAC were excluded. After serum sample collection, routine clinical evaluations were performed. As a control, 52 workers at National Jewish Health were recruited. All were free of symptoms at that time and had no lung disease or history of lung disease. The serum samples were stored at -20°C until assayed for the IgA GPL core antibody. The National Jewish Health institutional review board approved the study protocol (HS2326), and written informed consent was obtained from all participants.
GPL core-based EIA
Serum IgA antibodies against the GPL core were measured using the EIA kit (Tauns Laboratory Inc., Shizuoka, Japan) according to the manufacturer's instructions. Briefly, 50 μL of sample diluted 1:41 with dilution buffer was added to each well of a microtitre plate coated with GPL core antigen solution and incubated for 60 min at room temperature. The plates were washed three times with buffer, after which peroxidase-conjugated mouse anti-human (IgA) monoclonal antibody was added to each well and incubated for 60 min at room temperature. Unbound labelled antibody was removed by washing. A solution of 3,3′,5,5′-tetramethylbenzidine (100 μL) was added to each well and the plates were incubated for a further 20 min at room temperature. After stopping the enzymatic reaction, absorbance at 450 nm was measured with a microplate reader (Model 680; Bio-Rad Laboratories Inc., Hercules, CA, USA). Reactions were performed in duplicate. Results are given as arbitrary U·mL−1 in relation to the standard curve generated using reference sera. Technicians without prior knowledge of the clinical data performed the assay.
Chest computed tomography
The correlation between the extent of disease on chest computed tomography (CT) and antibody levels was investigated. To assess the extent of disease, we divided the lung into 18 segments on a conventional chest CT, according to the anatomical segments, as in previous studies [9, 10]. The extent of disease was expressed as the number of involved CT segments in which MAC lesions were present.
Statistical analysis
All statistical analyses were performed using GraphPad Prism Version 4 (GraphPad software, Inc., San Diego, CA, USA) or JMP Version 8.0 (SAS Institute Inc., Cary, NC, USA). Continuous variables are reported as mean±sd. Patient groups were compared using the Kruskal–Wallis test and Dunn's multiple comparison test as a post hoc analysis for continuous variables and Chi-squared test or Fisher's exact test for categorical variables. A receiver operating characteristic (ROC) curve was used to determine cut-off points to differentiate between MAC and non-MAC disease (patients who did not meet the criteria and healthy volunteers). Spearman's correlation coefficient by rank was used to determine the relationship between antibody levels and extent of disease on chest CT. Probability values (p)<0.05 were regarded as significant.
Results
Study subjects
In total, 152 participants were enrolled into this study; their baseline characteristics are shown in table 1. Most participants were Caucasian. Out of 100 patients with known or suspected MAC-PD, 87 met the ATS criteria, based on routine clinical evaluation at serum collection, and were classified in the MAC-PD group. Out of these 87 patients, 64 had at least one positive culture for MAC within 6 months and 44 patients had at least two positive sputum cultures within 6 months of serum collection. 13 patients did not meet the criteria, and were classified as the not MAC-PD group. All patients in the not MAC-PD group had respiratory symptoms, such as cough and sputum production (n = 6), and dyspnoea (n = 3), and all met ATS radiology criteria. Among them, three had never had positive MAC cultures. Two of these patients were diagnosed with bronchiectasis and one had a few small nodules without bronchiectasis on chest CT examination. The remaining 10 patients in this group had one previous culture positive for MAC and demonstrated multiple nodules with bronchiectasis, but did not meet ATS bacteriological criteria. Seven had cultures positive with other bacteria, including Pseudomonas aeruginosa, Haemophilus influenzae, Staphylococcus aureus, Klebsiella pneumoniae, Mycobacterium terrae, Mycobacterium gordonae and Mycobacterium kansasii. Most patients in the not MAC-PD group were thought to have had MAC-contaminated sputum cultures and bronchiectasis along with another bacterial infection, or they may have presented with low-grade or early-stage MAC infection. Healthy volunteers were younger (p<0.0001) and had a higher body mass index (p = 0.004) than the other groups. We observed a higher rate of prior therapy (p = 0.0008) and a higher rate of Mycobacterium intracellulare infection in the MAC-PD group (p = 0.005) than in the not MAC-PD group. 22 patients used immunosuppressive agents, including oral prednisone (n = 11), inhaled steroid (n = 10) or a combination of both (n = 1). No significant differences in laboratory data, including white cell count, C-reactive protein, albumin, IgG, IgA and IgM, were observed between the two groups.
Level of antibody to GPL core
The level of IgA antibody against the GPL core was 2.46±3.47 U·mL−1 in the MAC-PD group, 1.11±3.68 U·mL−1 in the not MAC-PD group, and 0.22±1.11 U·mL−1 in healthy volunteers. As shown in figure 1, antibody levels were significantly higher in the MAC-PD group than in the not MAC-PD group (p<0.01) and healthy volunteers (p<0.001). Three healthy volunteers and one patient in the not MAC-PD group, who was culture-positive for MAC with nodular bronchiectasis but did not meet the ATS criteria [6], had high levels of GPL antibody. The sensitivities and specificities under various cut-off points are shown in table 2. ROC analysis determined a best cut-off point of 0.3 U·mL−1 (fig. 2). The sensitivity and specificity of the test for diagnosing MAC-PD were 70.1% and 93.9%, respectively. The exact numbers of patients with MAC-PD, with not MAC-PD and healthy volunteers who had positive and negative test results under a cut-off point of 0.3 U·mL−1 are shown in table 3. Limiting the analysis to the 64 patients with MAC-PD who had at least one positive culture for MAC within 6 months or the 44 patients with MAC-PD who had two or more positive sputum cultures within 6 months, the sensitivities were 75.0% and 81.8%, respectively. We observed significantly higher antibody levels for M. intracellulare (3.08±3.52 U·mL−1) than for M. avium (1.42±1.77 U·mL−1) as causative agents in MAC-PD (p = 0.030).
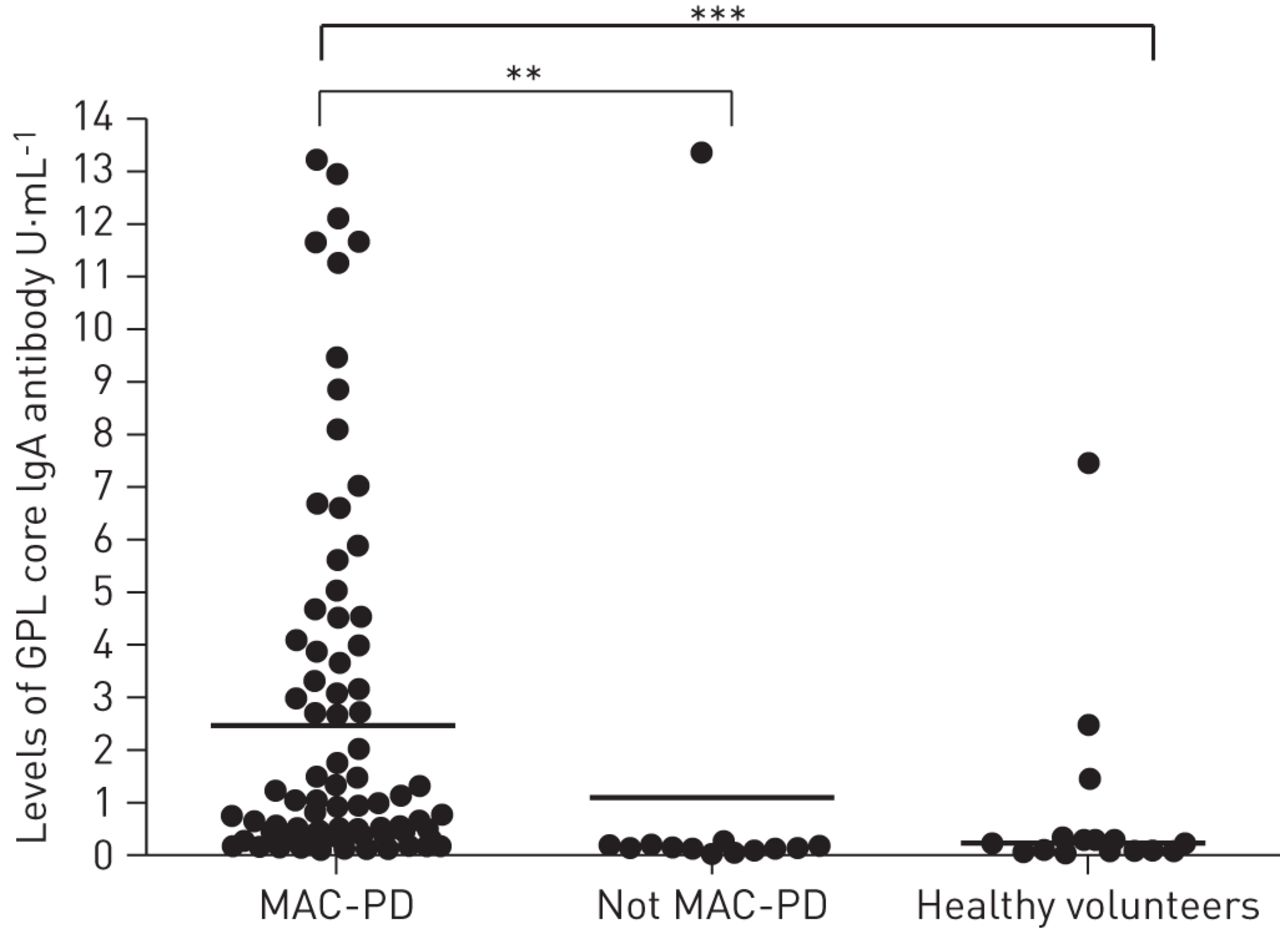
Levels of immunoglobulin (Ig)A antibody against glycopeptidolipid (GPL) core antigen. The Mycobacterium avium complex pulmonary disease (MAC-PD) group consisted of 87 patients who met American Thoracic Society (ATS) criteria and the not MAC-PD group consisted of 13 patients who did not meet ATS criteria. Antibody levels were significantly higher in the MAC-PD group than in the not MAC-PD group (p<0.01) or in healthy volunteers (p<0.001). All results are expressed as individual data points, and horizontal bars indicate geometric means. **: p<0.01; ***: p<0.001.

{kind=link}
{kind=link}
Receiver operating characteristic curve constructed between the Mycobacterium avium complex pulmonary disease (MAC-PD) group (n = 87) and non-MAC disease group (not MAC-PD and healthy volunteers, n = 65). Arrows indicate cut-off points.
Radiographic severity and the level of GPL core antibody
86 patients with MAC-PD underwent concurrent chest CT and serodiagnosis. The extent of disease on CT and antibody levels was correlated (r = 0.24, p = 0.0309). Nine patients presented with cavitary lesions. No significant differences were observed between patients with and without cavitary lesions (3.83±5.25 versus 2.32±3.24 U·mL−1; p = 0.597).
Discussion
This is the first report on the utility of serological testing for GPL core IgA antibody in the diagnosis of MAC-PD in the USA. The testing provided 70.1% sensitivity and 93.9% specificity with a cut-off point at 0.3 U·mL−1 for diagnosing MAC-PD. When limited only to patients with MAC-PD who had two or more recent positive cultures, the sensitivity was 81.8%, indicating that the test may be useful for rapid diagnosis of MAC-PD.
Serological responses to some MAC antigens were investigated in the 1980s and 1990s [13–15]. Elevated levels of IgG or IgM antibody to GPL or crude protein antigen in patients with MAC disease have been reported, but the sample sizes of these studies were relatively small. More recently, clinical investigations of MAC serodiagnosis using the GPL antigen have been reported in Japan [7, 8, 10, 16, 17]. Our previous studies showed that the antibody to the GPL core was elevated in patients with MAC-PD compared with patients with pulmonary TB, other lung diseases and healthy controls [7, 8, 10]. In our previous study, the best sensitivity and specificity were obtained in the measurement of IgA antibody [8]. In a multicentre study, the sensitivity and specificity of the test in 70 patients with MAC-PD, 18 with MAC contamination, 36 with pulmonary TB, 45 with other lung disease and 76 healthy subjects were 84.3% and 100%, respectively, using the cut-off point of 0.7 U·mL−1 set by ROC analysis [10]. Fujita et al. [16] investigated the IgG responses to the GPL core antigen and various lipid antigens in 64 patients with MAC-PD and 105 patients with pulmonary TB. Positive test results were found in 88.4% of MAC patients [16]. Nishimura et al. [17] also investigated IgG responses to apolar GPL in 65 patients with MAC-PD, 15 with suspected MAC-PD, 25 with pulmonary TB, 10 with M. kansasii pulmonary disease and 100 healthy controls. The sensitivity and specificity for diagnosis of MAC-PD were 88.4% and 81.7%, respectively [17]. Although the serological test demonstrated relatively good sensitivity and specificity, all these studies were conducted only in Japan and almost all participants were Asian. The present study is the first to evaluate the serological test in similar patients of different ethnicities and in a different region.
MAC is generally an indolent infection and the lack of human to human transmission has made identification of rapid and alternative diagnostic methodologies a relatively low priority. However, establishing a definitive diagnosis of MAC-PD can be difficult and time consuming and isolation of MAC does not necessitate the initiation of therapy, which is a decision based on an individualised risk–benefit analysis [6]. Therefore, rapid nonculture-based diagnostics would be helpful in distinguishing MAC-PD from other lung diseases, particularly when sputum specimens are difficult to obtain. Bronchoscopy is usually applied because of the need to rule out pulmonary TB or other infections that mimic MAC infection. In these cases, a seropositive result can reveal MAC growth because of the high specificity of the test, allowing patients to avoid invasive and expensive procedures. This approach may be especially useful in elderly patients who have multiple complications or in patients who are reluctant to undergo such an invasive procedure for very mild signs and symptoms. It is also useful for patients whose cultures revealed MAC at one time but who otherwise do not meet current diagnostic criteria [6]. A seropositive result confirms positive culture results, reassuring patients that the diagnosis is not merely the result of culture contamination. Conversely, seronegative results may indicate contamination rather than disease when the patient has no signs or symptoms of MAC infection. It is especially useful for patients who have underlying lung diseases from which it is difficult to distinguish MAC disease by chest radiography. It is not yet known whether antibody levels can be used to facilitate decision-making regarding initiation of treatment or for predicting treatment outcome or prognosis. The utility of the test for extrapulmonary disease has not been evaluated. Further studies are needed to address these issues.
A cut-off point of 0.3 U·mL−1 provided the best combination of sensitivity and specificity in this study. Previous studies in Japan reported that a cut-off point of 0.7 U·mL−1 was associated with a sensitivity of 84.3% [10]; however, 0.7 U·mL−1 was associated with a much lower sensitivity (51.7%) in the current study. There are several explanations for this. First, none of the study patients were taking antimycobacterial therapy at the time of serum collection, which yielded a more stable group status than was available in the previous study. In general, initiation of therapy is thought to control symptoms and prevent progression when patients have active MAC disease. Indeed, 23 patients (26.4%) had no positive culture for MAC within 6 months of serum collection, whereas all patients had a positive culture at the time of serum collection in the previous study [10]. Secondly, differences in race may affect the result, although the likelihood of this is not clear. In this study, most patients with MAC-PD were Caucasian (98.9%), whereas all patients in the previous study were Asian [10]. A third explanation may be the differences between MAC species. M. intracellulare was the dominant causative agent in this study (44.8%), whereas M. avium was dominant in the previous study (80.0%; p<0.001). The GPL core antigen that was used in the EIA kit was derived from M. avium serotype 4 [8]. However, the possibility of species specificity is unlikely because the GPL core is a common component in M. avium and M. intracellulare [11]. Interestingly, the antibody levels in patients infected with M. intracellulare were higher than those in patients with M. avium in this study (p = 0.005).
False-positive EIA test results most likely result from three major causes: 1) cross-reactivity to other antigens, 2) asymptomatic MAC infection (not disease) and 3) the sensitivity of the current ATS diagnostic criteria. Rapidly growing mycobacteria, such as Mycobacterium chelonae, Mycobacterium fortuitum and Mycobacterium abscessus, possess GPL on their cell wall and, thus, could induce production of antibodies to the GPL core [11]. Particular attention should be paid to M. abscessus, which has become an important pathogen in chronic lung infection because its radiographic findings are similar to those of nodular bronchiectatic MAC-PD [18, 19]. In our experience with small samples, some patients with M. abscessus or M. fortuitum had high levels of antibody against the GPL core (data not shown). In the present study, four patients with MAC disease and one patient with not MAC disease had co-infection of M. abscessus. However, the level of antibody was low (0.03 U·mL−1) in the one patient with not MAC disease. The second cause is asymptomatic MAC infection. According to a survey using the purified protein derivative (PPD)-B skin test, sensitisation to M. intracellulare is common in the USA, with about one in six persons in 1999–2000 demonstrating skin test positivity [20]. The clinical significance is unknown, but in the absence of adequate knowledge regarding the variability of the antibody response, one could speculate that some people with sensitisation (but not MAC-PD) have elevated IgA to GPL. Further, it may be reasonable to assume that a significant proportion of people with MAC “infection” are asymptomatic, but have an elevated IgA to GPL. In this study, three healthy volunteers also demonstrated a high response to MAC antigen. Two of these volunteers reported lifestyle habits, such as frequent hot tub use, indoor swimming pool use or gardening, in which possible exposure to MAC could have occurred, suggesting that they may have asymptomatic infection. Further studies in which the serological test is performed in much larger groups of healthy individuals may be necessary to investigate the relationship between asymptomatic infection and serological test results. The final cause is the sensitivity of the current ATS diagnostic criteria [6]. In this study, one patient in the not MAC disease group demonstrated a high serological response to MAC GPL antigen. In this case, she had a single positive culture for MAC and typical nodular bronchiectatic findings on chest CT, but she did not undergo bronchoscopy and repeated sputum cultures did not grow MAC again; thus, she failed to meet the criteria. Given the high levels of antibody to MAC antigen and the characteristic radiographic findings, she may have true MAC disease and it is possible that further investigations will yield results that satisfy the criteria.
A weak positive correlation between the extent of MAC-PD on chest CT and antibody levels was observed (r = 0.24, p = 0.0309), as reported in previous studies [9, 10]. This observation may indicate that the antibody levels reflect MAC disease activity. However, the extent of disease as defined by number of involved lobes on CT may not precisely reflect MAC-PD severity. Further investigation may be needed to compare the serological test and radiographic findings using standardised descriptions of radiographic severity.
In summary, the EIA test demonstrated good sensitivity and specificity for the identification of MAC-PD in the USA, particularly in patients with two or more positive cultures. The serological test can be performed repeatedly and adds useful information with minimal risk, which would help physicians to manage patients with suspected MAC-PD.
Footnotes
Conflict of interest: Disclosures can be found alongside the online version of this article at www.erj.ersjournals.com
- Received June 22, 2012.
- Accepted September 26, 2012.
- ©ERS 2013
References










