





Abstract
The aim of the present study was to perform cost-minimisation analysis of contact investigation from a public health perspective using the tuberculin skin test (TST) and a new blood assay, QuantiFERON-TB Gold (QFT-G).
A decision-analysis model simulated the costs of investigating a cohort of adult close tuberculosis contacts by the public health service following the current German guidelines over a period of 2 yrs. The economic outcomes were compared with alternative screening strategies. These were: 1) QFT-G instead of TST; 2) TST followed by QFT-G; and 3) TST followed by QFT-G in vaccinated (bacille Calmette–Guérin (BCG)) subjects.
In a base-case analysis, the costs of TST-based screening were 91.06 Euros (EUR)·contact-1, assuming a 1% tuberculosis-case-finding incidence. The least expensive strategy was TST screening plus subsequent QFT-G testing (52.05 EUR), resulting in a 43% cost reduction. Using QFT-G alone in BCG-vaccinated subjects who tested positive in the TST led to a 39% cost reduction. The savings using QFT-G alone instead of TST amounted to 29.77 EUR·contact-1. The results depended on the acquisition costs assumed and the proportion of positive results in TST-based screening.
Screening for tuberculosis by combining tuberculin skin testing and QuantiFERON-TB Gold markedly reduces public health costs compared with tuberculin skin test screening alone.
Although routine contact investigation of infectious tuberculosis (TB) cases is a key component of TB-control programmes in most countries, only a few studies have addressed the costs to the public health agencies that usually perform this most important task 1, 2, and which are financed by the local municipalities through tax revenues.
Contact investigation is based on the established fact that individuals recently infected with Mycobacterium tuberculosis are at greatest risk of developing the disease shortly after becoming infected. The lifetime risk of TB reactivation largely depends upon the age of the infected person and the size of the induration produced by a tuberculin skin test (TST), varying between 8, 10 and 13%, respectively, among adults aged 16–25 yrs separated into three categories of skin-test reaction (induration of ≥5, ≥10 and ≥15 mm diameter); the corresponding risks are 4, 5 and 7% among adults aged 35–45 yrs 3. However, an estimated 50% of the latent TB infection (LTBI) cases that will ever develop active disease do so within the first 2 yrs following infection 4.
There are two courses that the public health service can take if the TST result in a contact person is positive. These are complementary and serve the goal of preventing the spread of disease to the general public, thus breaking the chain of infection.
The first is to offer isoniazid (INH) chemoprevention to contact persons suspected of having LTBI. The second approach, for contact persons who do not or cannot accept the offer of treatment, entails screening for active TB disease through a series of subsequent radiographic examinations that cover the 2-yr observation period. In different countries, the national recommendations focus on different points. Although the recently published US recommendations of the Centers for Disease Control and Prevention (CDC) 5 emphasise chemoprevention and only provide for an initial chest radiograph in order to exclude active pulmonary TB infection, the UK recommendations 6 call for follow-up radiographic examinations 3 and 12 months after the initial examination of contact persons who decline chemoprevention. In such cases, the German recommendations call for radiographic follow-up after 3, 9 and even 15 months (fig. 1⇓) 7.
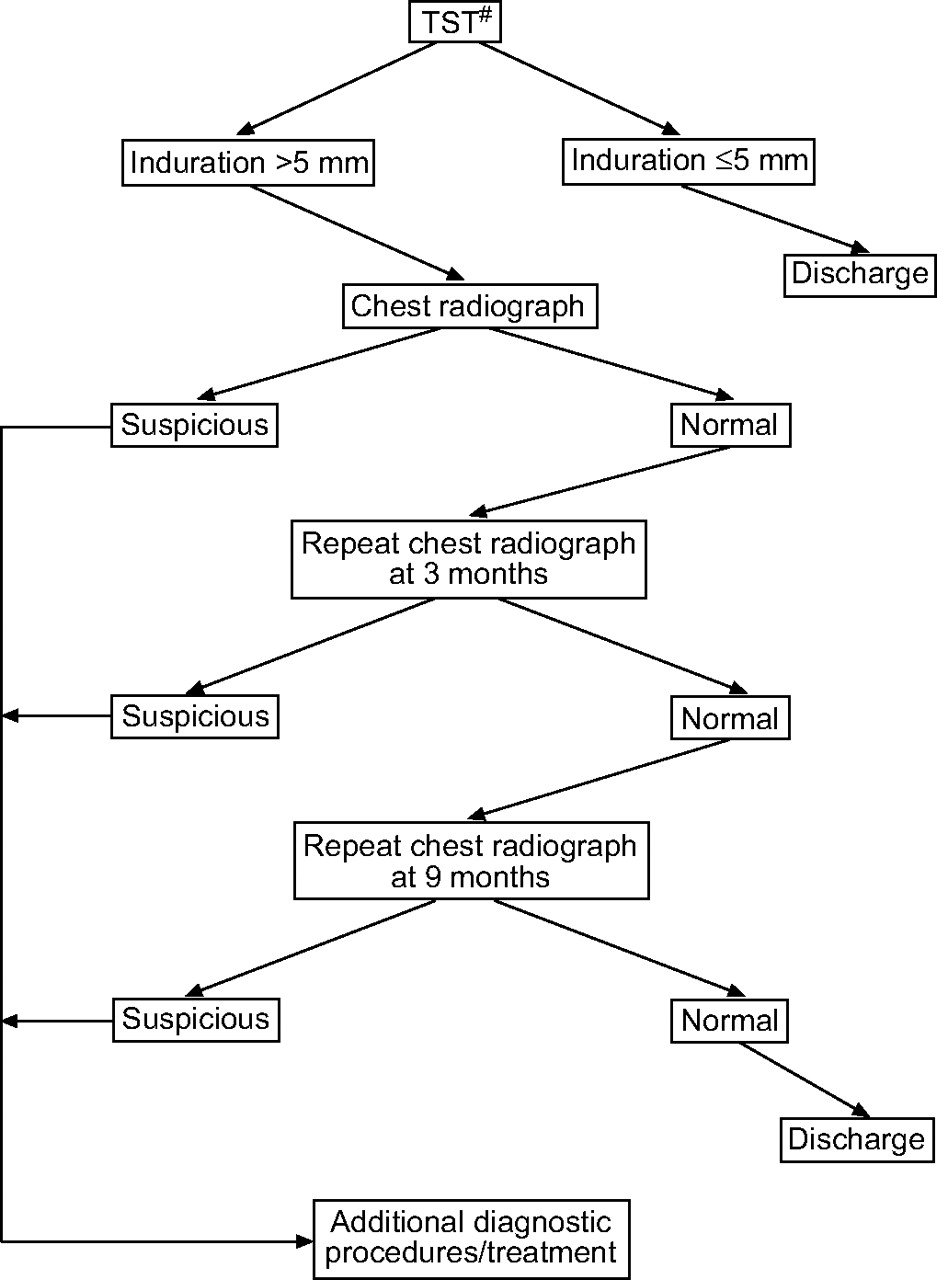
Flow chart showing the examination of close contacts of infectious tuberculosis cases in Germany. TST: tuberculin skin test. #: purified protein derivative of tuberculin RT 23 (2 TU·0.1 mL-1) from the Danish Statens Serum Institute.
Administration of INH (300 mg for 9 months recommended in Germany 8) to recent converters by practicing pneumologists who follow these patients has been clearly proven to be cost-effective 9. The costs of medication and observation by the physician until the end of the preventative therapy, however, are paid by the German statutory health insurance organisations called public Krankenkassen [medical insurance], and, therefore, lie beyond the economic scope of public health service and the present study. Of concern, however, to the public health service is the eventual neglect of its other obligatory and legal duties in connection with TB. The active seeking out and care of persons at risk of TB disease (particularly the homeless) compete with contact tracing activities for scarce resources. It is, therefore, imperative that contact investigation be carried out as efficiently as possible.
As an alternative to the TST for LTBI screening, M. tuberculosis-specific interferon gamma (IFN-γ) assays have recently become available. These claim not only a higher specificity regarding the degree of exposure of contacts to the source case but also the absence of or limited cross-reactivity in those vaccinated with M. bovis (bacille Calmette–Guérin (BCG)) or infected by nontuberculous mycobacteria (NTM) 10–14. One important aspect of the differences between the TST and IFN-γ tests is that their different results lead to different numbers of subsequent contact investigation procedures (radiographic or INH-chemoprevention).
Against the background of increasingly limited resources, an attempt was made to assess the costs of screening contacts for M. tuberculosis infection (including repeated chest radiographs for surveillance) and to conduct a cost-minimisation analysis within the framework of the German public health system, taking as an example the city of Hamburg, Germany. Hamburg is one of the German federal states, and, with 1.73 million residents, the second largest city in Germany; in 2004, it had the highest TB incidence (12.0 cases per 100,000 population) of all of the federal states.
In the absence of a gold standard reference test for LTBI, it is impossible to compare directly the accuracy (sensitivity and specificity) of the two assays, the effects of BCG vaccination on each test, and, therefore, the relative medical benefit of each testing strategy. Others have addressed these questions in different groups 13, 14. Therefore, in contrast to Markov modelling, the decision-tree analysis used ignores the dynamics of progression to disease by following a cohort for decades. It only takes into account the costs that would immediately be incurred upon following the screening steps
The cost-minimisation analysis, applied when the consequences of the alternatives are deemed to be equal, is a special type of cost-effectiveness analysis that aims to achieve a given goal of prevention at a lower cost. Unlike the dynamic development of a TB illness over the entire lifetime of a single M. tuberculosis-infected individual in western industrial countries, the percentage of contact individuals who fall ill within the short period of 2 yrs following detection of a particular TB case has, independent of the year studied and population observed, proven to be relatively stable at 1–2% in a large cohort of contact persons 15–18.
In this context, the more cost-effective intervention is defined in terms of testing cost alone. In doing this, an attempt was made to follow the current German guidelines and also to take into account new options as proposed in the national recommendations of other western countries.
METHODS
Screening strategies and input of relative probabilities
Recent CDC recommendations 5 suggest that the whole-blood IFN-γ test QuantiFERON-TB Gold (QFT-G; Cellestis International, Carnegie, Victoria, Australia) can be used in contact investigations to replace, rather than to supplement, the TST, and that the results of the QFT-G should prompt the same evaluation and management as those of the TST. However, because of the greater correlation of QFT-G with exposure, and enhanced specificity over the TST, it may be a reasonable option to use this test as a confirmatory test in those who are TST-positive and thereby minimise the number of subjects evaluated for active TB (i.e. using chest radiography and possibly treated for LTBI). This procedure is currently suggested in the Swiss recommendations 19 and the draft National Institute for Health and Clinical Excellence guidelines for the National Health Service in England and Wales [20]. Such a procedure may be additionally beneficial when screening BCG-vaccinated contacts in routine contact investigation, in which false-positive TST responses would be more commonly expected 12. In addition, the QFT-G excludes false-positive TST results due to not only BCG, but also boosting (if repeated for any reason) and NTM 13, 14.
Recently, in a prospective real-world comparison study regarding routine contact investigation of close contacts involving a high proportion of BCG-vaccinated persons, the results from 309 contacts (aged 28.5±10.5 yrs) of 17 index cases simultaneously tested using both the QFT-G and TST in the period between May 1, 2005 and October 31, 2005 were assessed (table 1⇓). Of these contacts, 157 (50.8%) had received BCG vaccination and 84 (27.2%) had migrated to Germany from a total of 25 different countries. For the TST, the positive response rate was 44.3% (137 of 309), whereas only 31 (10%) gave a positive QFT-G result. These results are consistent with those of two recent contact tracing studies in which TST results were strongly associated with prior BCG vaccination and >80% of the TST-positive BCG-vaccinated contacts did not respond to 6-kDa early secretory antigenic target in IFN-γ enzyme-linked immunospot tests 21, 22.
Results of tuberculin skin test(TST) and QuantiFERON-TB Gold (QFT-G) in a population of 309 close contacts stratified by bacille Calmette–Guérin (BCG) vaccination
Close contacts were defined as household and intimate contacts (and also comprised employees who showed demonstrable continuous exposure to the source case, or pupils sharing the same classroom) whose aggregate exposure time was ≥40 h within the period of infectiousness 18. TST results were considered positive if the induration was >5 mm in diameter, according to the current German guidelines 7, which, in line with the CDC guidelines, disregard BCG vaccination status in order to provide maximum sensitivity.
Using the frequencies of test results and other parameters obtained from this prior study on 309 contacts, it was possible to compare the expected costs (in Euros (EUR)) of four optional strategies within the context of a contact investigation programme. The strategies compared were as follows: 1) TST, 2) QFT-G alone, 3) TST followed by QFT-G for contact persons with a positive TST result, and 4) TST followed by QFT-G only for previously BCG-vaccinated contacts with a positive TST.
Decision-analysis model
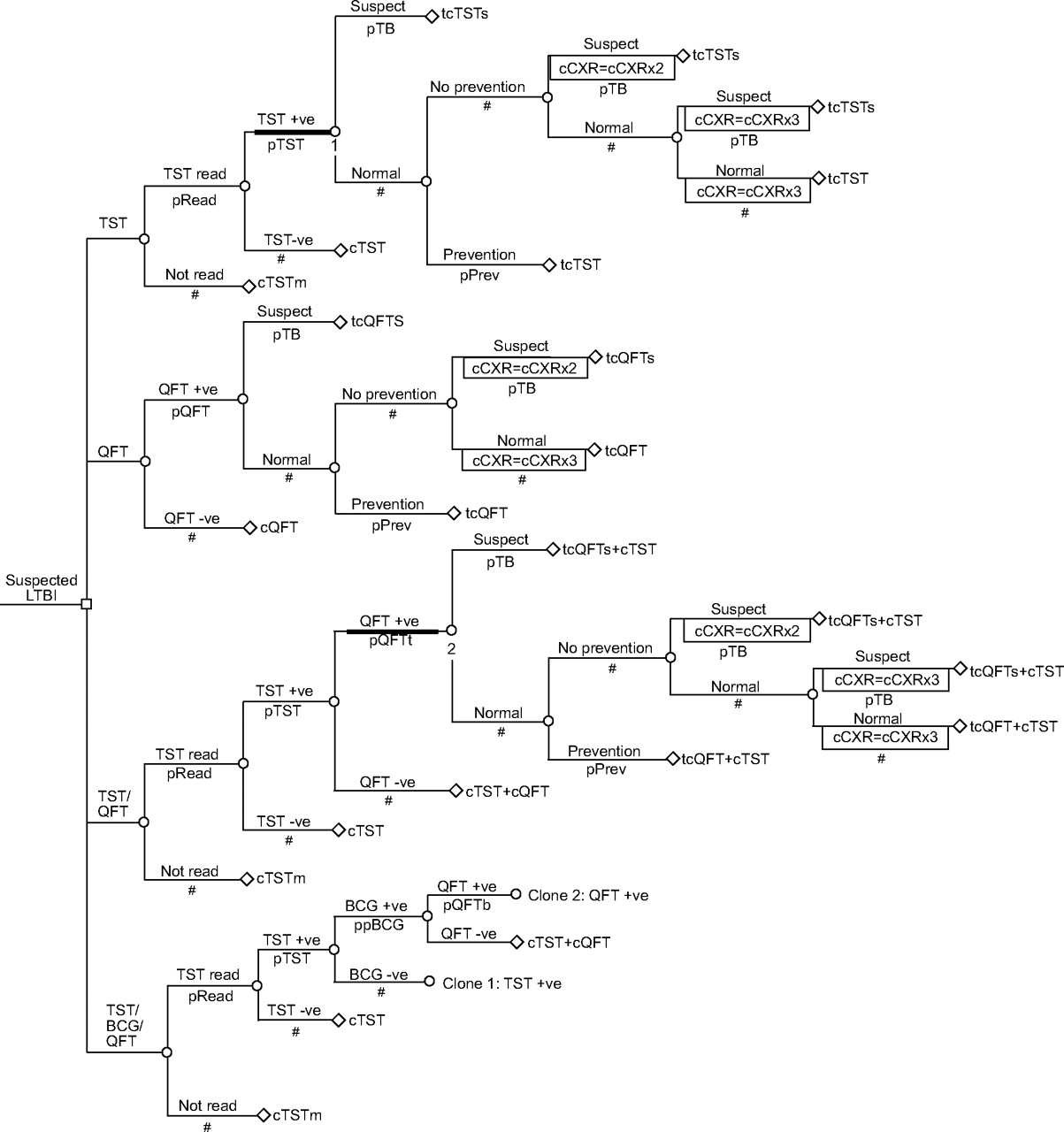
In order to perform the cost-minimisation analysis, a decision-tree model was developed to trace the economic outcomes for a hypothetical cohort of 1,000 adult close contacts of patients with sputum-smear-positive pulmonary TB (fig. 2⇓). The whole cohort begins at time zero in the contact state, entering the tree from the left. The model is evaluated by attaching probabilities to each branch of the tree, and rewards (component costs, which are used to calculate total cost for each scenario) to the terminal nodes on the right. The calculation of costs includes not only the first chest radiograph but also the two subsequent radiographic examinations. Decision-analytical calculations were performed using TreeAge Pro Healthcare Module 2005 (TreeAge Software Inc., Williamstown, MA, USA).

{kind=link}
{kind=link}
Decision-analysis model for predicting the costs of four alternative tuberculosis (TB) screening strategies in a cohort of adult close contacts. A decision node (□) represents the decision to test a contact using the tuberculin skin test (TST) or QuantiFERON-TB Gold (QFT). Branches from a change node (○) represent the possible outcomes of an event; terminal nodes (⋄) are assigned the cost of a prior series of actions and events. The bold horizontal lines indicate that the following subtree is cloned, i.e. a copy is attached to a node in another decision tree. The cloned subtrees, denoted 1 and 2, are attached to nodes in the TST/bacille Calmette–Guérin (BCG)/QFT decision tree. Probabilities (p) are as follows. pRead: probability of TST being read; pTB: probability of an infected contact developing active disease; ppBCG: probability of a TST-positive contact having received BCG vaccination; pQFT: probability of QFT-G result being positive; pQFTb: probability of QFT-G result being positive in BCG-vaccinees; pQFTt: probability of QFT-G result being positive in TST-positive contacts; pTST: probability of TST result being positive; pPrev: probability of a contact receiving isoniazid chemoprevention. Further explanations of definitions are given in table 2⇓. LTBI: latent TB infection; +ve: positive; -ve: negative; cTST: cost of TST; cTSTm: cost of unread TST; tcTST: total cost of TST; tcTSTs: total cost of TST-based screening per contact suspected of having TB disease; cCXR: cost of chest radiography; cQFT: cost of QFT-G; tc QFT: total cost of QFT-G; tcQFTs: total cost of QFT-G-based screening per contact suspected of having TB disease. #: complementary probability (all chance node branches probabilities sum to 1.0).
As stated above, the following four possible testing strategies were compared.
Tuberculin skin test
It was assumed that a TST was administered to the entire cohort, but that there was a small proportion of contacts (4.8% of all contacts tested in the Central Hamburg Public Health Department (Hamburg, Germany) in 2004; see below) who would not return to have the result read (1–pRead). All other contacts represent the final fraction with a TST result. For simplicity, it was assumed that no patient required a second test. No further action was taken with contacts showing negative TST results. Contacts exhibiting a positive skin reaction (pTST) were requested to undergo chest radiographic examination. Once active TB was excluded, these people were assumed to be cases of LTBI and may have been offered INH-chemoprevention (pPrev). Those who did not receive INH (1–pPrev) were further examined by undergoing a second and third chest radiographic examination at the aforementioned time intervals. The contact investigation ended at this point if radiographic examinations did not indicate pulmonary TB. Any contact suspected of having pulmonary TB was referred for further diagnosis to an outpatient pulmonologist or chest clinic (pTB).
QuantiFERON-TB Gold
By completely replacing the TST with QFT-G, the sequence of screening steps was identical to the TST scenario, except that it was assumed that no contact person was lost to follow-up (i.e. by failing to return to the local public health office to have the result of the test read). It was assumed that a positive QFT-G result would reflect the same immunological reactivity as the TST, i.e. that an infected person would have a positive test result 8−10 weeks following infection with M. tuberculosis. This is stated in recent CDC recommendations for the use of QFT-G 23, but, to the present authors’ knowledge, no systematic studies have been conducted that have directly compared the two tests with regard to this point.
QuantiFERON-TB Gold for TST-positive contacts
All contact individuals were given a TST, followed by a QFT-G only for those who were TST-positive. It was presupposed that blood would be collected into QFT-G tubes immediately after reading the TST; therefore, a third visit by the contact person was not necessary.
QuantiFERON-TB Gold only for those who are TST-positive and have been BCG-vaccinated
Here, it was assumed that the BCG-vaccinated contacts had already been identified during the first survey before any test, which is the same for all contact individuals, and, consequently, incurs no additional costs.
Discounting
Discounting reflects the higher value of money spent now as opposed to in the future. Owing to the short time-span of the contact screenings, costs and outcomes (number of active TB cases detected) were not discounted.
Sensitivity analysis
In order to identify the threshold at which changes in probability estimates and cost values cause changes in the ranking of the screening strategies assessed in the base-case analysis, univariate sensitivity analyses were conducted wherever appropriate. Therefore, except where otherwise stated, costs were halved and doubled to obtain lower and upper limits, respectively. Multivariate sensitivity analyses were performed on the costs for TST and QFT-G testing.
Costs
All costs are reported in 2004 Euros (except the 2005 costs for QFT-G and purified protein derivative of tuberculin (PPD) RT 23, from the Danish Statens Serum Institute) and presented in table 2⇓.
Base-case estimates and ranges used in cost-minimisation analysis
Personnel and material costs of the public health service
At the central location for combating TB in Hamburg, where all radiographic examinations are performed, the Central Hamburg Public Health Department employed 3.5 medical technical assistants in 2004, with resultant total salary costs of 197,280 EUR (2.5 BAT VIb positions plus 1 BAT Vb position), including additional administrative costs of 15% and a lump office workplace fee. On the basis of a mean of 211 workdays·yr-1 and a workday of 7.7 h (462 min), the resulting personnel expenses for one medical technical assistant were 0.58 EUR·min-1.
The tasks of medical technical assistants employed there are limited to TB screening, i.e. radiographic examinations and the performance of all of the tuberculin tests performed for contact investigations. Besides the actual radiographic procedure, the radiographic examination also involves personnel organising an appointment for TST-positive contacts to attend the examination. Upon failing to reply, these contact individuals again receive up to two further summonses, and, if necessary, are informed by telephone either personally or by their lodging providers (e.g. shelters for the homeless and other residences). Moreover, this work involves maintaining a registration site during office hours, explaining the examination procedure and filling in radiographic certificate cards.
The personnel costs for the radiographic examination were calculated as follows. The necessary time costs were multiplied by the number of tuberculin tests performed in 2004, i.e. 2,668 TSTs. A mean time cost of 7 min was measured for the preparation and performance of the test. This results in personnel costs of 4.06 EUR·contact-1 (cAdmin), i.e. 10,832.08 EUR for the 2,668 TSTs.
The remaining personnel costs can be attributed solely to radiographic examinations and their associated organisational as well as documentary cost, as described above (the sum of it here denoted “radiographic procedure”), which amounts to a total of 197,280–10,832.08 or 186,447.92 EUR. In 2004, 3,276 radiographic examinations were conducted. This amounts to personnel expenses of 56.91 EUR per radiographic procedure. Additional to these costs are the costs for the evaluation of the radiographic images by a specialist, which amounts to personnel costs of 0.96 EUR·min-1. Such a physician needs 3 min to assess one image, resulting in personnel expenses of 2.89 EUR.
Further material costs are incurred for the radiographic examination by using a digital radiography apparatus. These costs comprise material and operating expenses, assuming a linear depreciation of the instrument over a period of 10 yrs. The acquisition costs of the Philips Diagnost CS 2 applied radiographic system with the PCR AC 500 storage foil system and Micora Store observation station (Philips Medizin Systeme, Hamburg, Germany) amount to 205,809.95 EUR including value added tax (VAT), i.e. 20,581 EUR·yr-1 with average annual repair expenses, quality control tests and material costs of 4,834.71 EUR, as well as maintenance costs of 22,070.60 EUR. Dividing this by the number of examinations, each radiographic procedure creates material expenses of 14.50 EUR (47,486.31/3,276). Consequently, the costs for the performance of a radiographic examination within the scope of a contact investigation (sum of the personnel costs for medical technical assistants and physician plus material costs) amount to a total of 74.30 EUR including administrative expenses (cCXR).
At the end of screening tests yielding positive TST or QFT-G results, a medical consultation is necessary for the contact person to choose between chemoprevention and another radiographic screening within the next 2 yrs. This also includes the detection of disease symptoms that manifest between the radiographic appointments or thereafter and the precautionary measures to be taken as a result thereof. If the contact chooses to undergo chemoprevention, this consultation also includes an explanation of the treatment, and the doctor then refers the contact to a further pneumologist who has to be informed of the finding. This takes a mean time of 25 min, which incurs doctor’s expenses of 24 EUR (25×0.96; cCons). A radiographic finding of suspected TB, moreover, requires a further corresponding report, and an immediate organisation of more detailed diagnostics by a pneumologist/lung clinic. This takes a mean of 40 min, thereby leading to costs of 38.40 EUR (cSusp).
The reading of the TST is performed by a doctor. By including documentation and a brief consultation (e.g. about additional measures to be taken upon strong reaction, etc.), a mean time cost of 8 min was found, with corresponding personnel expenses of 7.68 EUR (8×0.96; cRead). In the year 2004, 2,540 of 2,668 TSTs performed were read (pRead = 0.952).
Material costs of the TST
The TST licensed for Germany is PPD RT 23, 2 TU·0.1 mL-1, from the Danish Statens Serum Institute, and distributed by Pharmore. The delivered price for 10 glass vials, each containing 1.5 mL RT 23 is 149.99 EUR, including 16.5% VAT. Since droplets always remain in the cannula and the vial, only 10 test doses of 2 TU are withdrawn from the 1.5-mL vials 24. According to the manufacturer’s specifications, opened vials can be used only up to a maximum of 24 h after the withdrawal of the first dose. Whether only one or the maximum of 10 test doses per vial are used depends on the number of contact individuals tested per day. Consequently, the material costs per TST range 1.5–15 EUR. The mean dose amount of five test doses, with costs of 7.5 EUR per contact individual, is assumed as the base-case value in the present analysis (cRT23).
Material and personnel costs of QuantiFERON-TB Gold
The current charge made by a local private laboratory (Labor A. von Froreich, C. Schmidt & Partner) in Hamburg (as per March 1, 2005) is 40 EUR per contact individual, a price that includes the tubes for blood collection, IFN-γ ELISA materials, labour and sample transport to the laboratory via a collection service (cLab). The time required for blood sampling is calculated to be equal to that needed for performing the TST (cAdm); nevertheless, this excludes the time for reading the TST. Material costs (syringes, cotton swabs, disinfection spray and bandages) are included, as for application of the TST, in the fee for labour costs.
Compliance with isoniazid chemoprevention
Since INH chemoprevention has not been routinely implemented in Germany, a base-case probability (pPrev) that a contact individual diagnosed with LTBI will undergo INH chemoprevention of only 50% was assumed.
RESULTS
Base-case analysis
The model inputs for the test results, i.e. the probabilities of positive QFT-G results, positive TST results and previous BCG vaccination, were obtained by direct extrapolation from the real study data by normalising the ratios in table 1⇑ to a hypothetical cohort size of 1,000 contact individuals to which each strategy was applied (table 2⇑).
The costs for each strategy within a 2-yr period were assessed by utilising the decision-tree model depicted in figure 2⇑ and incorporating the data of table 2⇑. Applying the baseline criteria showed that the combined TST/QFT-G strategy is clearly less costly than the TST-alone strategy (table 3⇓). On the assumption of a 1% case-finding rate within the 2-yr time-frame, the cost of TST alone amounted to 91.06 EUR per close contact, greater than that of using QFT-G alone, which amounted to 61.29 EUR and would save 29,770 EUR per 1,000 close contacts screened in comparison to TST alone. In a combination of both test procedures, whereby the QFT-G is applied only after a positive TST result, the expenses were lowest at 52.05 EUR, a cost saving of 39.01 EUR·contact-1 compared with the TST alone, but only 9.24 EUR compared with QFT-G alone. Further restricting the QFT-G application (namely, to those contact individuals who were both TST-positive and previously BCG-vaccinated) was estimated to be slightly more expensive than the TST/QFT-G combination, due to a higher use of expensive radiographic examinations. Following the present base-case study data, applying QFT-G after a positive TST, only 20.4% of subjects would undergo the subsequent three chest radiographic examinations (table 2⇑), whereas, among TST-positive contacts in the TST/BCG/QFT-G strategy, close to 30% (20% nonvaccinated TST-positive contacts plus 10.5% vaccinated TST-positive contacts who were QFT-G-positive) would receive subsequent chest radiographic examinations. This radiography cost outweighs the higher costs of QFT-G following the TST/QFT-G strategy. Compared with the TST reference procedure, the costs here amount to 55.45 EUR, a saving of 35.61 EUR per close contact.
Economic outcomes
Sensitivity analysis
The bivariate threshold analysis of the impact of TST and QFT-G expenses on the cost relationship of the four test strategies is shown in table 4⇓. Even with continuous maximum use of a PPD vial (i.e. with application of the TST to 10 contacts·day-1) incurring costs of only 1.5 EUR per RT 23 tuberculin dose, the QFT-G could cost up to 67.8 EUR and still remain the least expensive option. Under base-case cost assumptions of 7.5 EUR per tuberculin dose, the QFT-G alone remains cost-effective compared to TST at costs of up to 73.80 EUR. Conversely, the QFT-G-alone strategy is the most economical compared with the TST/QFT-G two-step strategy only if the QFT-G price falls to 27.20 EUR.
Threshold analysis referring to base-case ranking
The TST/BCG/QFT-G screening option becomes the most economical only if there is a probability of ≥88% that the TST-positive contact individuals have also been BCG-vaccinated. When the incidence of TST-positive previously BCG-vaccinated contacts is 66%, however, the QFT-G-alone strategy would be less expensive (61.30 versus 61.60 EUR ·person-1) and becomes the second-cheapest position.
A doubling of the number of freshly detected contact individuals showing disease in the subsequent radiographic screening from 1 to 2% would hardly reduce the costs of the TST-alone screening (91.06 versus 90.94 EUR), and would, therefore, not change the relative ranking of the costs of the individual strategies. This relationship remains robust even with maximum variation in compliance with INH chemoprevention of 0–100%.
Conversely, the TST strategy becomes a more efficient alternative to the QFT-G procedure when the percentage of TST-positive individuals in the examined cohort of contact persons falls below 26%. However, a doubling of the percentage of QFT-G-positive individuals in the present cohort to 20%, with resulting screening costs of 78.50 EUR·person-1, does not change the ranking.
If the public health service were to cease performing radiographic examinations and outsource this activity to the private sector, a cost of 29.38 EUR (16.32 EUR multiplied by the customarily applied factor of 1.8 for No.5130 of the Gebührenordnung für Ärzte [Scale of Charges for Doctors] 24, the German national reimbursement catalogue) would be paid per contact examination. Taking this cost as the lower limit in the sensitivity analysis, the radiographic cost could be substantially reduced to 53.52 EUR·examination-1, but TST-based screening would remain the most expensive (table 3⇑). It should also be borne in mind that the radiologist in private practice would not perform any service apart from the radiographic examination. The organisational and counselling work involved in following-up TST- and/or QFT-G-positive contacts would still be the responsibility of the public health service, and at significant cost.
DISCUSSION
The present analysis demonstrates that the combination of the traditional TST and a new IFN-γ test in the investigation of close contacts is, from the perspective of the public health service, considerably less expensive under the base-case assumptions employed than one procedure alone. Since the number of successive chest radiographic examinations is low, application of the QFT-G for TST-positive patients is far more efficient than the TST alone, which seems comparably inexpensive at first.
More than half of the contacts (157 of 309, 50.3%) had previously been BCG vaccinated, and this was independent of their origin (German or foreign-born) and age, since BCG vaccination was recommended up to March 1998 in Germany. Recently published studies suggest most positive TST results in BCG-vaccinated individuals are false positives 21, 22, 25. However, a further differentiation in respect of BCG anamnesis does not bring additional advantages in comparison with the combination of TST and QFT-G, since, even with a high percentage of previously BCG-vaccinated contacts, the smaller fraction of TST-positive-but-BCG-unvaccinated individuals, ∼20% of TST-positive patients in the present analysis, still have to undergo the costly triple radiographic screening procedure.
Use of INH prophylaxis for only those people who are both TST- and QFT-G-positive (and considering only these as having true M. tuberculosis infection) would avoid the prescribing of unnecessary preventive treatment (with associated costs and possible side-effects) to contacts with false-positive TST responses. Using such a strategy, the cost-effectiveness of INH chemoprevention may further increase over that recently reported 9.
The present study has some limitations. It considers the best available cost data for a public health service contact investigation programme already being implemented in a major German city. An attempt was made to take into account possible differences between costs for public health and local laboratory services incurred in Hamburg and at other locations by conducting sensitivity analyses. However, these cannot take into consideration future reductions in the cost of radiographic equipment, changes in wage structures for public health service employees, or when and how cost-saving structural changes consequent upon a new screening strategy could be implemented. Indeed, although the proper question to ask from an economist’s viewpoint is not that of whether a less expensive strategy will work in practice but rather when it should be implemented, concerns about organisational convenience may also influence any decision to change the process of contact investigation. Therefore, it remains to be seen whether, in the future, the most cost-efficient strategy or a slightly more expensive but simpler procedure, in this case, the exclusive use of the QFT-G, will prevail in the diagnosis of LTBI.
The results of the present cost-minimisation analysis depend more on contributory costs than associated probabilities. However, these results depend critically on the prevalence of M. tuberculosis-infected individuals. Since the TST strategy becomes the least expensive alternative when the percentage of TST-positive individuals falls below 26% (with considerably fewer successive chest radiographic examinations), a careful differentiation between close and distant contacts may be important. A higher rate of TST-positivity would be expected with the investigation of close contacts. However, using the TST as the first screening option, and not the QFT-G, could possibly exclude a considerable number of people with false-negative TST responses but likely to be QFT-G-positive 14. This may be especially the case in immunosuppressed contacts, such as those that are HIV-positive, and thus in a community with many HIV-positive patients. The TST/QFT-G two-step strategy should be reassessed in the presence of such specific epidemiological conditions.
In conclusion, screening for tuberculosis by introducing a new whole-blood interferon-gamma test as a replacement for the tuberculin skin test, or especially by combining the tuberculin skin test and QuantiFERON-TB Gold in the investigation of close contacts, may markedly reduce public health costs compared with the current procedure of using the tuberculin skin test alone.
- Received January 26, 2006.
- Accepted March 10, 2006.
- © ERS Journals Ltd
References










